
Journal of Surgery
Download PDF
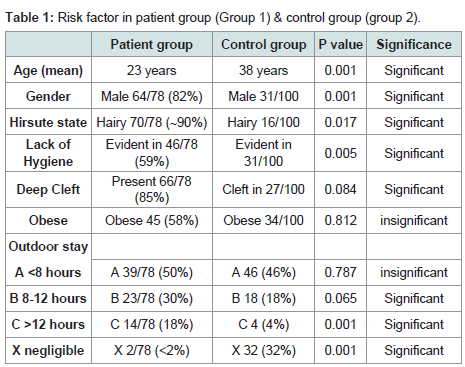 Table 1: Risk factor in patient group (Group 1) & control group (group 2).
Table 1: Risk factor in patient group (Group 1) & control group (group 2). 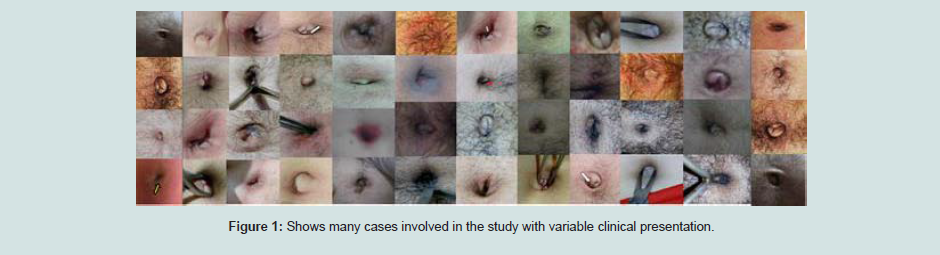 Figure 1: Shows many cases involved in the study with variable clinical presentation.
Figure 1: Shows many cases involved in the study with variable clinical presentation. 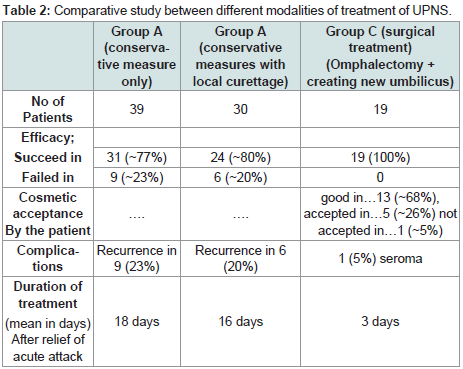 Table 2: Comparative study between different modalities of treatment of UPNS.
Table 2: Comparative study between different modalities of treatment of UPNS. 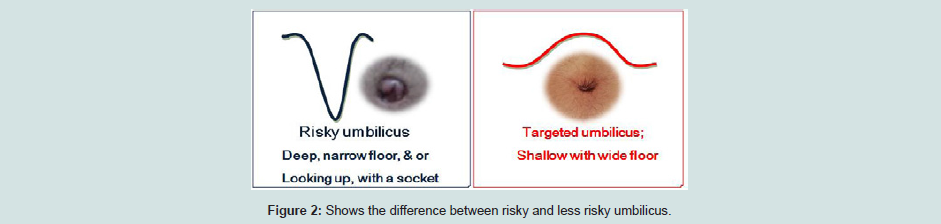 Figure 2: Shows the difference between risky and less risky umbilicus.
Figure 2: Shows the difference between risky and less risky umbilicus.
Research Article
Umbilical Pilonidal Disease;Predisposing Factors & Best Modality of Management
Elsaady A1*, Aboelsaad M2 and Elbehery M3
- 1Departement of general surgery, Kafr Elshikh General Hospital, Egypt
- 2Departement of general surgery, Desouk General Hospital, Egypt
- 3Departement of general surgery, Kafr Elshikh General Hospital, Egypt
*Address for Correspondence: Elsaady A, Departement of general surgery, Kafr Elshikh General Hospital, Egypt, Email: ah.elsaady30@gmail.com
Citation: Elsaady A, Aboelsaad M, Elbehery M. Umbilical Pilonidal Disease; Predisposing Factors & Best Modality of Management. J Surgery. 2018;6(2): 4.
Copyright: © 2018 Elsaady A. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 6, Issue: 2
Submission: November 02, 2018| Accepted: December 03, 2018 | Published: December 06, 2018
Abstract
Umbilical pilonidal sinus is an unusual variant of the pilonidal diseases. It occurs with an incidence thought to be 0.6%. Little was reported in literature about the disease. This study is a prospective one that aims at investigating factors predisposing to the development of disease and comparing different modalities of treatment.
All patients for more than fourteen years, were involved &assessed for age, gender, family history, hirsute state, obesity, local hygiene, and the presence of deep umbilical cleft were reported & compared with a control group Three modalities in treatment were compared ; conservative measures only (group A), curettage and conservative measures (group B), and omphalectomy with reconstruction of new umbilicus (group C).
Seventy eight cases were presented. Significant differences were present in age, sex, lack of local hygiene, & deep umbilicus compared to control group. Conservative modalities are quite efficient modality for treatment that was successful in 77% of the patients. Recurrence occurred in nine patients (23%) of group A & six patients 20% in group B. No recurrence reported in group C (19 cases) , with only one (4%) with minor complications (seroma) The cosmetic acceptance was good in seventeen patients (68%), accepted in six patients (24%) and not accepted in one patient (4%).
The study concluded that; deep navel, hairiness, and poor local umbilical hygiene are necessary for the umbilical pilonidal disease to be developed. Conservative management is a well efficient modality of treatment and should be considered as an initial modality of choice. Surgical treatment should be only confined to those fail to tolerate conservative measures. We prefer to remove the umbilicus and fashioning of new umbilicus with base and cylinder rather thancone shaped to be less risky for trapping hair to avoid the recurrence & cosmetically accepted by the patient.
Keywords
Umbilical pilonidal disease; Pilonidal sinus; Umbilical disease
Introduction
Pilonidal sinus is a well-recognized chronic foreign body inflammatory reaction that occurs mostly in the sacrococcygeal area [1]. However, several unusual occasional sites have been reported in literatures [2]. Umbilical ilonidal sinus is one of these rare variant that occurs with an incidence and the prevalence thought to be 0.6% and 0.1%, respectively [3]. Little was reported in literature about the disease and predisposing factors, with no consensus about best modalities of the treatment [4]. This study is a prospective one that aims at investigating factors predisposing to the development of disease and comparing different modalities of treatment.
Materials and Methods
All patients presented with pilonidal sinus in the umbilicus (from 1/2004 till 6/2018) in Kafr Elshiekh General Hospital were involved in the study. The diagnosis was made by the presence of a history of repeated inflammations and discharges with a demonstration of broken hairs seen exuding or present within the umbilicus, while the histologic diagnosis of the disease was limited to the operated cases only.
The study concerned about the evaluation of the possible risk factors accused of the development of the disease as well as the efficacy of different modalities of treatment. The patient characteristics in terms of; age, gender, family history, hirsute state, obesity, local hygiene, and the presence of deep umbilical cleft were reported as shown in the (Table 1). Findings were compared with those from 100 consecutive control patients presented to the general surgical policlinics who are not suffering from the disease. Thus we have the patient group (Group 1), & control group (Group 2).
The study also compared the efficacy of different modalities of treatment. Patients were divided into three groups. Group A; where conservative measures were applied only. This included; hair removal by regular shaving or depilatory agents or even laser ablation (in two cases). Good personal hygiene & local cleanliness for at least twice weekly were advised. Group B; where hair removal and curettage under local anesthesia were done with the conservative measures mentioned before. Group C; where surgical treatment was done either as an initial procedure or after the failure of treatment in group A & B. Failure of treatment in group A or B was defined as recurrence of acute inflammation for more than two times & or persistence of the discharge after 4months of conservative measures. Cases failed to respond to conservative measures were managed surgically and included in group C. Surgical treatment in this study entailed omphalectomy with refashioning of the new less risky umbilicus. The new umbilicus was designed to be cylinder rather than cone shaped with a wide base. This is done by removing a part of subcutaneous fat in area prepared to be the new umbilicus then pulling vertically downward, fixing the dermis above to the rectus sheath below in a circular line rather than a point by wide a purse string without tightening connecting the dermis to the sheath in a wide circle so that the new umbilicus become fixed in a ring. Patients of group C were assessed for recurrence (within two years), complications and cosmetic satisfaction (good, accepted, or bad). The study compared the three modalities of treatment in term of efficacy, complications & recurrence as well as the duration of treatment.
Patients were in the study followed up for at least two years. We exclude cases that dropped in follow up.
Results
Seventy-eight cases were presented in the study. The clinical presentations of the disease in this study vary from acute inflammation to chronic sinus with repeated umbilical discharge and sometimes chronic eczema from continuous discharge. (Figure 1) shows many of the cases presented in the study with the different clinical presentation.
Assessment of the risk factors in the patients & control groups were done. Most of the patients in (Group 1) were males; 64 from 78 patients (82%), with the mean age affected, were twenty-three years. The hirsute state was present in 70 patients (~90%), while lack of local umbilical cleaning was evident in 46 patients (59%). Deep umbilicus was evident in 66 patients (85%). Forty-five (58%) patients were obese. Thirty-nine patients (50%) working or stay outdoor for less than eight hours, twenty-three remain between eight to twelve hours, and fourteen patient (18%) stay for more than 12 hours, and only two patients (<2%) stay outdoor for less than two hours.
On comparison the patient group to the control group as shown in the (Table 1), significant differences were present in age, sex, lack of local hygiene, & deep umbilicus. There was no significant difference in obesity as a mere risk factor. As regard to the lifestyle and staying outdoor, there was no significant difference in those of less than eight hours but significant differences were present in those with more than eight hours as well as negligible periods (less than two hours).
Non-surgical management was applied in sixty nine cases. Group A (conservative measures only) included thirty nine cases, while group B (conservative measure with local curettage) included thirty cases. Group C (surgical treatment) included nineteen patients; five cases from the start and fourteen patients failed non-surgical management (nine patients from group A (23%), & six patients (20%) from group B). Conservative measures were successful in thirty one patients (77%) while Conservative measures with curettage were successful in twenty four patients (80%). No significant differences in the recurrence rate were found between groups A &B. Surgical treatment (group C) was successful in all patients with no recurrence reported, but with one (5%) (minor) complication (seroma). The cosmetic acceptance was good in thirteen patients (68%), accepted in five patients (26%) and not accepted in one patient (5%). There was no significant difference in the mean duration of treatment in group A&B, while it was significantly shorter in group C.
Discussion
Pilonidal sinus is a chronic foreign body reaction [5]. It represents a granulomatous reaction to a hair shaft penetrating the epidermis from the cutaneous surface [6]. Umbilical Pilonidal Sinus (UPNS) is an unusual variety of the disease that commonly seen in the sacroccocygeal area. The disease was first published by Warren in 1854, while the term “umbilical pilonidal sinus” was first described and used by Williams and Patey in 1956. The incidence of the disease is thought to be 0.6% [4]. However, it may be actually more common than thought and may be found more frequently if sought specifically [7]. Although these case had been reported in the literature as rare cases, but current reports indicate that umbilical pilonidal sinus is more common in the general population than was generally thought, and may be found more frequently if sought specifically with possible recent increased incidence [8,9]. The relatively higher incidence of the disease has been reported in Middle East countries [7]. This may be explained by the cultural and traditional factors. People in these areas believe that umbilicus is a delicate structure and it is dangerous to be manipulated too much! This leads to accumulation of hairs and dirty material with subsequent chronic infection and inflammation and hair penetration [7]. However, more studies are necessary toconfirm and explain this finding [7] (Table 2).
The development of the disease is suggested to be initiated by movement of broken hair from the surrounding skin into the umbilical groove, that with friction pits on movement & puncture the skin initiating the process [8]. Accordingly, the development of the disease is very suggestible by the concomitant availability of; invader (loose hair), the force causing hair penetration & skin vulnerability for penetration in the depth of a cleft [9]. So, once the three factors are provided at the umbilicus the disease may be developed [10]. Many predisposing factors are incriminated in the development of the disease in the literature [11]. Male gender, young age, hairiness, deep navel, poor personal hygiene, obesity, tight cloth were found to be the predisposing factors for the development of the disease in the umbilicus [9]. The increased incidence thought to be present may beattributed to the higher incidence of risk factors nowadays such as obesity, economic burdens making with long periods out-home life that may be associated with lack of personal hygiene & tight clothes [12].
This study demonstrated great predominance of the disease in male (82%). The mean age of affection was twenty three years old. This corresponds to the age of more tough hair than older or younger age groups [8]. The predisposing factors are very important in the development of the disease with clear significant difference with control groups. Hirsute state was nearly a constant finding presenting in nearly 90% of patients, while lack of local umbilical cleaning was evident in approximately 59%. Deep umbilicus was presented in about 85% of the patients. Although obesity was reported in many studies to be a risk factor [11], but this study failed to document this as a mere risk factor. This may explain the necessity of the presence of other factors such as dense hair, lack of personal hygiene and or deep umbilical cleft. The study reported more incidence of the disease in those working or staying outdoors more than eight hours (48%) which may reflect less local hygienic care to the already predisposed umbilicus.
Microscopically, the lesion characterized by the presence of a foreign body granuloma. An epithelial-lined sinus tract leads to an area of fibrosis and granulation tissue surrounding hair shafts [13]. Umbilical sinus tract differs from the sacrococcygeal variety in the absence of multiple tracts and low recurrence rates [14].
The clinical presentation of the disease varies from acute inflammation and sometimes with abscess formation, to chronic repeated discharge and recurrent inflammations [15]. Most of the patients complain recurrent attacks of umbilical pain & or discharge [16]. It can be diagnosed with a careful examination, in which hairs can be seen deep in the umbilicus and usually protrude from a small sinus. Other umbilical anomalies such as an umbilical hernia, endometriosis (for women), Sister Mary Joseph nodule, pyogenic granuloma, urachus and epidermoid cysts should be kept in mind at the differential diagnosis [17,18]. A special concern should be givenfor different causes of umbilical discharge [19]. A pre-operative intraabdominal imaging may be beneficial [20].
There is still controversy in the management [21]. Actually, umbilical pilonidal sinus (UPNS) is one of the most neglected diseases that only a few studies were reported in the literature. No consensus about the treatment of the disease [22]. Some recommend conservative management as the mainstay method of treatment, depending on the usual absence of multiple tracts and low recurrencerates in umbilical pilonidal sinus [23]. While other does not see any role in conservative management [24]. Some believe that there is a risk of peritoneal extension of inflammation from this lesion, and consequently, don`t accept conservative treatment [18]. Some author advocate complete excision of the umbilicus for curative goal and avoidance of recurrence [23]. This is may not be accepted cosmetically by some patients. Other advocate sinus excision with preservation of the umbilicus [25]. This limited resection is likely to be effective because umbilical pilonidal disease is significantly different from the sacrococcygeal condition, with low recurrence rates and absence of multiple tracts. In addition, the incision through the umbilicus results in a better cosmetic result and more accurate appreciation of the anatomic pathology than umbilectomy or a periumbilical incision [25]. Omphalectomy and creating new umbilicus is another option which is quite effective and cosmetically accepted [26]. On reviewing the shape of the umbilicus in the patients, most of them had a deep cleft cone or socket like with the deepest part was the narrowest part. This makes the umbilicus entrap hair easily, so the new umbilicus should be with a wide base to avoid hair entrapment as shown in (Figure 2).
In this study the surgical treatment (consists of omphalectomy and refashioning of new wide less risky umbilicus) provided an efficient definitive method of treatment with no recurrence and much less duration of treatment compared to other methods. However, the non surgical methods of management were also effective modalities in treatment that were successful in 77% of the patients, with recurrence rate 20-23%. There are no significant differences to do conservative measure either with or without local curettage. Conservative measures consist of regular hair removal and local umbilical cleaning. Conservative measures should be considered as an initial modality of treatment of umbilical pilonidal sinus. While surgical treatment should be only confined to the patients failed or can’t tolerate conservative measures. Omphalectomy with reconstructing a new umbilicus with a wide base is the optimum choice for surgical treatment with no recurrence and good cosmetic acceptance by the patients.
Conclusion
Although umbilical pilonidal sinus is reported as a rare disease with a prevalence of about 0.6% [27], however, it is generally thought that the true incidence is much more than believed [28]. Deep navel, hairiness, and poor local umbilical hygiene are necessary for the sinus to be developed. Conservative management is a well efficient modality of treatment and should be considered as an initial modality of choice. Although surgical treatment provides definitive treatment with no or very low recurrence and less duration of treatment, It should be only confined to the patients failed or can‘t tolerateconservative measures. We prefer to remove the umbilicus and fashioning the new umbilicus with base and cylinder rather than cone shaped to be less risky for trapping hair and subsequently recurrence & to be cosmetically accepted by the patient.
References
- Azzam S. Al-Kadi (2014) Umbilical Pilonidal Sinus. Int J Health Sci (Qassim) 8: 307-310.
- Sion-Vardy N, Osyntsov L, Cagnano E, Osyntsov A, Vardy D, et al. (2009) Unexpected location of pilonidal sinuses. Clin Exp Dermatol 34: e599-e601.
- Akkapulu N, Tanrikulu Y (2011) Umbilical Pilonidal Sinus: A Case Report. J Med Cases 2: 272-274.
- Sozen S, Kanat BH, Kanat Z, Bali I, Polat Y, et al. (2015) Effective conservative treatment of umbilical pilonidal sinus disease: Silver nitrate? Salt?. Ann Ital Chir 86: 450-455
- Salih AM, Kakamad FM, Essa RA, Mohammed SH, Salih RQ, et al. (2017) Kakamad Pilonidal sinus of the umbilicus; presentation and management. Edorium J Gastrointest Surg 4: 1-4.
- Jeffrey A. Sternberg (2017) The management of pilonidal disease. In: current surgical therapy. Cameron JL, et al. (12th edn). Philadelphia, Saunders Elsevier 387-390.
- Salih AM, Kakamad FH, Essa RA, Mohammed SH, Salih RQ, et al. (2017) Pilonidal sinus of the umbilicus: Presentation and management. Edorium J Gastrointest Surg 4: 1-4.
- Coskun A, Bulus H, Akinci OF, Özgönül A (2011) Etiological factors in umbilical pilonidal sinus. Indian J Surg 73: 54-57
- Eryilmaz R, Sahin M, Okan I, Alimoglu O, Somay A, et al. (2005) Umbilical pilonidal sinus disease: predisposing factors and treatment. World J Surg 29: 1158-1160.
- Kaplan M, Kaplan EF, Kaplan T, Kaplan FC (2017) Umbilical pilonidal sinus, an underestimated and little-known clinical entity: report of two cases. Am J Case Rep18: 267-270.
- Coşkun A, Buluş H, Akıncı OF, Özgönül A (2011) Etiological factors in umbilical pilonidal sinus. Indian J Surg 73: 54-57.
- McClenathan JH (2000) Umbilical pilonidal sinus. Can J Surg 43: 225.
- Parpoudi SN, Kyziridis DS, Patridas DC, Makrantonakis AN, Iosifidis P, et al. (2016) Is histological examination necessary when excising a pilonidal cyst? Am J Case Rep 16: 164-168.
- Al-Kadi AS (2014) Umbilical pilonidal sinus. Int J Health Sci (Qassim) 8: 307-310.
- Clery AP, Clery AB (1963) Pilonidal disease of the umbilicus. Br J Surg 50: 666-668.
- Mallin K, Pemminati S (2016) Unique application of cryocone to diagnose umbilical pilonidal cyst. J Clin Diagn Res 10: LD01-LDO2.
- Leelamma JP, Mohammed BA (2016) Case Report Umbilical pilonidal cyst presenting as umbilical sepsis Int J Adv Med 3: 136-137.
- Yadav G, Mohan R (2010) Clinical profile of umbilical discharge in adults; a multicentric study in north India. Internet J Surg 27: 1.
- El-Bakry AA (2002) Discharging umbilicus. Saudi Med J 23: 1099-1100.
- Kaplan M, Kaplan FC (2017) Comment to “An umbilical surprise: a collective review on umbilical pilonidal sinus”. J. B. Ponten, J. E. H. Ponten, M. D. P. Luyer, S. W. Nienhuijs. Hernia 21: 493-494.
- Kaplan M, Ozcan O, Kaplan F, Yalcin H, Salman B, et al. (2016) Conservative vs. surgical interventions for umbilical pilonidal sinus: A multicenter, double-blind, prospective, randomized clinical trial. J Am Coll Surg 222: 878-889.
- Ponten JB, Ponten JE, Luyer MD, Nienhuijs SW (2016) An umbilical surprise: A collective review on umbilical pilonidal sinus: An uncommon alternative diagnosis in common umbilical symptoms. Hernia 20: 497-504.
- Haj M, Cohen I (2004) Umbilical pilonidal sinus: Ambulatory surgical technique. J Ambul Sur 11: 37-39.
- Naraynsingh V, Hariharan S, Dan D (2009) Umbilical pilonidal sinus: A new treatment technique of sinus excision with umbilical preservation. Dermatol Surg 35: 1155-1156.
- Fazeli MS, Lebaschi AH, Adel MG, Kazemeini AR (2008) Evaluation of the outcome of complete sinus excision with reconstruction of the umbilicus in patients with umbilical pilonidal sinus. World J Surg 32: 2305-2308.
- Srinidhi M, Bhat B (2015) Umbilical pilonidal sinus: a rare presentation. IJSS Case Reports & Reviews 1: 41-43.
- Zeugma Saglik Hizmetleri San (2016) Conservative versus surgical treatment of umbilical pilonidal disease clinical trials.
- Meher S, Mishra TS, Sasmal PK, Sharma R, Rout B, et al. (2016) Umbilical pilonidal sinus: A report of two cases and recent update of literature. J Clin Diagn Res 10: PD20-PD22.