
Case Report
*Address for Correspondence: Wilmo C. Orejola, MD, Department of Surgery, Hackensack University Medical Center, 30 Prospect Avenue, Hackensack, NJ 07601, USA E-mail: wilcore@optonline.net
Citation:Orejola WC, Elmann EM, Wilderman MJ, Cocke TP, Vaidya P, et al. Combined Transcatheter Aortic Valve Replacement and Endovascular Aortic Repair: A Transfemoral Approach Dilemma. J Surgery. 2016;3(2): 3.
Copyright © 2016 Orejola WC, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 4, Issue: 1
Submission: 21 October 2015 | Accepted: 30 December 2015 | Published: 04 January 2016
 Next, through the right femoral artery a 14Fr DrySeal (WL Gore, Flagstaff, AZ) was inserted and a pigtail was positioned in the abdominal aorta over a stiff wire for aortogram. Through an 18Fr DrySeal on the left, a 31 mm Gore Excluder endograft (WL Gore, Flagstaff, AZ) was deployed just below the right renal artery. Then the 23 mm limb was deployed into the right common iliac artery. A completion angiogram demonstrated patent renal arteries, SMA, endografts and showed no evidence of type I, II or III endoleaks (Figure 2). There were no intraoperative complications.
Next, through the right femoral artery a 14Fr DrySeal (WL Gore, Flagstaff, AZ) was inserted and a pigtail was positioned in the abdominal aorta over a stiff wire for aortogram. Through an 18Fr DrySeal on the left, a 31 mm Gore Excluder endograft (WL Gore, Flagstaff, AZ) was deployed just below the right renal artery. Then the 23 mm limb was deployed into the right common iliac artery. A completion angiogram demonstrated patent renal arteries, SMA, endografts and showed no evidence of type I, II or III endoleaks (Figure 2). There were no intraoperative complications.
 Postoperatively, the patient had good urine output with postoperative creatinine down to 2.1 mg/dL. He had a brief upper GI bleeding episode and endoscopic retrograde cholangiopancreatographic (ERCP) restenting of the common bile duct he had previously for choledocholithiasis. There were no cardiovascular events post-operatively. He was discharged home on postoperative day 13.
Postoperatively, the patient had good urine output with postoperative creatinine down to 2.1 mg/dL. He had a brief upper GI bleeding episode and endoscopic retrograde cholangiopancreatographic (ERCP) restenting of the common bile duct he had previously for choledocholithiasis. There were no cardiovascular events post-operatively. He was discharged home on postoperative day 13.
Combined Transcatheter Aortic Valve Replacement and Endovascular Aortic Repair: A Transfemoral Approach Dilemma
Wilmo C. Orejola1,2, Elie M. Elmann1,2, Michael J. Wilderman1,2, Thomas P. Cocke2,Pranaychandra Vaidya2 and Gregory T. Simonian1,2
- 1Department of Surgery, Hackensack University Medical Center, 30 Prospect Avenue, Hackensack, NJ 07601, USA
- 2The Heart and Vascular Hospital, Hackensack University Medical Center, 30 Prospect Avenue, Hackensack, NJ 07601, USA
*Address for Correspondence: Wilmo C. Orejola, MD, Department of Surgery, Hackensack University Medical Center, 30 Prospect Avenue, Hackensack, NJ 07601, USA E-mail: wilcore@optonline.net
Citation:Orejola WC, Elmann EM, Wilderman MJ, Cocke TP, Vaidya P, et al. Combined Transcatheter Aortic Valve Replacement and Endovascular Aortic Repair: A Transfemoral Approach Dilemma. J Surgery. 2016;3(2): 3.
Copyright © 2016 Orejola WC, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 4, Issue: 1
Submission: 21 October 2015 | Accepted: 30 December 2015 | Published: 04 January 2016
Abstract
We report a case of an elderly patient with severe aortic stenosis (AS) too risky for conventional surgery because of comorbidities that included an infrarenal saccular abdominal aortic aneurysm (AAA). The presence of the aneurysm could impact the outcome of transcatheter aortic valve replacement (TAVR) as improved systolic pressure could increase the risk of aneurysm rupture. Transapical and transaortic approaches for TAVR precluded simultaneous endovascular aortic repair (EVAR). Transfemoral approach was the most viable option. Doing EVAR first would circumvent aortic rupture but it could be technically precarious to do EVAR before TAVR when both are done transfemorally. Contrast-induced nephropathy could be considered whether combined procedure is riskier than angiogram-dependent procedures performed in two settings. The patient underwent uncomplicated transfemoral TAVR and then EVAR in one setting. This case underscores the management strategy of a patient with this complicated clinical presentation and underlying pathologies in the light of presently available technologies..Keywords
Aortic valve replacement; Abdominal aortic aneurysm; Endovascular procedure/stentsIntroduction
In 2002, Cribier et al. reported the first human case of percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis [1]. This procedure called TAVR or TAVI (transcatheter aortic valve implantation) has emerged as an effective alternative to conventional aortic valve replacement too risky for patients with preexisting comorbidities [2]. Designed to be less invasive and percutaneous, transfemoral is the preferred approach, but inadequacy of this access in some patients led to more invasive transapical or transaortic approach. The presence of an abdominal aortic aneurysm compounds the risk but could be accordingly repaired endovascularly and transfemorally [3]. We report a case of a combined TAVR and EVAR done transfemorally and in one setting.A Case Report
The patient is an 83-year-old man who presented with severe symptomatic AS and an infrarenal saccular abdominal aortic aneurysm. He came in NYHA class III and ischemic cardiomyopathy. He had coronary artery bypass grafting and mitral valve replacement (St. Jude Medical mechanical valve) in 1994 and multiple percutaneous coronary interventions with stents. He also had a history of myocardial infarction, hypertension, hyperlipidemia, biventricular AICD implantation, chronic renal insufficiency with creatinine 2.7 mg/dL, benign prostatic hyperplasia and stenting of the common bile duct for choledocholithiasis. For conventional AVR, his predicted risk of mortality STS score was 8% and logistic EuroSCORE 18.4%.Transthoracic echocardiogram indicated an aortic valve area 0.8 cm2, mean gradient of 49 mmHg, peak velocity 3.1 m/sec and an ejection fraction of 35%. Coronary angiogram showed patent vein grafts to the distal LAD, an atretic LIMA to proximal LAD and occluded vein grafts to the circumflex and the RCA. A computed tomographic (CT) angiogram revealed an infrarenal saccular abdominal aortic aneurysm measuring 5.5 cm.
He was taken to the hybrid OR. A multi-disciplinary team of cardiac and vascular surgeons, interventional cardiologist and anesthesiologist did the combined procedure. Under general endotracheal anesthesia, bilateral femoral cut-downs were done. Through the right femoral vein a 5Fr balloon-tipped temporary pacing wire was advanced to the RV for rapid pacing during valve positioning. Through the right femoral artery, a 7Fr pigtail was positioned in the ascending aorta for aortogram, while through the left, a J-wire was advanced over the Glidewire up to the thoracic aorta. Multiple dilators were inserted before the Novoflex 3 THV Sapien XT delivery system (Edwards Lifesciences, Irvine, CA) could be advanced. Under fluoroscopic guidance a 23 mm x 40 mm BAV balloon was positioned across the aortic valve. The valve was dilated. The 26-mm Sapien XT THV was deployed as the heart was rapidly paced to 180/min and the mean arterial blood pressure dropped to 45 mmHg transiently. The Sapien valve was deployed without difficulty (Figure 1).
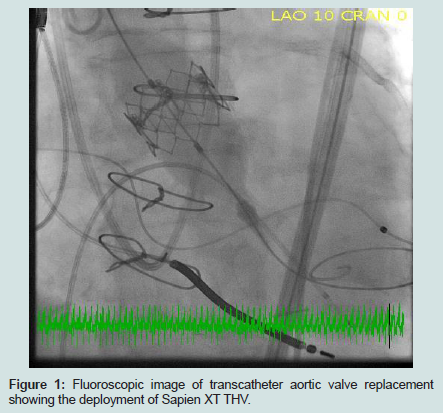
Figure 1: Fluoroscopic image of transcatheter aortic valve replacement showing the deployment of Sapien XT THV.
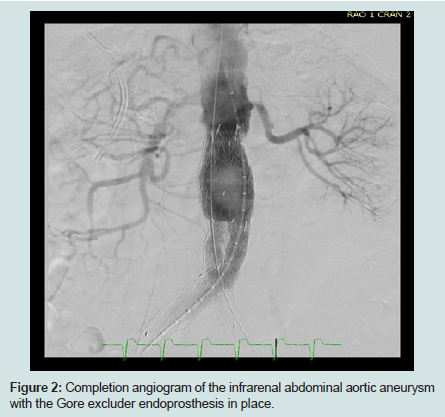
Figure 2: Completion angiogram of the infrarenal abdominal aortic aneurysm with the Gore excluder endoprosthesis in place.
In a six-month and 12-month follow-up, the patient was treated medically for brief exacerbations of congestive heart failure. He is presently asymptomatic.
Comment
Transcatheter aortic valve replacement is increasingly used in an ageing population. Similarly, EVAR has become the primary treatment modality for an abdominal aortic aneurysm (AAA). A combined procedure offers a special challenge because of potential contrast-induced nephropathy [4] and physiologic and technical issues [5,6].Contrast-induced nephropathy is well reported in the medical literature [4]. A dilemma would arise where two-stage instead of a combined one-stage procedure would be more appropriate to allow the kidneys to recover from the nephrotoxic effects of contrast media during multiple angiograms. However, this case showed that minimal use of contrast did not harm our patient who had chronic renal insufficiency preoperatively. Improved postoperative renal function could also be attributed to the immediate hemodynamic effect of TAVI.
Immediate hemodynamic effects of TAVI include decrease in left ventricular end-diastolic pressure and increase in systolic blood pressure [7]. In a patient with coexistent aortic aneurysm increased blood pressure will increase wall strain of the aneurysm and saccular aneurysms have increased risk of dilatation and rupture, as demonstrated by Vorp et al. [8].
A successful TAVI was done on a patient with severe aortic stenosis with comorbidities including coexistent AAA, which was previously treated with EVAR [9]. In a combined procedure reported by Yanes-Bowden et al., EVAR was done before the TAVI for two reasons, namely; to avoid dissections that may be caused by advancing the stiff TAVI devices in a relatively tortuous aorta and to prevent aneurysmal rupture from the increased blood pressure following TAVI [5]. However, this technique needs extra precaution during deployment of the TAVI device over the stiff guide wire as it could deform or displace the aortic stent already in place.
Drury-Smith et al. reported combined percutaneous transfemoral procedure doing TAVI first using the 18 Fr CoreValve, then followed with a “drive-by” endovascular aortic repair [6]. We report a similar case and did TAVR first using a larger delivery system with 26 mm Sapien XT and then EVAR through the same open cut-down transfemoral access. We advocate doing TAVR first through this approach as the preferred method for one-setting combined TAVR and EVAR for severe AS with coexisting saccular abdominal aortic aneurysm.
This case highlights the importance of management strategy of a multi-disciplinary team of heart and vascular surgeons, interventional cardiologists and anesthesiologists as aortic stenosis become increasingly prevalent in an ageing population. The long-term result of this combined procedure is not known. Long-term follow-up is warranted.
Acknowledgements
The authors are grateful for the assistance of Elly Delaportas and the surgical nurses and technicians of the hybrid OR TAVR team, Vlad Chir for the fluoroscopic images, and Deborah Magnan and Ana Rivero-Ortiz for the literature search.References
- Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, et al. (2002) Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis. Circulation 106: 3006-3008.
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, et al. (2010) Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med 363: 1597-1607.
- Davis M, Taylor P (2008) Endovascular infrarenal abdominal aortic aneurysm repair. Heart 94: 222-228.
- Quader MA, Sawmiller C, Sumpio BA (1998) Contrast-induced nephropathy: review of incidence and pathophysiology. Ann Vasc Surg 12: 612-620.
- Yanes-Bowden G, Bosa-Ojeda F, del Castro-Madrazo JA, Laynez-Cerdeña I, Vargas-Torres MJ, et al. (2014) Simultaneous transfemoral aortic valve implantation and endovascular repair of abdominal aortic aneurysm. Rev Esp Cardiol (Engl Ed) 67: 408-409.
- Drury-Smith M, Garnham A, Khogali S (2012) Critical aortic stenosis in a patient with a large saccular abdominal aortic aneurysm: simultaneous transcatheter aortic valve implantation and drive-by endovascular aortic aneurysm repair. Catheter Cardiovasc Interv 80: 1014-1018.
- Gotzmann M, Hehen T, Germing A, Lindstaedt M, Yazar A, et al. (2010) Short term effects of transcatheter aortic valve implantation on neurohormonal activation, quality of life and 6 minute walk test in severe and symptomatic aortic stenosis. Heart 96: 1102-1106.
- Vorp DA, Raghavan ML, Webster MW (1998) Mechanical wall stress in abdominal aortic aneurysm: Influence of diameter and asymmetry. J Vasc Surg 27: 632-639.
- Durand E, Julia P, Blanchard D (2012) Transfemoral aortic valve implantation in a patient presenting with critical aortic stenosis and previously treated by endovascular aortic aneurysm repair. Heart 98: 1611-1612.