
Review Article
*Address for Correspondence: Mahmoud Rouabhia, Professor, Groupe de Recherche en Écologie Buccale, Faculté de Médecine Dentaire, Université Laval, 2420 Rue de la Terrasse, Québec, QC, G1V 0A6, Canada, Fax: 0-418-6562861; E-mail: Mahmoud.rouabhia@fmd.ulaval.ca
Citation: Rouabhia M. Advantages and Limitations of Oral Stem Cell use for Oral Tissue Replacement. J Oral Bio. 2015;2(1): 9.
Copyright © 2014 Rouabhia. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Oral Biology | ISSN: 2377-987X | Volume: 2, Issue: 1
Submission: 27 January 2015 | Accepted: 25 February 2015 | Published: 28 February 2015
Hard and soft tissue defects secondary to trauma

 Apical papilla refers to the soft tissue at the apices of developing permanent teeth [54]. Extracted and expanded in vitro, SCAP can be differentiated into a variety of cell types including odontoblasts and adipocytes [55,56]. SCAP differentiation into odontoblasts can be promoted by BMP2 [57] or bFGF [58]. SCAP was reported to express low levels of dentin sialoprotein, matrix extracellular phosphoglycoprotein, transforming growth factor β receptor II, FGFR3, VEGF receptor 1, FGFR1, and melanoma-associated glycoprotein [59]. Interestingly, SCAP express CD24 but not DPSCs. Under neurogenic stimulation, SCAP express glutamic acid decarboxylase, neuronal nuclear antigen, and neurofilament-M markers [53]. Comparative studies of DPSC and SCAP have suggested that SCAP appear to be the source of primary odontoblasts responsible for the formation of root dentin, whereas DPSCs are likely the source of replacement odontoblasts that form reparative dentin [60]. An in vivo study with mini pigs demonstrated that the removal of root apical papilla at an early development stage halted root development [61]. Although very promising to engineer dental tissue, SCAPs may not be available at a high number and throughout a patient’s lifetime. Such limitation may suggest the reduced therapeutic potential of theses SCAPs.
Apical papilla refers to the soft tissue at the apices of developing permanent teeth [54]. Extracted and expanded in vitro, SCAP can be differentiated into a variety of cell types including odontoblasts and adipocytes [55,56]. SCAP differentiation into odontoblasts can be promoted by BMP2 [57] or bFGF [58]. SCAP was reported to express low levels of dentin sialoprotein, matrix extracellular phosphoglycoprotein, transforming growth factor β receptor II, FGFR3, VEGF receptor 1, FGFR1, and melanoma-associated glycoprotein [59]. Interestingly, SCAP express CD24 but not DPSCs. Under neurogenic stimulation, SCAP express glutamic acid decarboxylase, neuronal nuclear antigen, and neurofilament-M markers [53]. Comparative studies of DPSC and SCAP have suggested that SCAP appear to be the source of primary odontoblasts responsible for the formation of root dentin, whereas DPSCs are likely the source of replacement odontoblasts that form reparative dentin [60]. An in vivo study with mini pigs demonstrated that the removal of root apical papilla at an early development stage halted root development [61]. Although very promising to engineer dental tissue, SCAPs may not be available at a high number and throughout a patient’s lifetime. Such limitation may suggest the reduced therapeutic potential of theses SCAPs.
Advantages and Limitations of Oral Stem Cell use for Oral Tissue Replacement
Mahmoud Rouabhia*
- Groupe de Recherche en Écologie Buccale, Faculté de Médecine Dentaire, Université Laval, 2420, Rue de la Terrasse, Québec, QC, G1V 0A6, Canada
*Address for Correspondence: Mahmoud Rouabhia, Professor, Groupe de Recherche en Écologie Buccale, Faculté de Médecine Dentaire, Université Laval, 2420 Rue de la Terrasse, Québec, QC, G1V 0A6, Canada, Fax: 0-418-6562861; E-mail: Mahmoud.rouabhia@fmd.ulaval.ca
Citation: Rouabhia M. Advantages and Limitations of Oral Stem Cell use for Oral Tissue Replacement. J Oral Bio. 2015;2(1): 9.
Copyright © 2014 Rouabhia. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Oral Biology | ISSN: 2377-987X | Volume: 2, Issue: 1
Submission: 27 January 2015 | Accepted: 25 February 2015 | Published: 28 February 2015
Abstract
The oral cavity is the richest stem cell source in the human body. Oral stem cells are indeed found in dental pulp, exfoliated deciduous teeth, periodontal ligaments, the apical papilla, dental follicles, gingival epithelial tissue, and gingival connective tissue. These oral stem cell populations have common cell properties including the capacity for self-renewal and multi-lineage differentiation potential giving rise to odontogenic, osteogenic, chondrogenic, adipogenic, myogenic, and neurogenic cell types. Because the oral cavity is so accessible, oral stem cell extraction is easy. These stem cells are now recognized as being vital to different types of dental tissue regeneration, such as that of dentine and periodontal ligaments following injury, thus emphasizing the potential use of these oral stem cells in regenerative medicine. This involves stem cell recruitment or seeding at the injured site, or a combination with appropriate biocompatible scaffolds for tissue engineering. Such initiatives may provide specific innovative dental tissue restoration strategies using the patient’s own oral stem cells. This review focuses on identifying the main available stem cells in the oral cavity and their potential use for basic and clinical applications. We will also highlight the potential limitations that may reduce the clinical use of oral stem cells as tissue regeneration therapy.Introduction
The superior oral cavity extends from the vermilion of the lips to the junction of the hard and soft palates, while the inferior cavity extends to the line of the tongue’s circumvallate papillae and includes the lips, upper and lower alveolar ridges, buccal mucosa, retromolartrigone, hard palate, floor of the mouth, and the anterior two-thirds of the tongue. Each structure is critical to the complex functional capacity of the oral cavity. Although oral tissues are protected, they are prone to disorders such as hard and soft tissue defects secondary to trauma (e.g., car accidents), congenital defects (e.g., cleft palate), and acquired diseases (e.g., periodontal disease, cancer) [1,2]. Oral tissue defects must be restored to improve the patient’s life and well-being.Hard and soft tissue defects secondary to trauma
Cranio maxillofacial injuries occur in a significant number of trauma patients either in isolation or in combination with other serious injuries, including cranial, spinal, and upper and lower body injuries [3,4]. The epidemiology of facial fractures varies according to type, severity, and cause as a function of the involved population [5,6]. Activities of daily life and play accidents are the leading causes of injuries along with sports, assaults, traffic accidents, and work related accidents [7-9]. Hard and soft tissue defects secondary to trauma include tooth displacement, root fracture, fracture of the anterior teeth, and soft tissue injuries.
Oral Mucosa defect secondary to periodontal disease
The importance of and need for periodontal care has been largely attributed to the significant prevalence of periodontal diseases worldwide. It has been reported that approximately 20% of the populations of most countries suffer from severe forms of periodontal disease [10,11]. In recent years, despite significant improvements in other oral pathologies such as dental caries, periodontal diseases have remained prevalent, with little decrease in terms of severity [12]. These diseases cause inflammation and the destruction of the periodontium, thus having a considerable impact on both day-today life and quality of life [13]. Severe destructive periodontitis associated with gingival recession leads to the loss of gingival tissue and underlying alveolar bone [14]. Dental tissue damage, in either its localized or generalized form, is an undesirable condition resulting in such significant health issues such as gingival mucosa damage, root exposure and resorption, tooth sensitivity, and ultimately, tooth loss [15]. Clinical interventions are intended to overcome these side effects and improve patient health.
Hard and soft tissue defects secondary to oral cancer
Oral cancer represents a high risk factor for mortality around the world [16,17]. It may involve the tongue, lips, floor of the mouth, soft palate, tonsils, salivary glands, or back of the throat. More than 90% of oral and pharyngeal cancers occur in individuals over 45 years of age [16,18]. Oral cancer is not only promoted by several exogenous insults, such as tobacco and alcohol use [19-22], but can also cause chronic pain, loss of function, and at times irreparable and socially disfiguring impairment. Following cancer treatment, maxillofacial prosthetic rehabilitation is crucial in the efforts to restore head and neck functions for the patient [23,24]. With recent advances in cancer treatment and reconstruction (e.g., the introduction of brachytherapy and microvascular free flap transfers), oral tissue rehabilitation has taken on a new dimension by providing a more acceptable quality of life for patients. Innovative techniques in surgical reconstruction thus make the maxillofacial prosthodontist’s task that much more challenging [25].
Oral tissue reconstructions
Periodontal plastic surgery is performed to prevent, correct, or eliminate anatomical, developmental, or traumatic deformities of the oral soft and hard tissues [26,27]. Multiple techniques have been proposed for oral tissue defects secondary to periodontal or cancer disease [28-30]. The rationale for these procedures is to restore oral cavity functionality and improve patient comfort and well-being. While these techniques are considered as the gold standard, by employing autologous soft and hard tissues they are neverthelesshampered by significant limitations and complications. For example, gingival recession treatment with a hard palate graft leads to an unmatched color of the implant with the neighboring native tissue. Furthermore, frequent post-operative sequels of the donor area may at times be significant [31]. In addition, many patients exhibit a minimal band of buccal keratinized tissue with several areas of gingival loss, which limits the availability of suitable tissue for grafting. This limitation can be further complicated by the presence of a small, flat palate, which also impedes the therapist’s ability to obtain an adequate amount of keratinized soft tissue to graft [32]. Other challenges include the need for a second surgical site, which prolongs the procedure, not to mention patient discomfort. In the case of oral cancer resection, large soft and hard tissues are required, which lead to a more complex clinical situation due to the deficiency of implantable autologous tissue [33]. In recent years, tissue engineering has focused on one highly challenging goal, namely, to recreate healthy functional tissue and organs to replace diseased ones [34,35].
Impact of tissue engineering in dentistry
Dental reconstructions following tissue loss are required for a large number of patients worldwide [36]. Tissue engineering seeks to devise functional and healthy soft as well as hard oral tissues to replace diseased or non-functional ones [36]. Compared to conventional grafts, tissue engineering procedures for tissue reconstruction in the oral cavity may provide significant advantages, as there is minimal or no donor site morbidity. In the field of tissue engineering of oral mucosa, naturally derived and synthetic polymers (membranes) populated with cells are being used in dentistry for tissue reconstruction [37,38]. One of the major challenges for dental tissue engineering is the use of cells that are characterized by their capacity to self-renew and to differentiate into multiple lineages. Human oral stem cells can be extracted from dental pulp, exfoliated deciduous teeth, the apical papilla, periodontal ligaments, dental follicle progenitor cells, gingival connective tissue, and gingival epithelial tissue.
Oral Stem Cells
Pulp stem cells and tissue engineering
It is now well established that dental pulp contains stem cells which are activated upon tooth injury leading to cell growth and differentiation to repair tooth damage [39]. Dental pulp contains several stem cell niches localized predominantly in the perivascular area of the pulpal cavity and ready to restore the damaged area [40]. Dental pulp is crucial to tooth homeostasis; loss of this pulp is without question associated with tooth fracture and periapical disease leading to tooth loss [41,42]. To avoid this situation, one may think of pulp regeneration as including important key players [43,44] regenerated dental pulp must be vascularized; the differentiated stem cells must be supported by the existing dentinal wall of the root canal space; and the newly regenerated tissue must adequately interact with the existing dentin [43,44].
A number of research groups have attempted to engineer pulp tissue replacements similar to normal pulp tissue for use in such regenerative endodontic procedures as pulp stem cell extraction, growth and differentiation, and in vitro tissue engineering. Dental pulp stem cells (DPSCs) can be differentiated, resulting in a dentin pulp-like complex that includes mineralized matrix and odontoblasts [44,45]. DPSCs were reported to differentiate into multi-cell lineages, such as adipocytes, neural-like cells, and osteoblasts [46,47]. We were able to extract stem cells from dental pulp, culture and differentiate them onto osteoblast-like cell-generating bone nodules, as shown in Figure 1. To promote bone tissue formation, we also combined DPSCs with an osteogenic porous scaffold to demonstrate in vitro this bone tissue formation (Figure 2). Animal studies also showed in vivo bone tissue formation following dental pulp cell differentiation into osteoblasts than implementation [48]. These studies suggest the potential use of dental pulp stem cells to restore dentin and bone defects in humans. However, the major limit using these DPSCs for clinical therapies is the available throughout a patient’s lifetime. As this availability is basically greater at an early age, DPSCs banking may constitute a potential solution by cryopreserving the cells for future clinical use. Such solution may not be useful for all around the world.
Exfoliated deciduous teeth stem cells
Replacement of deciduous teeth by adult permanent teeth is a dynamic process that combines the resorption of deciduous root and its detachment from the mandibular under the pressure of the permanent teeth. Exfoliated deciduous teeth can be used to collect the remaining dental pulp tissue. This has been reported to be rich in stem cells. Extracted and cultured in vitro, deciduous teeth stem cells were shown to display a faster proliferation rate compared to that of dental pulp stem cells [49]. They can also differentiate into odontoblasts, osteoblasts, adipocytes, neural cells, etc. [50]. Interestingly, these exfoliated deciduous teeth stem cells are regarded as immature dental pulp stem cells expressing embryonic stem cell markers Oct4, stage-specific embryonic antigens (SSEA-3, SSEA-4), and tumor-recognition antigens (TRA-1-60 and TRA-1-81) [51]. In vivo grafting of these cells in a mouse model showed the formation of dentin [49]. When used in critical-sized bone defects in mouse calvarias, these cells demonstrated bone repair [52]. Based on these cell properties, we hypothesize that exfoliated deciduous teeth stem cells can be introduced in vivo as autologous or allogeneic grafts, thus exfoliated deciduous teeth may constitute a feasible cell source for dental regenerative medicine. However, the use of these stem cells as autologous implementation may not be applicable throughout a patient’s lifetime.
Apical papilla stem cells
Stem cells from the apical papilla (SCAP) refer to mesenchymal stem cells residing in the apical papilla of underdeveloped teeth [53].
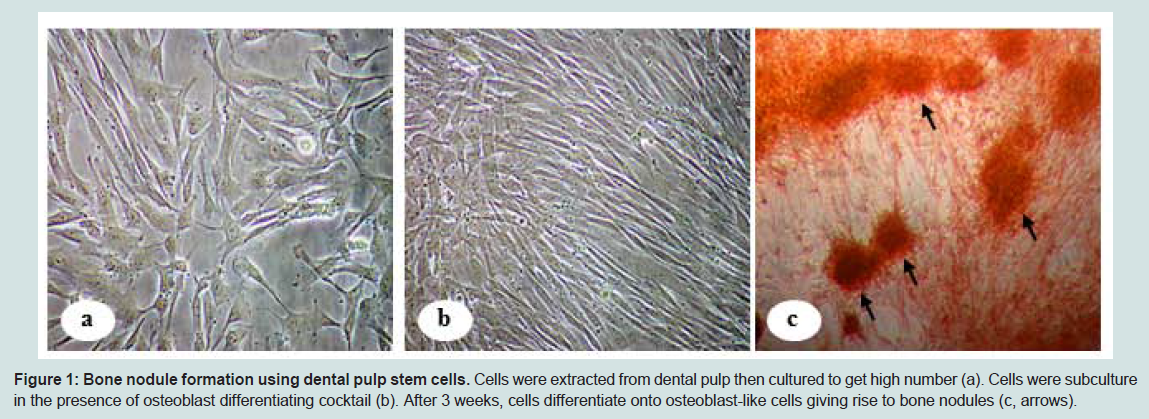
Figure 1: Bone nodule formation using dental pulp stem cells. Cells were extracted from dental pulp then cultured to get high number (a). Cells were subculture in the presence of osteoblast differentiating cocktail (b). After 3 weeks, cells differentiate onto osteoblast-like cells giving rise to bone nodules (c, arrows).
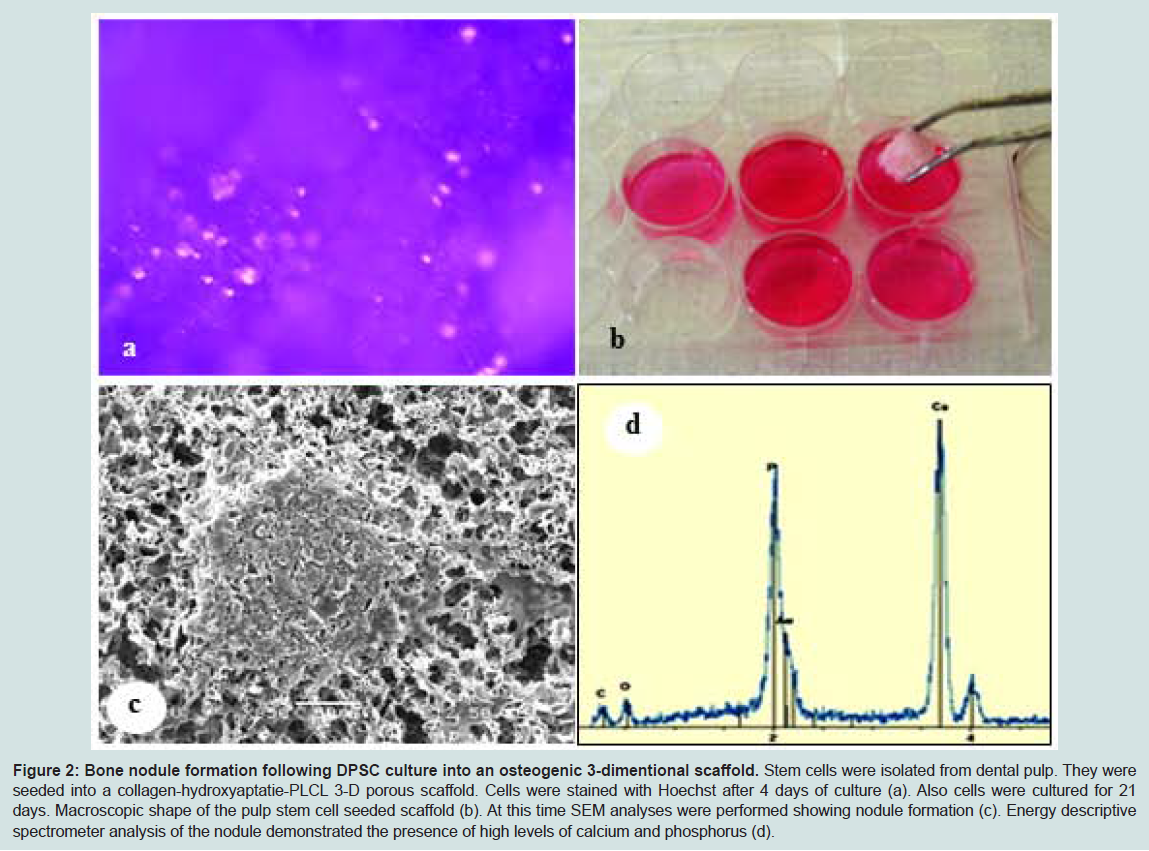
Figure 2: Bone nodule formation following DPSC culture into an osteogenic 3-dimentional scaffold. Stem cells were isolated from dental pulp. They were seeded into a collagen-hydroxyaptatie-PLCL 3-D porous scaffold. Cells were stained with Hoechst after 4 days of culture (a). Also cells were cultured for 21 days. Macroscopic shape of the pulp stem cell seeded scaffold (b). At this time SEM analyses were performed showing nodule formation (c). Energy descriptive spectrometer analysis of the nodule demonstrated the presence of high levels of calcium and phosphorus (d).
Dental follicle progenitor cells
The dental follicle is an ecto-mesenchymal tissue that surrounds the developing tooth germ [62,63]. During tooth root formation, periodontal components, such as cementum, periodontal ligaments (PDL), and alveolar bone derive from the differentiation of dental follicle stem cells [62,63]. Phenotyping of cells extracted from the dental follicle showed the expression of Notch1, STRO-1, nestin, collagen type I, bone sialoprotein (BSP), osteocalcin (OCN), and fibroblast growth factor receptor 1-IIIC [64]. Dental follicle stem cells (DFSCs) can be differentiated into osteoblasts, cementoblasts, adipocytes, and neurons [65,66]. Human BMP-2 and BMP-7 were shown to increase BMP-2 and BMP-7 expression by dental follicle stem cells [65]. in vivo studies demonstrated that dental follicle stem cells were able to form periodontal ligament (PDL)-like tissue [66]. In vivo generated tissue was found to express high levels of humanspecific transcripts for BSP and OCN, but a low level of collagen type I [64]. Overall data therefore suggest that dental follicle stem cells may be a useful research tool for regenerating/restoring PDL formation, thus representing an important regenerative therapy. However, the collection of these cells or tissue containing a significant amount of DFSCs may not be easy, due to the limited volume and the need of this tissue to support the regeneration of cementum, PDL, and alveolar bone [62,63].
Periodontal ligament stem cells
The periodontal ligament (PDL) is a key dental tissue of the tooth. It suspends the tooth in its bony socket (the alveolus proper) and supplies nutrients to both the alveolus and the cementum to maintain tooth homeostasis [67]. Structural and or functional deregulations of the periodontal tissue often result in alveolar bone resorption leading eventually to tooth loss [68]. Earlier studies reported that PDL contained progenitor cells that maintain the homeostasis and regeneration of periodontal tissue [69,70]. Specifically, PDL houses a population of clonogenic cells that display the characteristics of post-natal stem cells [71,72]. Following extraction and in vitro culture, cell phenotyping demonstrated that PDL stem cells expressed CD105, CD90, CD44, and CD73, but not CD45, CD31, and CD34. Under the appropriate culture conditions, PDL stem cells can be differentiated into osteoblasts, chondrocytes, and adipocytes [73,74]. Multiple growth factors contribute to PDL stem cell differentiation into multiple cells types. in vitro studies have shown the efficacy of basic fibroblast growth factor 2 (FGF-2) in periodontal tissue regeneration [75]. FGF-2 modulates the activity of various cell types by promoting fibroblast and osteoblast proliferation, in addition to enhancing angiogenesis. These activities are directly associated with periodontal tissue regeneration [75]. FGF-2 promotes the expression of FGFR1 and FGFR2 by periodontal ligament stem cells [76]. The responsiveness to FGF-2 was also shown to be higher in PDL stem cells than in mature periodontal ligament cells [77]. These in vitro data were confirmed in vivo with an animal model showing that local application of FGF-2 promoted periodontal regeneration in both dog and primate models [78,79]. We have learned from in vivo studies that PDLSCs possess unique properties to form a cementum/periodontal ligament complex-like structure when introduced into an animal model [71]. Structural analysis of the in vivo regenerated tissue showed a dense type I collagen-positive PDL-like tissue within the transplants. Interestingly, in another study, the generated collagen fibers were shown to interact with the newly formed cementum-like structures and to mimic the physiological attachment of Sharpey’s fibers [80]. These findings suggest the possible differentiation of PDL stem cells into cementoblasts/cementocytes and collagen-forming cells in vivo. Furthermore, the graft of human PDL stem cells in immune compromised mice to restore periodontal defects resulted in the formation of PDL-like tissue. Moreover, human PDL stem cells were found to be closely associated with the trabecular bone next to the regenerated PDL. These data indicate a contribution of PDL stem cells to alveolar bone regeneration [80-83]. Overall data therefore suggest that PDLSCs are ideal cell sources for cell-based periodontal therapies. Tissue inaccessibility may, however limit the potential use of these PDLSCs for clinical applications.
Gingival mucosa stem cells
(a) Stem cells in human gingival epithelium: Adult or tissuespecific stem cells have been identified in various tissues, including the hematopoietic system, corneal epithelium, neural crest, and gingival mucosa. Inside these tissues, stem cells are associated with a specialized environment that provides key signals to guide stem cell function [84,85]. In the gingival epithelium, epithelial stem cells are involved in self-renewal and multi-potency. Indeed, one stem cell goes under asymmetrical division giving rise to two cells; one will remain with the same stem cell characteristics as the progenitor. The other one will undergo several proliferation rounds forming the different strata of the epithelial tissue before terminal differentiation [86,87]. Gingival epithelium can be subdivided into different layers (basal, suprabasal, superficial). Epithelial stem cells are located in the basal layer of the gingival epithelium. In normal tissue, epithelial stem cells are quiescent or slow-cycling cells [88]. Cell phenotyping has shown that epithelial stem cells express the following stem cell markers: α6 and β1 integrins, keratins 15 and 19, p63, α6β4, oct3/4, CD44H, p75, ATP-binding cassette subfamily G member 2 and K5 [89]. When needed, under specific stimulation, epithelial stem cells undergo phenotype to become first a supra basal cell layer, then superficial epithelial cells [1,89]. Extraction and in vitro subculture of epithelial gingival stem cells showed elevated clonogenicity and proliferative capacity [90].
These properties have led us to engineer oral mucosa epithelium to be used for basic and clinical applications (Figure 3). Indeed, under appropriate culture conditions, these gingival epithelial stem cells proliferated and stratified to form a three-dimensional gingival epithelium [91,92]. Engineered oral mucosal epithelial cell sheets were shown to be safe and effective for corneal and esophageal epithelium reconstructions [93,94]. This evidence thus suggests that oral epithelial stem cells have the capacity to repair damaged epithelial tissues in the human body.
epithelium reconstructions [93,94]. This evidence thus suggests that oral epithelial stem cells have the capacity to repair damaged epithelial tissues in the human body.
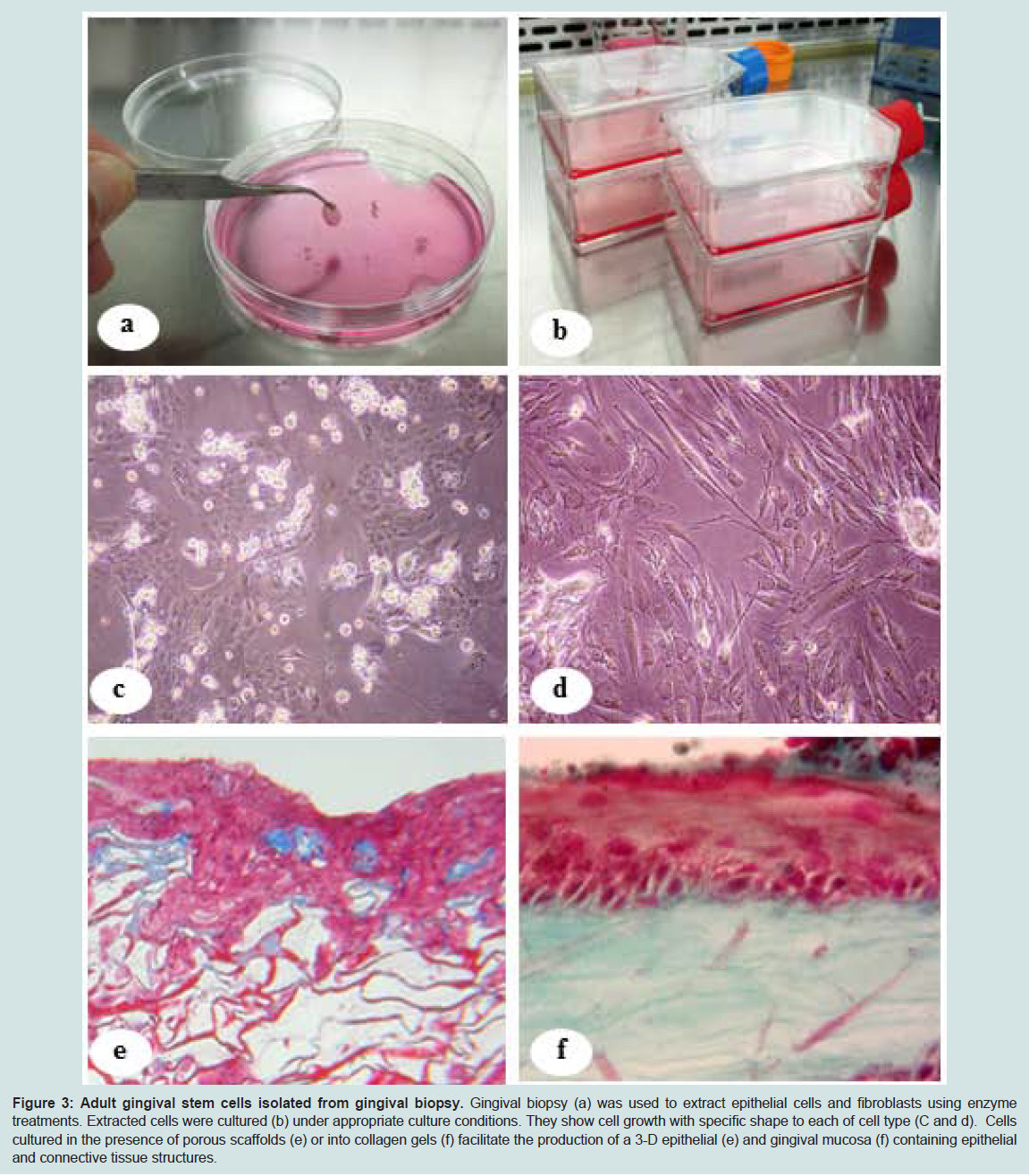
Figure 3: Adult gingival stem cells isolated from gingival biopsy. Gingival biopsy (a) was used to extract epithelial cells and fibroblasts using enzyme treatments. Extracted cells were cultured (b) under appropriate culture conditions. They show cell growth with specific shape to each of cell type (C and d). Cells cultured in the presence of porous scaffolds (e) or into collagen gels (f) facilitate the production of a 3-D epithelial (e) and gingival mucosa (f) containing epithelial and connective tissue structures.
Gingival epithelial stem cells may be combined with gingival fibroblasts to engineer native-like gingival mucosa tissue. We demonstrated that when interacting with gingival fibroblasts through a 3-D collagen scaffold, gingival epithelial stem cells produced a wellstructured, stratified gingival mucosa tissue (Figure 3). This was used for in vitro and in vivo basic research to demonstrate its usefulness as a promising strategy for dental tissue regeneration. Gingival epithelium is the most accessible tissue in the oral cavity. This guarantees the availability of stem cells extract from the epithelium throughout a patient’s lifetime. Moreover, stem cell banking may not be needed thanks to the possibility to harvest gingival tissue at any time and extract the stem cells for basic and /or clinical use.
(b) Stem cells in human gingival connective tissue (lamina propria): Multiple experimental procedures have demonstrated that oral mucosal connective tissues originate embryonically from the cranial neural crest [84]. With this distinct developmental origin, cells present in the oral mucosal connective tissue have a specific gene expression profile compared to that of skin cells [95]. The multipotent differentiation potential of mesenchymal stromal cells from oral connective tissue is comparable to that of cells isolated from skin dermis and bone marrow [96]. Phenotypically, human gingivalconnective tissue stem cells express CD44, CD73, CD90 and CD105 [97]. Human gingival connective tissue MSCs can undergo specific differentiation to produce tooth matter and periodontal tissue when placed in an extra-oral niche [84]. in vitro and in vivo studies have shown a possible PDL regeneration using human gingival stem cells [81,83] present in gingival connective tissue.
Gingival connective tissue stem cells were found to display a significant self-renewal capacity and a higher proliferation rate compared to BMSCs [98-100]. With this elevated proliferation capacity, it then becomes possible to grow cells and to engineer in vitro connective tissue following the combination of cells with extracellular matrix. As shown in Figure 3f, it is possible to seed a collagen gel matrix with gingival connective tissue mesenchymal stem cells to produce gingival connective tissue in vitro [101]. This engineered tissue can subsequently be used for in vitro and in vivo studies [92,102,103]. Of interest is that human gingival connective tissue MSCs can be differentiated into osteoblasts, adipocytes, and chondrocytes [100,104,105]. In vivo use of a biocompatible scaffold populated with gingival connective tissue MSCs was shown to generate various tissues, such as connective tissue-like structures [100,104] or bone matrix [99,106]. Thus gingival connective tissue as well as gingival epithelium may constitute potential stem cell supply sources with the advantage of being accessible at all times during the patient’s lifetime, thereby allowing for safe, non-invasive tissue and cell collections for cell/tissue therapies.
Conclusion
The potential for the clinical applications of stem cells to restore damaged human tissue is highly attractive. Having access to stem cell sources is a key step in the design and use of engineered tissue for regenerative medicine. The oral cavity, the most accessible stem cell source in the human body, houses different stem cell niches. in vitro studies have not only confirmed the usefulness of the oral stem cells for tissue production but have been supported by a plethora of animal studies, providing an overwhelming body of evidence to support the significant potential of oral stem cells for dental tissue regeneration applications. Some human clinical trials have used oral stem cells for the regeneration of corneas, dental pulp, and bone. Appropriate double-blind randomized clinical trials are still to be performed to confirm the true regenerative power of these stem cells. Through further clinical research, multiple key parameters should be optimized; including the required stem cell density and availability as well as appropriate strategies for their use (either alone or in combination with scaffolds, site injection, etc.). The other major issue regarding the clinical use of oral stem cells is the availability of the cells over time. For example, dental pulps stem cells or exfoliated deciduous tooth stem cells are not available throughout a patient’s lifetime. As this availability is basically greater at an early age, oral stem cell banking may constitute a potential solution by cryopreserving these oral stem cells for future clinical use. However, such a possibility is not only time-consuming and costly but limits the use of some oral stem cells as a clinical strategy. The use of oral stem cells for dental tissue regeneration is nonetheless an important biotechnological innovation with the potential of providing significant benefits to overcome the effects of dental diseases.References
- Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T (2014) Aetiology of maxillofacial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 52: 901-906.
- Gladwell M, Viozzi C (2008) Temporal bone fractures: a review for the oral and maxillofacial surgeon. J Oral Maxillofac Surg 66: 513-522.
- Hussain K, Wijetunge DB, Grubnic S, Jackson IT (1994) A comprehensive analysis of craniofacial trauma. J Trauma 36: 34-47.
- Oikarinen KS (1995) Clinical management of injuries to the maxilla, mandible, and alveolus. Dent Clin North Am 39: 113-131.
- Haug RH, Prather J, Indresano AT (1990) An epidemiologic survey of facial fractures and concomitant injuries. J Oral Maxillofac Surg 48: 926-932.
- Girotto JA, MacKenzie E, Fowler C, Redett R, Robertson B, Manson PN (2001) Long-term physical impairment and functional outcomes after complex facial fractures. Plast Reconstr Surg 108: 312-327.
- Gopalakrishna G, Peek-Asa C, Kraus JF (1998) Epidemiologic features of facial injuries among motorcyclists. Ann Emerg Med 32: 425-430.
- Hogg NJ, Stewart TC, Armstrong JE, Girotti MJ (2000) Epidemiology of maxillofacial injuries at trauma hospitals in Ontario, Canada between 1992 and 1997. J Trauma 49: 425-432.
- Iida S, Kogo M, Sugiura T, Mima T, Matsuya T (2001) Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg 30: 286-290.
- Needleman I, McGrath C, Floyd P, Biddle A (2004) Impact of oral health on the life quality of periodontal patients. J Clin Periodontol 31: 454-457.
- Hugoson A, Laurell L (2000) A prospective longitudinal study on periodontal bone height changes in a Swedish population. J Clin Periodontol 27: 665-674.
- Downer M C (1998) The changing pattern of dental disease over 50 years. Br Dent J 185: 36-41.
- Locker D (1988) Measuring oral health: a conceptual framework. Community Dent Health 5: 3-18.
- Brown LJ, Loe H (1993) Prevalence, extent, severity and progression of periodontal disease. Periodontol 2000 2: 57-71.
- Needleman IG, Worthington HV, Giedrys-Leeper E, Tucker RJ (2006) Guided tissue regeneration for periodontal infra-bony defects. Cochrane Database Syst Rev Apr 19: CD001724.
- Boring CC, Squires TS, Tong T, Montgomery S (1994) Cancer statistics. CA Cancer J Clin 44: 7-26.
- East SC, Stocker JL, Avery BS (2005) Is the two week rule of any benefit to patients with oral cancer? Br J Oral Maxillofac Surg 43: 511-512.
- Baden E (1987) Prevention of cancer of the oral cavity and pharynx. Cancer 37: 49-62.
- Shillitoe EJ, Greenspan D, Greenspan JS, Silverman S Jr (1986) Five-year survival of patients with oral cancer and its association with antibody to herpes simplex virus. Cancer 58: 2256-2259.
- National Cancer Institute (1989) Cancer statistics review 1973-1987. Washington, DC: US Department of Health and Human Services, National Institutes of Health, National Cancer Institute, NIH publication no (NIH) 88-2789.
- Boffetta P, Mashberg A, Winkelmann R, Garfinkel L (1992) Carcinogenic effect of tobacco smoking and alcohol drinking on anatomic sites of the oral cavity and oropharynx. Int J Cancer 52: 530-533.
- Blot WJ, McLaughlin JK, Winn DM, Austin DF, Greenberg RS, et al. (1988) Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res 48: 3282-3287.
- Beumer J, DePaola LG, Leupold RJ (1986) Prosthetic management. In: Peterson DE, Elias EG, Sonis ST, eds. Head and neck management of the cancer patient. Boston: Martinus Nijhoff Publishers 453-478.
- Toljanic JA, Eckert SE, Roumanas E, Beumer J, Huryn JM, et al. (2005) Osseointegrated craniofacial implants in the rehabilitation of orbital defects: an update of a retrospective experience in the United States. J Prosthet Dent 94: 177-182.
- Yadav P (2014) Recent advances in head and neck cancer reconstruction. Indian J Plast Surg 47: 185-190.
- Dace B (2003) Periodontal plastic surgery. Northwest Dent 82: 33-34.
- Cairo F, Nieri M, Pagliaro U (2014) Efficacy of periodontal plastic surgery procedures in the treatment of localized facial gingival recessions. A systematic review. J Clin Periodontol 41: S44-S62.
- Short JM (1999) Root coverage using a subepithelial connective tissue graft and rotational flaps in the mandibular posterior region. N M Dent J 50: 8-11.
- Pini Prato GP, Baldi C, Nieri M, Franseschi D, Cortellini P, et al. (2005) Coronally advanced flap: the post-surgical position of the gingival margin is an important factor for achieving complete root coverage. J Periodontol 76: 713-722.
- Villar CC, Cochran DL (2010) Regeneration of periodontal tissues: guided tissue regeneration. Dent Clin North Am 54: 73-92.
- McGuire MK, Scheyer ET, Nunn ME, Lavin PT (2008) A pilot study to evaluate a tissue-engineered bilayered cell therapy as an alternative to tissue from the palate. J Periodontol 79: 1847-1856.
- Lorenzana ER, Allen EP (2000) The single-incision palatal harvest technique: a strategy for esthetics and patient comfort. Int J Periodontics Restorative Dent 20: 297-305.
- Deneve JL, Turaga KK, Marzban SS, Puleo CA, Sarnaik AA, et al. (2013) Single-institution outcome experience using AlloDerm® as temporary coverage or definitive reconstruction for cutaneous and soft tissue malignancy defects. Am Surg 79: 476-482.
- Platt JL, Cascalho M (2013) New and old technologies for organ replacement. Curr Opin Organ Transplant 18: 179-185.
- Hanauer N, Latreille PL, Alsharif S, Banquy X (2015) 2D, 3D and 4D Active Compound Delivery in Tissue Engineering and Regenerative Medicine. Curr Pharm Des [Epub ahead of print].
- Balaji SM (2014) Craniofacial reconstruction and stem cell engineering. Ann Maxillofac Surg 4: 127.
- Sieira Gil R, Pagés CM, Díez EG, Llames S, Fuertes AF, et al. (2015) Tissue-engineered oral mucosa grafts for intraoral lining reconstruction of the maxilla and mandible with a fibula flap. J Oral Maxillofac Surg 73: 195.e1-195.e16.
- Earthman JC, Sheets CG, Paquette JM, Kaminishi RM, Nordland WP, et al. (2003) Tissue engineering in dentistry. Clin Plast Surg 30: 621-639.
- Gronthos S, Mankani M, Brahim J, Robey PG, Shi S (2000) Postnatal human dental pulp stem cells (DPSCs) in vitro and in vivo. Proc Natl Acad Sci U S A 97: 13625-13630.
- Lizier NF, Kerkis A, Gomes CM, Hebling J, Oliveira CF, et al. (2012) Scaling-up of dental pulp stem cells isolated from multiple niches. PLoS One 7: e39885.
- Romanos GE, Papadimitriou DE, Hoyo MJ, Caton JG (2014) Loss of pulp vitality after maxillary sinus augmentation: a surgical and endodontic approach. J Periodontol 85: 43-49.
- Yu C, Abbott PV (2007) An overview of the dental pulp: its functions and responses to injury. Aust Dent J 52: S4-S16.
- Huang GT (2009) Pulp and dentin tissue engineering and regeneration: current progress. Regen Med 4: 697-707.
- Tatullo M, Marrelli M, Shakesheff KM, White LJ (2014) Dental pulp stem cells: function, isolation and applications in regenerative medicine. J Tissue Eng Regen Med [Epub ahead of print].
- Sun HH, Jin T, Yu Q, Chen FM (2011) Biological approaches toward dental pulp regeneration by tissue engineering. J Tissue Eng Regen Med 5: 1-16.
- La Noce M, Paino F, Spina A, Naddeo P, Montella R, et al. (2014) Dental pulp stem cells: state of the art and suggestions for a true translation of research into therapy. J Dent 42: 761-768.
- Akkouch A, Zhang Z, Rouabhia M (2014) Engineering bone tissue using human dental pulp stem cells and an osteogenic collagen-hydroxyapatite-poly (L-lactide-co-ε-caprolactone) scaffold. J Biomater Appl 28: 922-936.
- Janebodin K, Horst OV, Ieronimakis N, Balasundaram G, Reesukumal K, et al. (2011) Isolation and characterization of neural crest-derived stem cells from dental pulp of neonatal mice. PLoS One 6: e27526.
- Miura M, Gronthos S, Zhao M, Lu B, Fisher LW, et al. (2003) SHED: stem cells from human exfoliated deciduous teeth. Proc Natl Acad Sci U S A 100: 5807-5812.
- Nowwarote N, Pavasant P, Osathanon T (2015) Role of endogenous basic fibroblast growth factor in stem cells isolated from human exfoliated deciduous teeth. Arch Oral Biol 60: 408-415.
- Kerkis I, Kerkis A, Dozortsev D, Stukart-Parsons GC, Gomes Massironi SM, et al. (2006) Isolation and characterization of a population of immature dental pulp stem cells expressing OCT-4 and other embryonic stem cell markers. Cells Tissues Organs 184: 105-116.
- Seo BM, Sonoyama W, Yamaza T, Coppe C, Kikuiri T, et al. (2008) SHED repair critical-size calvarial defects in mice. Oral Dis 14: 428-434.
- Sonoyama W, Liu Y, Yamaza T, et al (2008) Characterization of the apical papilla and its residing stem cells from human immature permanent teeth: a pilot study. J Endod 34: 166-171.
- Sonoyama W, Liu Y, Fang D, Yamaza T, Seo BM, et al. (2006) Mesenchymal stem cell-mediated functional tooth regeneration in Swine. PLoS One e79.
- Vanacker J, Viswanath A, De Berdt P, Everard A, Cani PD, et al. (2014) Hypoxia modulates the differentiation potential of stem cells of the apical papilla. J Endod 40: 1410-1418.
- Abe S, Yamaguchi S, Amagasa T (2007) Multilineage cells from apical pulp of human tooth with immature apex. Oral Sci Int 4: 45-58.
- Zhang W, Zhang X, Ling J, Liu W, Zhang X, et al. (2014) Proliferation and odontogenic differentiation of BMP2 gene transfected stem cells from human tooth apical papilla: an in vitro study. Int J Mol Med 34: 1004-1012.
- Wu J, Huang GT, He W, Wang P, Tong Z, et al. (2012) Basic fibroblast growth factor enhances stemness of human stem cells from the apical papilla. J Endod 38: 614-622.
- Bakopoulou A, Leyhausen G, Volk J, Koidis P, Geurtsen W (2013) Comparative characterization of STRO-1(neg)/CD146(pos) and STRO 1(pos)/CD146(pos) apical papilla stem cells enriched with flow cytometry. Arch Oral Biol 58: 1556-1568.
- Huang GT, Sonoyama W, Liu Y, Liu H, Wang S, et al. (2008) The hidden treasure in apical papilla: the potential role in pulp/dentin regeneration and bioroot engineering. J Endod 34: 645-651.
- Lang H, Schüler N, Nolden R (1998) Attachment formation following replantation of cultured cells into periodontal defects -a study in minipigs. J Dent Res 77: 393-405.
- Rezai Rad M, Liu D, He H, Brooks H, Xiao M, et al. (2015) The role of dentin matrix protein 1 (DMP1) in regulation of osteogenic differentiation of rat dental follicle stem cells (DFSCs). Arch Oral Biol 60: 546-556.
- Yokoi T, Saito M, Kiyono T, Iseki S, Kosaka K, et al. (2007) Establishment of immortalized dental follicle cells for generating periodontal ligament in vivo. Cell Tissue Res 327: 301-311.
- Morsczeck C, Gotz W, Schierholz J, Zeilhofer F, Kuhn U, et al. (2005) Isolation of precursor cells (PCs) from human dental follicle of wisdom teeth. Matrix Biol 24: 155-165.
- Kémoun P, Laurencin-Dalicieux S, Rue J, Farges JC, Gennero I, et al. (2007) Human dental follicle cells acquire cementoblast features under stimulation by BMP-2/-7 and enamel matrix derivatives (EMD) in vitro. Cell Tissue Res 329: 283-294.
- Liu J, Wang L, Liu W, Li Q, Jin Z, et al. (2014) Dental follicle cells rescue the regenerative capacity of periodontal ligament stem cells in an inflammatory microenvironment. PLoS One 9: e108752.
- Gartner LP (1989) Oral Histology and Embryology. Baltimore, MD: Williams and Wilkins.
- Racz GZ, Kadar K, Foldes A, Kallo K, Perczel-Kovach K, et al. (2014) Immunomodulatory and potential therapeutic role of mesenchymal stem cells in periodontitis. J Physiol Pharmaco l65: 327-339.
- McCulloch CA, Bordin S (1991) Role of fibroblast subpopulations in periodontal physiology and pathology. J Periodontal Res 26: 144-154.
- Isaka J, Ohazama A, Kobayashi M, Nagashima C, Takiguchi T, et al. (2001) Participation of periodontal ligament cells with regeneration of alveolar bone. J Periodontol 72: 314-323.
- Bright R, Hynes K, Gronthos S, Bartold PM (2014) Periodontal ligament-derived cells for periodontal regeneration in animal models: a systematic review. J Periodontal Res [Epub ahead of print].
- Chamila Prageeth Pandula PK, Samaranayake LP, Jin LJ, Zhang C (2014) Periodontal ligament stem cells: an update and perspectives. J Investig Clin Dent 5: 81-90.
- Saito MT, Salmon CR, Amorim BR, Ambrosano GM, Casati MZ, et al. (2014) Characterization of highly osteoblast/cementoblast cell clones from a CD105-enriched periodontal ligament progenitor cell population. J Periodontol 85: e205-211.
- Trubiani O, Zalzal SF, Paganelli R, Marchisio M, Giancola R, et al. (2010) Expression profile of the embryonic markers nanog, OCT-4, SSEA-1, SSEA-4, and frizzled-9 receptor in human periodontal ligament mesenchymal stem cells. J Cell Physiol 225: 123-131.
- Kao RT, Murakami S, Beirne OR (2009) The use of biologic mediators and tissue engineering in dentistry. Periodontol 2000 50: 127-153.
- Takayama S, Yoshida J, Hirano H, Okada H, Murakami S (2002) Effects of basic fibroblast growth factor on human gingival epithelial cells. J Periodontol 73: 1467-1473.
- Hasegawa T, Chosa N, Asakawa T, Yoshimura Y, Fujihara Y, et al. (2012) Differential effects of TGF-β1 and FGF-2 on SDF-1α expression in human periodontal ligament cells derived from deciduous teeth in vitro. Int J Mol Med 30: 35-40.
- Murakami S, Takayama S, Kitamura M, Shimabukuro Y, Yanagi K, et al. (2003) Recombinant human basic fibroblast growth factor (bFGF) stimulates periodontal regeneration in class II furcation defects created in beagle dogs. J Periodontal Res 38: 97-103.
- Takayama S, Murakami S, Shimabukuro Y, Kitamura M, Okada H (2001) Periodontal regeneration by FGF-2 (bFGF) in primate models. J Dent Res 80: 2075-2079.
- Huang GT, Gronthos S, Shi S (2009) Mesenchymal stem cells derived from dental tissues vs. those from other sources: their biology and role in regenerative medicine. J Dent Res 88: 792-806.
- Yang H, Gao LN, An Y, Hu CH, Jin F, et al. (2013) Comparison of mesenchymal stem cells derived from gingival tissue and periodontal ligament in different incubation conditions. Biomaterials 34: 7033-7047.
- Moshaverinia A, Chen C, Xu X, Akiyama K, Ansari S, et al. (2014) Bone regeneration potential of stem cells derived from periodontal ligament or gingival tissue sources encapsulated in RGD-modified alginate scaffold. Tissue Eng Part A 20: 611-621.
- Yu X, Ge S, Chen S, Xu Q, Zhang J, et al. (2013) Human gingiva-derived mesenchymal stromal cells contribute to periodontal regeneration in beagle dogs. Cells Tissues Organs 198: 428-437.
- Angelova Volponi A, Kawasaki M, Sharpe PT (2013) Adult human gingival epithelial cells as a source for whole-tooth bioengineering. J Dent Res 92: 329-334.
- Calenic B, Ishkitiev N, Yaegaki K, Imai T, Costache M, et al. (2010) Characterization of oral keratinocyte stem cells and prospects of its differentiation to oral epithelial equivalents. Rom J Morphol Embryol 51: 641-645.
- Lechler T, Fuchs E (2005) Asymmetric cell divisions promote stratification and differentiation of mammalian skin. Nature 437: 275-280.
- Kirschner M, Montazem A, Hilaire HS, Radu A (2006) Long-term culture of human gingival keratinocyte progenitor cells by down-regulation of 14-3-3 sigma. Stem Cells Dev 15: 556-565.
- Nakamura T, Endo K, Kinoshita S (2007) Identification of human oral keratinocyte stem/progenitor cells by neurotrophin receptor p75 and the role of neurotrophin/p75 signaling. Stem Cells 25: 628-638.
- Jones KB, Klein OD (2013) Oral epithelial stem cells in tissue maintenance and disease: the first steps in a long journey. Int J Oral Sci 5: 121-129.
- Sen S, Sharma S, Gupta A, Gupta N, Singh H, et al. (2011) Molecular characterization of explant cultured human oral mucosal epithelial cells. Invest Ophthalmol Vis Sci 52: 9548-9554.
- Luitaud C, Laflamme C, Semlali A, Saidi S, Grenier G, et al. (2007) Development of an engineering autologous palatal mucosa-like tissue for potential clinical applications. J Biomed Mater Res B Appl Biomater 83: 554-561.
- Rouabhia M, Allaire P (2010) Gingival mucosa regeneration in athymic mice using in vitro engineered human oral mucosa. Biomaterials 31: 5798-5804.
- Burillon C, Huot L, Justin V, Nataf S, Chapuis F, et al. (2012) Cultured autologous oral mucosal epithelial cell sheet (CAOMECS) transplantation for the treatment of corneal limbal epithelial stem cell deficiency. Invest Ophthalmol Vis Sci 53: 1325-1331.
- Ohki T, Yamato M, Murakami D, Takagi R, Yang J, et al. (2006) Treatment of oesophageal ulcerations using endoscopic transplantation of tissue-engineered autologous oral mucosal epithelial cell sheets in a canine model. Gut 55: 1704-1710.
- Mah W, Jiang G, Olver D, Cheung G, Kim B, et al. (2014) Human Gingival Fibroblasts Display a Non-Fibrotic Phenotype Distinct from Skin Fibroblasts in Three-Dimensional Cultures. PLoS One 9: e90715.
- Fournier BP, Larjava H, Häkkinen L (2013) Gingiva as a source of stem cells with therapeutic potential. Stem Cells Dev 22: 3157-3177.
- Jin SH, Lee JE, Yun JH, Kim I, Ko Y, et al. (2014) Isolation and characterization of human mesenchymal stem cells from gingival connective tissue. J Periodontal Res 17.
- Davies LC, Locke M, Webb RD, Roberts JT, Langley M, et al. (2010) A multipotent neural crest-derived progenitor cell population is resident within the oral mucosa lamina propria. Stem Cells Dev 19: 819-830.
- Fournier BP, Ferre FC, Couty L, Lataillade JJ, Gourven M, et al. (2010) Multipotent progenitor cells in gingival connective tissue. Tissue Eng Part A 16: 2891-2899.
- Tang L, Li N, Xie H, Jin Y (2011) Characterization of mesenchymal stem cells from human normal and hyperplastic gingiva. J Cell Physiol 226: 832-842.
- Rouabhia M, Deslauriers N (2002) Production and characterization of an in vitro engineered human oral mucosa. Biochem Cell Biol 80: 189-195.
- Mostefaoui Y, Bart C, Frenette M, Rouabhia M (2004) Candida albicans and Streptococcus salivarius modulate IL-6, IL-8, and TNF-alpha expression and secretion by engineered human oral mucosa cells. Cell Microbiol 6: 1085-1096.
- Claveau I, Mostefaoui Y, Rouabhia M (2004) Basement membrane protein and matrix metalloproteinase deregulation in engineered human oral mucosa following infection with Candida albicans. Matrix Biol 23: 477-486.
- Zhang Q, Shi S, Liu Y, Uyanne J, Shi Y, et al. (2009) Mesenchymal stem cells derived from human gingiva are capable of immunomodulatory functions and ameliorate inflammation-related tissue destruction in experimental colitis. J Immunol 183: 7787-7798.
- Marynka-Kalmani K, Treves S, Yafee M, Rachima H, Gafni Y, et al. (2010) The lamina propria of adult human oral mucosa harbors a novel stem cell population. Stem Cells 28: 984-995.
- Wang F, Yu M, Yan X, Wen Y, Zeng Q, et al. (2011) Gingiva-derived mesenchymal stem cell-mediated therapeutic approach for bone tissue regeneration. Stem Cells Dev 20: 2093-2102.