
Journal of Syndromes
Download PDF
Case Report
*Address for Correspondence: Mandira Dasgupta, MD, DNB (G&O), Department of Obstetrics and Gynecology, Medical College, Kolkata 88, College Street, Kolkata 700 073, Kolkata, India, Tel: +91 9831106193; E-mail: mandiradasgupta@hotmail.com
Citation: Dasgupta M, Jaya D, Bag T, Dutta S, Mallick D. Recurrence of Ogilvie’s Syndrome, a Rare Postoperative Complication in Second Caesarean Section. J Syndromes. 2016;3(1): 4.
Copyright © 2016 Dasgupta et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Syndromes | ISSN: 2380-6036 | Volume: 3, Issue: 1
Submission: 23 May, 2016 | Accepted: 13 June, 2016 | Published: 18 June, 2016

We summoned help from general surgery. The surgeon, not having found any signs of peritonitis made a diagnosis of paralyticileus. He recommended conservative treatment with intravenous fluids, insertion of nasogastric and rectal tubes, p-enema daily, metoclopromide 3 times daily, antibiotics and blood transfusion.

Thus, this was a case of recurrent Ogilvie’s syndrome or acute colonic pseudo obstruction (ACPO) recurring in 2 consecutive Caesarean Sections both for severe pre-eclampsia.

In obstetric cases, it is speculated that this autonomic imbalance may be triggered by damage to the sacral parasympathetic nerves that supply the colon and run close to the cervix, vagina and broad ligament [7]. Thus surgical procedures that may damage sacral parasympathetic nerves like caesarean section, pelvic surgery and trauma may be responsible for Ogilvie’s syndrome in female population.
Recurrence of Ogilvie’s Syndrome, a Rare Postoperative Complication in Second Caesarean Section
Mandira Dasgupta*, Deepti Jaya, Tarasankar Bag, Shyamali Dutta and Dipa Mallick
- Department of Obstetrics and Gynecology, Medical College, Kolkata, India
*Address for Correspondence: Mandira Dasgupta, MD, DNB (G&O), Department of Obstetrics and Gynecology, Medical College, Kolkata 88, College Street, Kolkata 700 073, Kolkata, India, Tel: +91 9831106193; E-mail: mandiradasgupta@hotmail.com
Citation: Dasgupta M, Jaya D, Bag T, Dutta S, Mallick D. Recurrence of Ogilvie’s Syndrome, a Rare Postoperative Complication in Second Caesarean Section. J Syndromes. 2016;3(1): 4.
Copyright © 2016 Dasgupta et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Syndromes | ISSN: 2380-6036 | Volume: 3, Issue: 1
Submission: 23 May, 2016 | Accepted: 13 June, 2016 | Published: 18 June, 2016
Abstract
Acute colonic pseudo obstruction (ACPO), also known as Ogilvie’s syndrome is a very rare postoperative complication of Caesarean section. It has classically been reported in critically ill patients and following cardiac and hip surgery. Whether this complication recurs in subsequent operations is not known. Only one case report of recurrence following caesarean section was found in literature survey. We report a case of Ogilvie’s syndrome which recurred in the second Caesarean section and was successfully managed conservatively.Keywords
Ogilvie’s syndrome; Acute colonic pseudo-obstruction; RecurrenceIntroduction
Ogilvie’s syndrome or acute colonic pseudo obstruction (ACPO) is a rare but potentially fatal postoperative complication which is characterised by severe adynamic ileus with massive colonic dilatation in the absence of mechanical obstruction. Sir William Heneage Ogilvie described this syndrome in 1948 which was subsequently named after him. It has an incidence of 0.1% approximately following major surgeries [1] like cardiac and hip surgery [2,3]. In women, caesarean section appears to be the most common surgery associated with Ogilvie’s syndrome [4].We report a case of recurrent Ogilvie’s syndrome in two consecutive Caesarean sections in a patient with severe pre-eclampsia. On both occasions she was successfully managed conservatively. This case is unique because it seems to be the second such reported case of post cesarean section recurrent Ogilvie’s syndrome (MEDLINE with search terms pseudo obstruction, post caesarean, and recurrence). Given the rising trend of caesarean sections, it is intuitive that this rare syndrome may not remain rare in the future. Obstetricians thus need to have awareness regarding the features, preventive measures and early recognition and management of this complication because patients may have to undergo cesarean sections in more than one occasions in her lifetime.
Case Presentation
A 33 years old P2+0 with 2 previous caesarean sections was referred to our hospital with gradual distension of abdomen from the 5th postoperative day of Caesarean section. She had no stool since operation but was passing flatus without any vomiting or fever. She had undergone emergency Caesarean section under spinal anaesthesia in a peripheral health unit for severe pre-eclampsia in a post caesarean pregnancy.The operative notes in the referral card mentioned that she had an episode of postpartum haemorrhage on the operation table which was managed by syntocinon drip, prostaglandin F2 ɑ (250 mcg I.M) and per rectal misoprostol (800 mcg). The estimated blood loss was around 1000 ml which was replaced with crystalloids and colloids. No adhesions were found during the surgery. The mother remained stable throughout the operative period and was put on magnesium sulphate injection as per Pritchard’s regime. She received postoperative medications as per protocol which included syntocinon, mepiridine, tramadol and antibiotics. From the 5th postoperative day she developed abdominal distension and pallor, and was transferred to our care.
On admission, her blood pressure was 160/110 mm of Hg. She also had proteinuria-(urine dipstick 4+), pallor (haemoglobin-7.9 gm%), low platelets (23,000/mm3) and icterus (total bilirubin of 9.3 mg/dl). Her abdomen was distended with a girth of 100 cm, tympanic note on percussion with intact peristaltic sounds. She had normal blood sodium (132 mmol/l), potassium (3.6 mmol/l), urea (31 mg%) and creatinine (1.2 mg/dl) levels.
Non contrast X-ray abdomen in erect posture revealed multiple air fluid levels with no evidence of free gas under the domes of diaphragm (Figure 1). CT scan revealed dilated caecum and ascending colon without any features of mechanical obstruction.
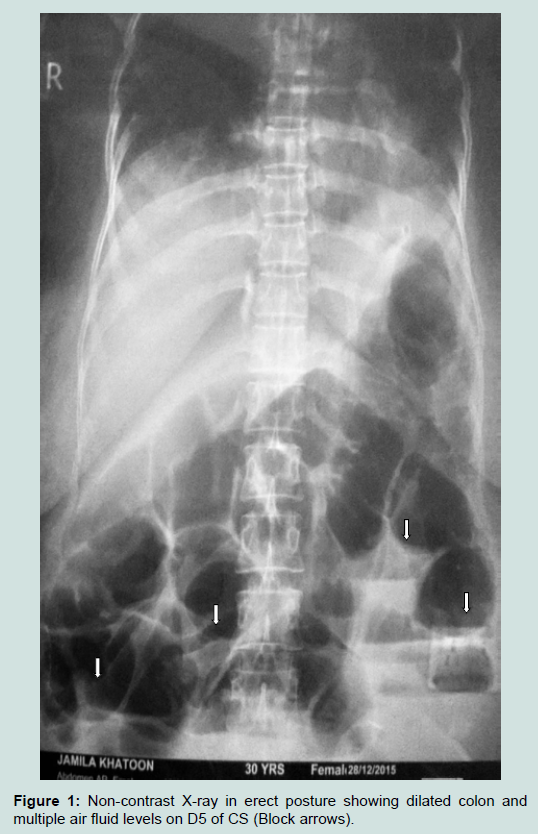
Figure 1: Non-contrast X-ray in erect posture showing dilated colon and multiple air fluid levels on D5 of CS (Block arrows).
Since there were no features of mechanical obstruction or dyselectrolytemia a diagnosis of colonic pseudo-obstruction was made with massive dilatation of the caecum (diameter 10 cm) and right colon on abdominal X-ray (Figure 1).
Her condition remained unimproved for 3 days. A repeat x-ray in erect posture was done to look for free gas under the diaphragm. Fortunately it was not present and conservative management continued in the absence of features of organ perforation or sepsis.
Abdominal girth gradually started decreasing after 3 days and the patient passed stools on fourth day. She was finally discharged from hospital on the 14th day with a diagnosis of Ogilvie’s syndrome in a case of severe pre-eclampsia following Caesarean section.
She showed us notes of her previous Caesarean section which she had undergone 10 years back, for severe pre-eclampsia with fetal distress. There was documentation of a similar episode of abdominal distension from the fourth postoperative day without any dys-electrolytimia, sepsis or features of mechanical obstruction. The non-contrast erect posture X-ray plate was almost identical with the present plate with hugely dilated colon and no free gas under the domes of diaphragm (Figure 2). She recovered with conservative management even on that occasion. However, the probable diagnosis of Ogilvie’s Syndrome was missed. By retrospective analysis this diagnosis was made this time.

Figure 2: Non-contrast X-ray in erect posture showing dilated colon (Block arrows) in previous CS (D4).
Discussion
The precise mechanism of ACPO remains unknown although it is likely to be related in part to excessive parasympathetic suppression or sympathetic stimulation in the regulation of intestine motility [5,6]. The parasympathetic nervous system promotes gut motility through the vagus and sacral parasympathetic nerves (S2-S5), while sympathetic stimuli inhibit bowel peristalsis. An imbalance in the sympathetic and parasympathetic tone leads to reduced colonic motility and functional bowel obstruction.Conditions that lead to a dysfunction of the parasympathetic sacral nerves-nervi erigentes (S2, S3, S4), are responsible for a weakness of the left colon and rectum causing a functional occlusion. This explains the anatomical junction between normal and dilated colon most commonly being the splenic flexure. The proximal colon with parasympathetic nerve supply from the vagus nerve has normal peristalsis (Figure 3).
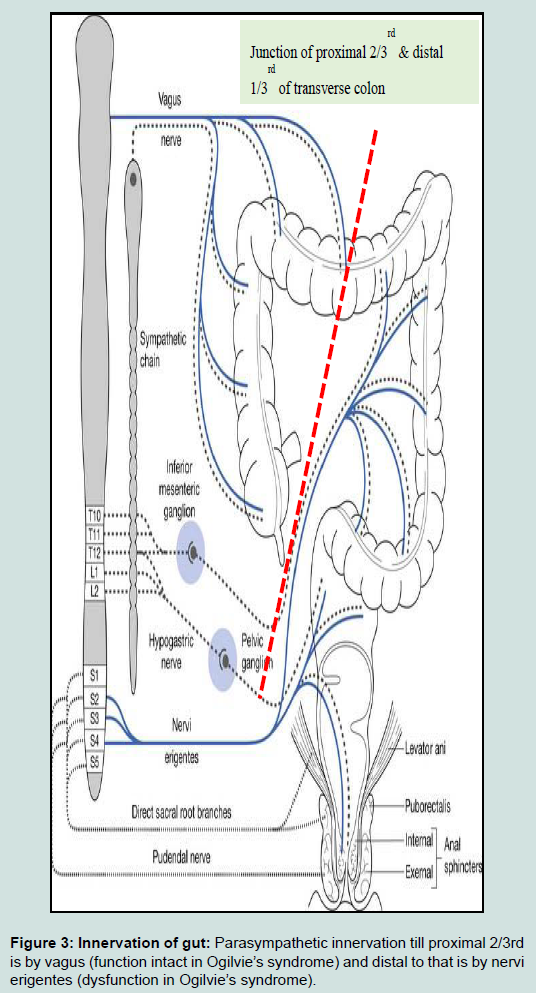
Figure 3: Innervation of gut: Parasympathetic innervation till proximal 2/3rd is by vagus (function intact in Ogilvie’s syndrome) and distal to that is by nervi erigentes (dysfunction in Ogilvie’s syndrome).
Intraoperative spillage of peritoneal irritants (e.g. meconium), intestine manipulation, and the release of inflammatory mediators may affect the neuronal pathways of the intestine [8]. Conditions like surgery (especially cardiac and hip surgery), cardiac failure, respiratory failure, opioid use, spinal anaesthesia, neurological problems, infection, electrolyte imbalance and stress that causes central secretion of corticotrophin-releasing factor leading to sympathetic overactivity (i.e. inhibits gut motility) [5,8] have been reported as positive associations with this condition.
In our patient, the etiology appears to be multifactorial. The caesarean section per se together with peroperative and postoperative opioids, spinal anesthesia, hypertension, post-partum haemorrhage and oxytocin could have all contributed to the development of the Ogilvie’s syndrome. The effect of prostaglandin F2ɑ and magnesium sulphate on the smooth muscles could have compounded this effect.
Finally, it is possible that the vasculopathy of severe pre-eclampsia might have played a role too.
The mainstay of management of this condition is early diagnosis. The diagnosis should be suspected in patients presenting with gradual abdominal distension following Caesarean section/gynaecological surgery, or in hospitalized patients with serious underlying medicaland surgical conditions. Life threatening complications like ischemic necrosis in massively dilated intestinal segments [9] leading to peritonitis may occur.
Abdominal distension usually develops over 3-7 days (mean of 5 days) but can occur as rapidly as 24 h. The clinical features of ACPO include abdominal distension, abdominal pain (80%) and nausea and/or vomiting (60%). Passage of flatus or stool is reported in up to 40% of patients. Patients with ischaemic or perforated bowel have similar symptoms but are more likely to be febrile. On examination, the abdomen is tympanitic and bowel sounds are typically present. Fever, marked abdominal tenderness and leucocytosis are more common in patients with ischaemia or perforation but also occur in those who have not developed these complications [10].
Supportive therapy is the preferred initial management of ACPO and should be instituted in all patients [11]. Success rates as high as 96 per cent have been achieved with conservative measures [12], but poorer results have been reported [13]. Medical managements include drugs like metoclopramide and neostigmine. Neostigmine (a reversible acetylcholinersterase inhibitor that stimulates the colon) is the best evaluated medical treatment with published success rates of up to 50 per cent of patients [14,15].
Additional trials of prokinetics have not been so successful in treating ACPO. Only anecdotal cases utilizing erythromycin, metoclopramide, and cisapride have been reported [2,16]. Colonic decompression may be needed in cases of severe caecal distension. Surgery is usually required only if conservative management has failed and usually involves bowel resection with temporary diversion, requiring a second stage closure. Although colonoscopic decompression is successful in 77% of patients, colonoscopy is technically difficult, not always successful, and may cause complications such as perforation. Additionally, colonic distention may recur in up to 40% of patients, despite initial successful decompression [4]. Furthermore, the cost of colonoscopy is substantially higher than that of parenteral neostigmine. Surgical intervention is associated with high morbidity and mortality rates [10]. Therefore, colonoscopic or surgical decompression needs to be reserved for situations wherein conservative treatment fails. Patient age, caecal diameter and timing of decompression influence mortality rate (15% versus 36-44%), because of ischaemia and perforation [17]. Luckily our patient did not require any aggressive treatment.
In our case there was a previous history of Ogilvie syndrome, which had remained undiagnosed. A similar case has been reported by Bozin M, et al. in 2014 which showed recurrence of Ogilvie syndrome after successive caesarean sections and demonstrated failure to identify previous ACPO after her first caesarean section and inappropriate use of simethicone and opioid analgesia leading to progression of disease and the need for laparotomy for intestinal perforation [19].
In our case also the syndrome was unrecognised in a previous Caesarean Section and thus no preventive measures could be adopted this time. But we diagnosed Ogilvie’s syndrome early and with timely intervention could avoid surgical intervention.
Lessons learnt from this case
Ogilvie’s syndrome, though rare can recur in subsequent pregnancies or Caesarean Sections, especially in the presence of hypertension and PPH. Spinal anaesthesia, opioids, PPH and other precipitating factors should be avoided in patients with a prior history of Ogilvie’s syndrome as a measure for preventing recurrence. The role of magnesium sulphate, a neuromuscular inhibitor in aggravating or precipitating this syndrome needs to be explored. Early diagnosis of this rare complication by a high degree of suspicion in postoperative intestinal obstruction following Caesarean Section can avert significant maternal morbidity and mortality. Advances in minimally invasive surgery and newer drugs will improve future management of this life-threatening complication.
References
- Srivastava G, Pilkington A, Nallala D, Polson DW, Holt E (2007) Ogilvie's syndrome: a case report. Arch Gynecol Obstet 276: 555-557.
- Delgado-Aros S, Camilleri M (2003) Pseudo-obstruction in the critically ill. Best Pract Res Clin Gastroenterol 17: 427-444.
- van der Spoel JI, Oudemans-van Straaten HM, Stoutenbeek CP, Bosman RJ, Zandstra DF (2001) Neostigmine resolves critical illness related colonic ileus in intensive care patients with multiple organ failure--a prospective, double-blind, placebo-controlled trial. Intensive Care Med 27: 822-827.
- Tenofsky PL, Beamer L, Smith RS (2000) Ogilvie's syndrome as a post operative complication. Arch Surg 135: 682-686.
- Saunders MD (2007) Acute colonic pseudo-obstruction. Best Pract Res Clin Gastroenterol 21: 671-687.
- Ponec RJ, Saunders MD, Kimmey MB (1999) Neostigmine for the treatment of acute colonic pseudo-obstruction. N Engl J Med 341: 137-141.
- Kadesky K, Purdue GF, Hunt JL (1995) Acute pseudo-obstruction in critically ill patients with burns. J Burn Care Rehabil 16(2 Pt 1): 132-135.
- Batke M, Cappell MS (2008) Adynamic ileus and acute colonic pseudo-obstruction. Med Clin North Am 92: 649-670.
- Alam HB, Fricchione GL, Guimaraes AS, Zukerberg LR (2009) Case records of the Massachusetts General Hospital. Case 31-2009. A 26-year old man with abdominal distention and shock. N Engl J Med 361: 1487-1496.
- Vanek VW, Al-Salti M (1986) Acute pseudo-obstruction of the colon (Ogilvie’s syndrome). An analysis of 400 cases. Dis Colon Rectum 29: 203-210.
- Eisen GM, Baron TH, Dominitz JA, Faigel DO, Goldstein JL, et al. (2002) Acute colonic pseudo-obstruction. Gastrointest Endosc 56: 789-792.
- Sloyer AF, Panella VS, Demas BE, Shike M, Lightdale CJ, et al. (1988) Ogilvie’s syndrome. Successful management without colonoscopy. Dig Dis Sci 33: 1391-1396.
- Loftus CG, Harewood GC, Baron TH (2002) Assessment of predictors of response to neostigmine for acute colonic pseudo-obstruction. Am J Gastroenterol 97: 3118-3122.
- Abeyta BJ, Albrecht RM, Schermer CR (2001) Retrospective study of neostigmine for the treatment of acute colonic pseudo-obstruction. Am Surg 67: 265-268.
- De Giorgio R, Barbara G, Stnahellini V, Tonini M, Vasina V, et al. (2001) The pharmacologic treatment of acute colonic pseudo-obstruction. Aliment Pharmacol Ther 15: 1717-1727.
- MacColl C, MacCannell KL, Baylis B, Lee SS (1990) Treatment of acute colonic pseudoobstruction (Ogilvie's syndrome) with cisapride. Gastroenterology 98: 773-776.
- Shakir AJ, Sajid MS, Kianifard B, Baig MK (2011) Ogilvie’s syndrome-related right colon perforation after caesarean section: a case series. Kaohsiung J Med Sci 27: 234-238.
- Bozin M, Khomko N, Shedda S (2014) Recurrence of acute colonic pseudo-obstruction post-caesarean section: a case report. ANZ J Surg 84: 196-197.