
Case Report
*Address for Correspondence: John Nguyen, MD, Department of Ophthalmology, West Virginia University, 1 Medical Center Dr., PO Box 9193, Morgantown, WV 26506-9193, USA, Tel: 304-598-6925; E-mail: nguyenj@wvuhealthcare.com
Citation: Yen-Vi Nguyen E, Nguyen J. Ophthalmoplegic “Migraine” as a Presenting Symptom of Dermoid Cyst of the Cavernous Sinus: A Case Report and Review of the Literature. J Ocular Biol. 2015;3(2): 4.
Copyright © 2015 Nguyen EY, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Ocular Biology | ISSN: 2334-2838 | Volume: 3, Issue: 1
Submission: 11 Augsut 2015 | Accepted: 27 October 2015 | Published: 02 November 2015
Reviewed & Approved by: Dr. Barrett Katz, Professor of Ophthalmology, Neurology and Neurosurgery, Montefiore Medical Center, Albert Einstein College of Medicine, USA

 He underwent a frontotemporal craniotomy with excision of the lesion. The lesion was found to be well adherent to the cavernous sinus for which drainage of the cyst content and excision of the capsule were performed. The histopathological examination revealed a keratinized squamous epithelium lined cyst containing pilosebaceous units with acellular material centrally, consistent with a dermoid cyst. The patient had resolution of all symptoms except for diplopia with upgaze at 6 months follow up.
He underwent a frontotemporal craniotomy with excision of the lesion. The lesion was found to be well adherent to the cavernous sinus for which drainage of the cyst content and excision of the capsule were performed. The histopathological examination revealed a keratinized squamous epithelium lined cyst containing pilosebaceous units with acellular material centrally, consistent with a dermoid cyst. The patient had resolution of all symptoms except for diplopia with upgaze at 6 months follow up.

The differential diagnoses of cavernous sinus lesion include neoplastic, vascular, inflammatory, infectious and granulomatous cause. Thorough assessment of other systemic symptoms and signs narrows the differential diagnosis as inflammatory, infective, and granulomatous lesions such as tuberculous, fungal infection, Wegener granulomatosis, and sarcoidosis have involvement elsewhere. These lesions typically may show linear or nodular enhancement of the meninges surrounding the cavernous sinus but often has nonspecific MRI imaging features. The differential diagnosis of cavernous cyst include trigeminal nerve schwannoma, arachnoid cyst, pyocele, cystic meningioma, colloid cyst, and hydatid cyst [16-19]. MRI findings of dermoid cyst include interdural location (originate in the lateral cavernous sinus wall), smooth contours, rounded shape, and medial displacement of the internal carotid artery. They are generally T1 hyperintense and T2 hypointense but at times may show mixed signal intensity on T2-weighted MRI. Epidermoid cysts, however, can be found of extracavernous origin with extension into the cavernous sinus, interdural or intracavernous. They appear hypointense/ isointense on T1 and hyperintense on T2. On FLAIR and high resolution T-2 weighted images, heterogenous signal intensity is seen, and there is a lack of enhancement. There is restricted diffusion with higher signal intensity than CSF on diffusion-weighted imaging [20].
Ophthalmoplegic “Migraine” as a Presenting Symptom of Dermoid Cyst of the Cavernous Sinus: A Case Report and Review of the Literature
Elena Yen-Vi Nguyen1 and John Nguyen Shahib1,2*
- 1School of Medicine, West Virginia University, Morgantown, WV, USA
- 2Department of Ophthalmology, West Virginia University, Morgantown, WV, USA
*Address for Correspondence: John Nguyen, MD, Department of Ophthalmology, West Virginia University, 1 Medical Center Dr., PO Box 9193, Morgantown, WV 26506-9193, USA, Tel: 304-598-6925; E-mail: nguyenj@wvuhealthcare.com
Citation: Yen-Vi Nguyen E, Nguyen J. Ophthalmoplegic “Migraine” as a Presenting Symptom of Dermoid Cyst of the Cavernous Sinus: A Case Report and Review of the Literature. J Ocular Biol. 2015;3(2): 4.
Copyright © 2015 Nguyen EY, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Ocular Biology | ISSN: 2334-2838 | Volume: 3, Issue: 1
Submission: 11 Augsut 2015 | Accepted: 27 October 2015 | Published: 02 November 2015
Reviewed & Approved by: Dr. Barrett Katz, Professor of Ophthalmology, Neurology and Neurosurgery, Montefiore Medical Center, Albert Einstein College of Medicine, USA
Abstract
Dermoid cysts are rarely seen at the cavernous sinus and may present with symptoms such as isolated cranial nerve palsies and headache. Ophthalmoplegic migraine has not been described as a presenting symptom. We present a case of a 27 year-old healthy man with adermoid cyst abutting the lateral wall of the cavernous sinus causing ophthalmoplegic migraine. He had resolution of symptoms after excision of the lesion. It is important to consider less common causes of migraine-like symptoms and early diagnostic imaging to minimize the potential for delay of diagnosis that can lead to significant morbidity.Keywords
Dermoid cyst, Ophthalmoplegic migraine headache, Ptosis, Diplopia, Cavernous sinus, Cranial nerve palsyIntroduction
Dermoid cysts are common congenital benign tumors that arise from entrapped embryonic epithelial nests and consisted of keratinized squamous epithelium with dermal appendages and adnexal structures, and epidermoid cysts are similar but without dermal appendages [1,2]. While subcutaneous dermoid cysts are commonly seen in children, intracranial dermoid and epidermoid cysts are rare and account for 0.04-0.7% of intracranial tumors [3]. They maybe suspected after specific or non-specific neurologic symptoms such as cranial nerve palsies, diplopia, and meningismus [2-12]. We herein report a rare case of adermoid cyst of the cavernous sinus presenting with ophthalmoplegic migraine.Case Report
A 27-year-old healthy Caucasian man presented to the Emergency Department with a 2-week history of intermittent, nonradiating, throbbing and sharp pain behind the left eye. Pain was worsened with head movement. He also complained of nausea, vertical diplopia and photophobia with each episode. The headache had been recurring for the past several years but with less intensity and frequency. He was previously treated for ocular migraine with butalbital/acetaminophen/caffeine (Fioricet - Activis, Dublin, Ireland) which brought no relief. He had no recent illness or trauma, fever, weakness, paresthesias, speech or swallowing difficulties. His past medical history was significant for Bell’s palsy 8 years prior which had resolved. The ophthalmic exam showed visual acuity of 20/20 in each eye. There was no relative afferent pupillary defect or color desaturation. External examination showed a ptotic left upper lid and left fourth nerve palsy. The remainder of the ophthalmic and neurologic examination was unremarkable. A Humphrey visual field showed left superior quadrantanopia defect (Figure 1). MRI with MRA and MRV showed a non-enhancing 1 cm cystic lesion near the left anterior clinoid process abutting the later wall of the cavernous sinus (Figure 2).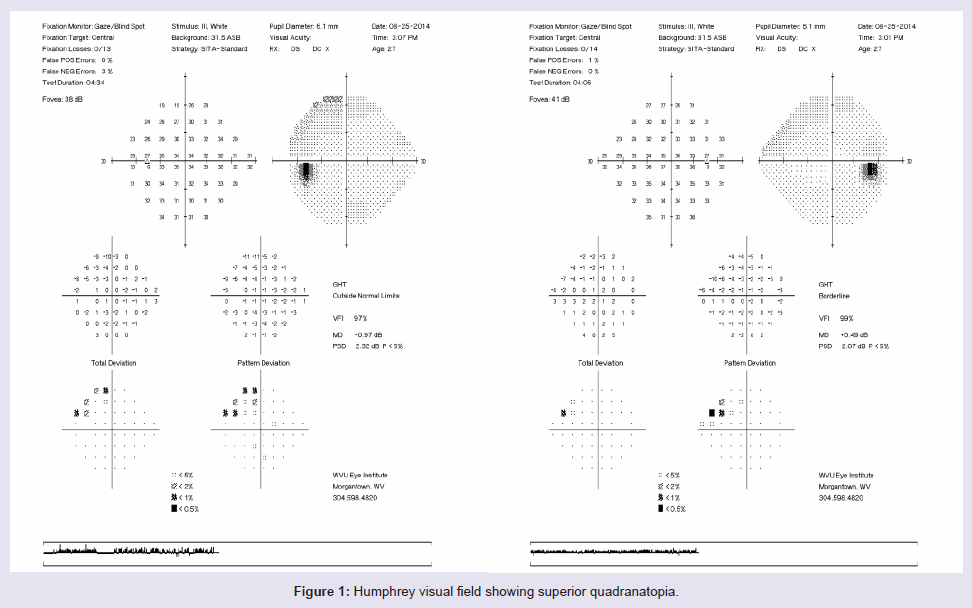
Figure 1: Humphrey visual field showing superior quadranatopia
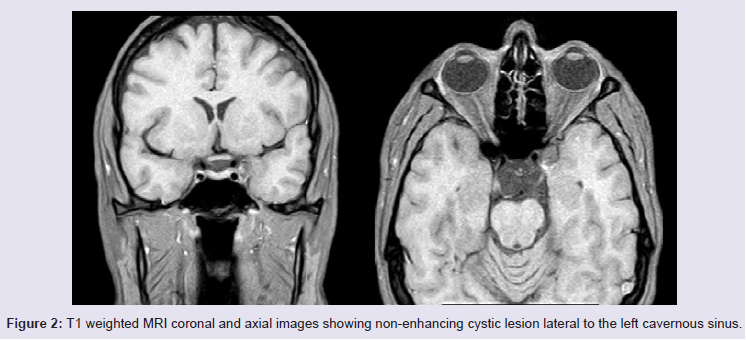
Figure 2: T1 weighted MRI coronal and axial images showing non-enhancing cystic lesion lateral to the left cavernous sinus.
Discussion
Epidermoid and dermoid cysts located in the cavernous sinus are rare. The age range of reported cases is 4-41 year old without gender predilection [2-12] (Table 1). Headache is a common presenting symptom in 50% of 12 reported cases, but there has not been a reported case of migraine-like symptoms exhibited by our patient [2,8,9,11-13]. While Rato et al. described symptoms of a tension headache in their report, other studies did not elaborate on the nature of the headaches of their patients [13]. Ophthalmoplegic migraine, also called cranial neuralgia, is defined by the International Headache Society as more than two attacks of migraine headache accompanied or followed within 4 days of its onset by paresis of one or more of the third, fourth, and/or sixth cranial nerves in the absence of any demonstrable intracranial lesion other than MRI changes within the affected nerve. Our patient exhibited symptoms of ophthalmoplegic migraine instead of ocular or retinal migraine as it is characterized by two or more attacks of monocular visual disturbance, including scintillations, scotoma or blindness, associated with migraine headache in the absence of other causes of transient monocular blindness [14]. It is likely that prior headache episodes maybe due to micro-leakage of the undiagnosed dermoid cyst as there was intraoperative findings of significant inflammation and adherence of the dermoid cyst to the cavernous sinus and adjacent tissue. Small lesions may affect adjacent cranial nerves such as CN III, CN IV as seen in our patient and also in three other reports [5-7], but larger lesions cause more serious symptoms and signs including meningismus, seizures, and isolated intracranial hypertension [9,15].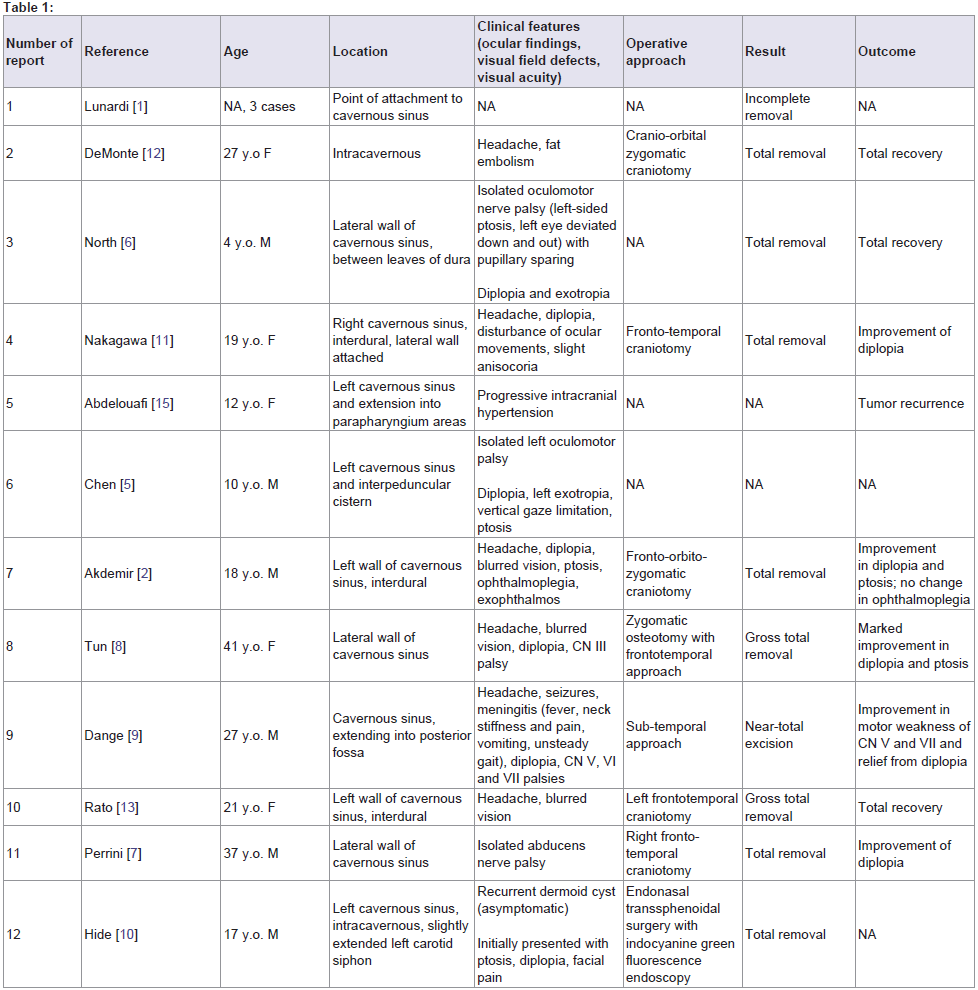
Table 1:
The treatment has been surgical excision when symptomatic. While total excision is recommended, the location and extent of these lesions poses challenges for the neurosurgeon in balancing minimization of morbidity and prevention of recurrence [1-12]. Most case reports describe improvement and resolution of presenting sign and symptoms, no long term follow up for case of near-total excision is available [9]. While ophthalmic examination is important to establish baseline findings prior to treatment, follow up ophthalmic assessment and cranial nerve exams help in early detection ofpotential recurrence.
References
- Lunardi P, Missori P (1991) Supratentorial dermoid cysts. J Neurosurg 75: 262-266.
- Akdemir G, Daglioglu E, Ergungor MF (2004) Dermoid lesion of the cavernous sinus: case report and review of the literature. Neurosurg Rev 27: 294-298.
- Yasargil MG, Abernathey CD, Sarioglu AC (1989) Microneurosurgical treatment of intracranial dermoid and epidermoid tumors. Neurosurgery 24: 561-567.
- Arseni C, Danaila L, Constantinescu AI, Carp N, Decu P (1976) Cerebral dermoid tumors. Neurochirurgia (Stuttq) 19: 104-114.
- Chen YF, Liu HM, Tu YK (2003) Dermoid cyst as a dumbbell-shaped tumour of the cavernous sinus. Pediatr Radiol 33: 72.
- North KN, Antony JH, Johnston IH (1993) Dermoid of cavernous sinus resulting in isolated oculomotor nerve palsy. Pediatr Neurol 9: 221-223.
- Perrini P, Di Russo P, Iannelli A (2013) Dermoid cyst of the lateral wall of the cavernous sinus presenting with isolated abducens nerve palsy. Acta Neurchir (Wien) 155: 741-742.
- Tun K, Celikmez RC, Okutan O, Gurcan O, Beskonakli E (2008) Dermoid tumour of the lateral wall of the cavernous sinus. J Clin Neurosci 15: 820-823.
- Dange N, Mahore A, Goel A (2010) Ruptured giant dermoid cyst of the cavernous sinus. J Clin Neurosci 17: 1056-1058.
- Hide T, Yano S, Kuratsu J (2014) Indocyanine green fluorescence endoscopy at endonasal transsphenoidal surgery for an intracavernous sinus dermoid cyst: case report. Neurol Med Chir (Tokyo) 54: 999-1003.
- Nakagawa K, Ohno K, Nojiri T, Hirakawa K (1997) Interdural dermoid cyst of the cavernous sinus presenting with oculomotor palsy: case report. No Shinkei Geka 25: 847-851.
- DeMonte F, al-Mefty O (1992) Ruptured dermoid tumor of the cavernous sinus associated with the syndrome of fat embolism: Case report. J Neurosurg 77: 312-315.
- Rato RM, Pappamikail LB, Ratilal BO, Luiz CA (2012) Dermoid tumor of the lateral wall of the cavernous sinus. Surg Neurol Int 3: 10.
- Headache Classification Committee of the International Headache Society (IHS) (2013) The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 33: 629-808.
- Abdelouafi A, Ousehal A, Gharbi A, Ait Benali S, El Kamar A, et al. (2000) Cavernous sinus dermoid cyst with unusual parapharyngeal development. J Neuroradiol 27: 140-143.
- Barr D, Kupersmith MJ, Pinto R, Turbin R (1999) Arachnoid cyst of the cavernous sinus resulting in third nerve palsy. J Neuroophthalmol 19: 249-251.
- Inui T, Okuno S (2011) Cystic meningioma originating from cavernous sinus: a case report. No Shinkei Geka 39: 877-881.
- 1Lettau M, Laible M (2011) Colloid cyst of the cavernous sinus. Rofo 183: 282-284.
- Kiresi DA, Karabacakoglu A, Odev K, Karakose S (2003) Uncommon locations of hydatid cysts. Acta Radiol 44: 622-636.
- Razek AA, Castillo M (2009) Imaging lesions of the cavernous sinus. AJNR AM J Neuroradiol 30: 444-452.