
Research Article
*Address for Correspondence: Birgul Bayoglu, Hacettepe University Children Hospital, Ankara, Turkey, Tel: 00903124275057; E-mail: bayoglu@hacettepe.edu.tr
Citation: Bayoglu B. Preschool Developmental Screening with Denver II Test in Semi-Urban Areas. J Pediatr Child Care. 2015;1(2): 4.
Copyright © 2015 Bayoglu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 1, Issue: 2
Submission: 29 October, 2015 | Accepted: 24 November, 2015 | Published: 30 November, 2015
Reviewed & Approved by: Dr. Jillian Childres, Assistant Professor of Pediatrics, Medical University of South Florida, USA
 Neurological evaluation revealed risk factors in past medical history of 3/6 children with abnormal and 3/8 children with suspect Denver II results. On examination, 1/6 with abnormal Denver II results had microcephaly and one child with suspect Denver II results was diagnosed as having mild cerebral palsy.
Neurological evaluation revealed risk factors in past medical history of 3/6 children with abnormal and 3/8 children with suspect Denver II results. On examination, 1/6 with abnormal Denver II results had microcephaly and one child with suspect Denver II results was diagnosed as having mild cerebral palsy.
 Re-testing with Denver II did not show significant difference from initial test (z=1.33, p=0.053). However 2/4 children with abnormal first test had a normal result on the second. 1/6 in the “suspect” category was abnormal and 3 remained “suspect”; two (33%) were normal on the second test.
Re-testing with Denver II did not show significant difference from initial test (z=1.33, p=0.053). However 2/4 children with abnormal first test had a normal result on the second. 1/6 in the “suspect” category was abnormal and 3 remained “suspect”; two (33%) were normal on the second test.
Preschool Developmental Screening with Denver II Test in Semi-Urban Areas
Emine Eratay1, Birgül Bayoglu2* and Banu Anlar2
- 1Izzet Baysal University, Faculty of Education, Special Education Department, Bolu, Turkey
- 2Hacettepe University Children Hospital, Ankara, Turkey
*Address for Correspondence: Birgul Bayoglu, Hacettepe University Children Hospital, Ankara, Turkey, Tel: 00903124275057; E-mail: bayoglu@hacettepe.edu.tr
Citation: Bayoglu B. Preschool Developmental Screening with Denver II Test in Semi-Urban Areas. J Pediatr Child Care. 2015;1(2): 4.
Copyright © 2015 Bayoglu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 1, Issue: 2
Submission: 29 October, 2015 | Accepted: 24 November, 2015 | Published: 30 November, 2015
Reviewed & Approved by: Dr. Jillian Childres, Assistant Professor of Pediatrics, Medical University of South Florida, USA
Introduction
The first few years of life have a crucial role in development and provide a time window when a supportive and stimulating environment can be most effective, and conversely when adverse factors can cause more pervasive damage. Developmental assessment and follow-up allow early detection of potential delays and early intervention. In spite of the importance of early recognition, parents and physicians may overlook mild or moderate delays in infancy and early childhood. Only 20-30% of developmental delays are diagnosed before school age [1]. Therefore developmental screening with standardized methods is recommended as part of routine follow-up of young children [2].Screening practices vary according to health care and social systems [3]. The Denver II Developmental Test is a practical observational screening test which has been standardized in many countries including Turkey [4-7]. Previous experience in children with various disorders support Denver II’s sensitivity in detecting adverse neurodevelopmental outcome [8-15]. On the other hand, its predictive value, concordance with school performance or with other tests, and the outcome of children detected by screening have been controversial [16,17].
This study intends to examine the feasibility and reliability of screening preschool children with Denver II in a semi-urban population by assessing developmental and neurological status. We also intended to examine methods to be used in the re-evaluation and referral of children who were found to have abnormal and suspect results on Denver II [18].
Materials and Methods
This is a longitudinal study using the approach of observation of cohorts. In the first phase, Denver II developmental screening test was applied to 583 children (305 girls and 278 boys, aged 3 months to 6 years, mean=3,5 years) who visited family physicians or other health centers in the province of Bolu, Turkey [19]. The latest standardization of the Denver II test for Turkey was used which consists of 134 items covering four developmental domains: personal-social, fine motoradaptive, language, and gross motor. Items are scored as “pass” or “fail” and the test is interpreted as normal, abnormal, or suspect [4]. In the cohort, 544 children had normal results; 26 results were suspect, 6 were abnormal, and 7 children were found untestable due to behavioral issues.In the second phase of the study, children with abnormal and suspect results were evaluated by neurological examination, Development Profile-3 (DP-3), repeat Denver II or Wechsler Intelligence Scales for Children-Revised (WISC-R) depending on the age of the child, and teacher’s perception of school performance and behavior within one year of the first phase. No intervention was intended during the study, and children went through the routine educational system as considered appropriate by their pediatricians and teachers between the two tests.
Neurological examination was performed by a pediatric neurologist (BA). Prenatal, natal and postnatal risk factors and family history were recorded using a standard form (Appendix A).
The DP-3 is a questionnaire covering four developmental areas: cognitive, language-communication, movement and social-adaptive [19]. Questions are answered as “yes” or “no” during interview with the parents. Each interview lasts 20-40 minutes. The DP-3 items’ translation to Turkish was used for this pilot study. As a control group, DP-3 was also applied to a subgroup of children who tested normal on first Denver II (referred hereafter as “normal Denver II” n=30).
The WISC-R is a widely used psychometric test for 6-16 years consisting of 12 sub-tests covering verbal and performance skills. The test was adapted to Turkey [20]. A score between 70 and 90 is considered “ low average ”, 90-110 as “normal” and 110-130, “above average”. WISC-R was applied to children >6 years old by a certified psychologist at Bolu Counseling and Investigation Center attached to the Ministry of National Education.
Teacher interviews were conducted using semi-quantitative questionnaires inquiring about school grades, peer relations, attention, and behavior designed for this study by the authors in collaboration with three specialists of classroom teaching, special education and program development (Appendix B). Questionnaires were filled out during structured interviews of the author (EA) with the grade school teacher and scored as “below average”, “normal”, and “above average”. As a control group, the questionnaire was also applied to 30 children with normal initial Denver II attending the same schools.
Data analysis
Relationships were investigated between the initial Denver II screening test results and neurological examination findings, neurological risk factors, DP-3, repeat Denver II test results for children < 6 years old, WISC-R results for children >6 years old; domains of failure in the first and second Denver II tests; and data obtained from families and teachers regarding school performance, behavior and attention. Wilcoxon signed rank test and Mann-Whitney test were used in the analysis of quantitative data [21].
Results
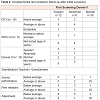
Demographic characteristics of the cohort are summarized in Table 1. Of the 32 children with suspect and abnormal Denver II results, a total of 18 (56%) children were re-examined, (6 with abnormal and 12 with suspect results), the other 14 children moved to other cities (n=12) or decline to participate (n=2). There were 11 girls (61%) and 7 boys (39%); 8 of the children were over 6 (44%) and 10,were under 6 years old (56%). Mean age was 3.1 years (3-70 months) in the first and 6.0 years (44-105 months) in the second phase of the study.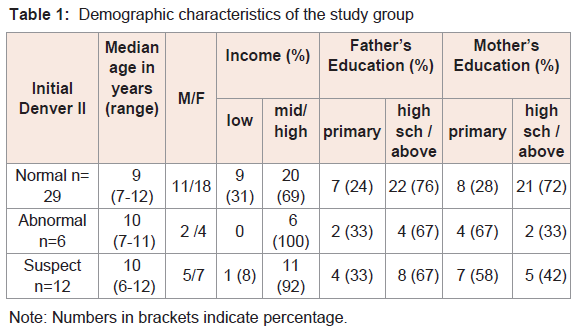
Table 1: Demographic characteristics of the study group.
DP-3 was given to 6 children with abnormal initial Denver II and 12 children with suspect Denver II. DP-3 results were average or above (4/6) or low average (2/6) in the abnormal Denver II group and average (9/12) or below average (3/12) in the suspect Denver II group, (Table 2) (p: n.s.), both different from the “normal Denver II” sample (average or above in 30/30).
The WISC-R was administered with 8 children: of the 2 children with abnormal initial screening with Denver II, one was below average and the other was average; of those with suspect Denver II, 5/6 were average or above (Table 2).
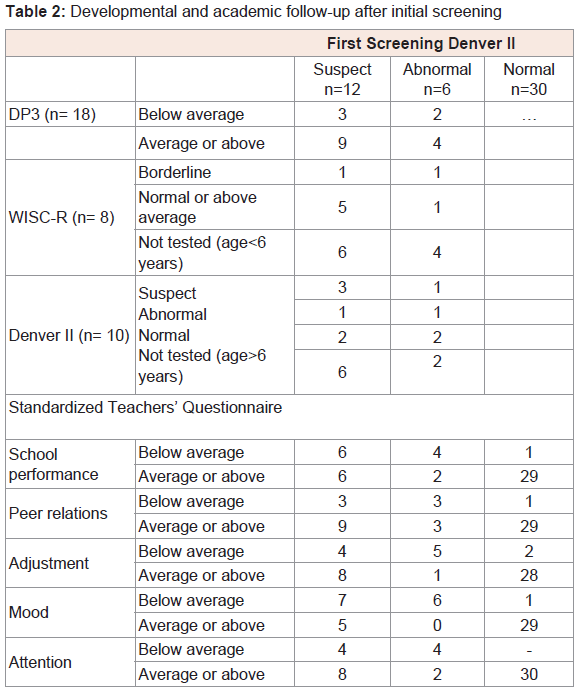
Table 2: Developmental and academic follow-up after initial screening.
In the 18 children with abnormal (n=6) or suspect (n=12) results on the first Denver II who were school age and attending school, teachers’ evaluation was significantly more likely to score “under average classroom level” in all areas compared to a sample of children attending the same schools who had normal initial Denver II (Table 2).
Discussion
Developmental delays have a prevalence between 3-25% in the first 6 years of life and constitute one of the most frequent problems in children, especially in those under adverse environmental conditions. Developmental screening is therefore recommended in the care of all children by the American Academy of Pediatrics [2]. The choice of methods vary between centers: for clinical purposes, they include parent questionnaires, observational tests, and most commonly, the physician’s general impression although the latter detects only 30% of delays [1].Questionnaires are subjective methods of evaluation varying according to the age and gender of the child, the presence of parental concern, and factors pertaining to the physician. They may be costeffective in a busy outpatient clinic, but direct observation is more reliable in rural areas and shows greater agreement with standardized tests [22,23]. Observational tests are not used routinely by physicians due to time, training and reimbursement issues [1,24,25]. Denver II is an observational screening test which has the advantage of being practical for use by community health workers, nurses and child care providers. Studies evaluating Denver II in comparison with other screening methods demonstrated good correlation with CAT/CLAMS, another observational tests, and with the Ages and Stages Questionnaire (ASQ), an interview-based tool [26,27].The proportion of children found to have abnormal or suspect results at initial screening was 39/583 (6.6%) in our study. This rate varies between 15-25% depending on the population and screening method [1,24]. The reason for the lower rate in our study may be the relatively wide age range and low risk of our population collected from day care centers and family physician’s offices.
Few studies investigated the outcome of developmental screening in the population of reportedly normal children. We intended to examine the results of re-evaluation in children with abnormal and suspect initial Denver II and applied different instruments in order to optimize the methods for second look in our population. We reapplied the Denver II if the child was under 6 years of age at second look. Comparison of the first and second Denver II results showed some suspect or abnormal results persisted but others (2/12 and 2/6 respectively) improved to normal. This fact might indicate “catchingup,”, adverse factors being corrected in the interim period, or just a false-positive initial result; it supports the general recommendation of initial screening be verified and followed-up.
Of those tested with DP-3 done after age 6 years, 2/6 with suspect and 3/12 with abnormal Denver II had low DP-3 scores despite the time elapsed and the routine developmental interventions given between these two tests. Whether more specific and intense developmental intervention would be more efficient in this group needs to be studied further.
Children over 6 years of age at second evaluation were tested with WISC-R. We previously observed that children with normal Denver II at ages 5-6 years had an average IQ of 90 on WISC-R [28]. In the current study, WISC-R was normal or superior in 5/6 children with suspect and 1 of 2 with abnormal initial Denver II. Discrepancy between a developmental screening test and a cognitive test like the WISC-R is expected because the Denver II evaluates global development including gross motor items, and has a lower index of suspicion as appropriate for a screening test.
Children with abnormal and suspect Denver II results had similar rates of abnormality or neurological risk factor in their historyies. This suggests the Denver II might complete or support the neurological examination, and suspect results should also be followed-up as abnormal ones. The Denver II test has been used jointly with neurological examination especially in infants with perinatal risk factors: and these studies showed that the Denver II results at 6 months had good concordance with the neurological examination at 12 months [29-31].
School performance was assessed in a semi-objective manner in our study, which constitutes one of its limitations. Because standard, universally accepted tests are not available at primary school level, we designed a standardized questionnaire for the teacher about classroom performance. Teachers’ opinion has been shown as a reliable method of evaluation: primary grade teacher ratings are at least as predictive of subsequent learning problems as standardized cognitive tests [32]. Children with abnormal initial Denver II results, when attending regular school, were highly likely to be below class level (4/6). Likewise, Cadman et al. observed children with positive preschool Denver Developmental Screening Tests had substantially more school problems three years after screening [32]. Poor school performance has also been reported earlier in 6 year-old children with abnormal Denver Developmental Screening Test [33]. On the other hand those with suspect results did not differ from class level. This might suggest the “suspect” category on the Denver II contains a high rate of false-positives and could be considered as “normal”. However, this group might still be candidate for school problems on longer follow-up [34]. Our previous studies showed children with both abnormal and suspect results on the Denver II tended to show low performance in their first year at school, but test results and school performance improved at the end of the first school year [30]. This is probably due to schooling providing the child with opportunity to develop the skills measured in the Denver II, and mitigating the adverse environmental impacts of deprived environment. Children in the current study had not received kindergarten education yet at their second evaluation: so it is possible that their results might improve if tested after attending school.
A selection bias favoring the study group is possible but unlikely because the demographic data of the groups with normal and abnormal Denver II results and of those who could and could not be reached after the first survey were similar, and because the most common reason for unavailability was re-location of the family. The main limitation of the study is lack of systematic follow-up in the normal Denver II group, especially for school problems.
According to our study, early screening followed by further evaluation within one year is feasible even in a region with high population mobility. In this study more than half (56%) of the target population could be reached. Higher rates can be achieved in areas with a more stable population, but coverage at school entry can be less than adequate even in countries with more developed health and education systems. In the UK, only 57% of 400 children invited for a health interview could be examined in the presence of a parent [35]. Our pilot study suggests preschool screening with the Denver II and re-evaluation of children with abnormal and suspect test results for global development and school performance appears useful in our population, the administration of the test is practical for workers in health care and education, and that early detection of various degrees of school problems is feasible.
Acknowledgement
This work was partially supported by the Developmental Child Neurology Society (GNCD), Ankara, Turkey.References
- Sand N, Silverstein M, Glascoe FP, Gupta VB, Tonniges TP, et al. (2005) Pediatricians' reported practices regarding developmental screening: do guidelines work? Do they help? Pediatrics 116: 174-179.
- Foy JM, American Academy of Pediatrics Task Force on Mental Health (2010) Enhancing pediatric mental health care: report from the American Academy of Pediatrics Task Force on Mental Health. Introduction. Pediatrics 125 Suppl 3: S69-S74.
- Sabol TJ, Pianta RC (2012) Patterns of school readiness forecast achievement and socioemotional development at the end of elementary school. Child Dev 83: 282-299.
- Frankenburg WK, Dodds J, Archer P, Shapiro H, Bresnick B (1992) The Denver II: a major revision and restandardization of the Denver Developmental Screening Test. Pediatrics 89: 91-97.
- Wijedasa D (2011) Developmental screening in context: adaptation and standardization of the Denver Developmental Screening Test-II (DDST-II) for Sri Lankan children. Child Care Health Dev 38: 889-899.
- Lim HC, Chan T, Yoong T (1994) Standardisation and adaptation of the Denver Developmental Screening Test (DDST) and Denver II for use in Singapore children. Singapore Med J 35: 156-160.
- Durmazlar N, Ozturk C, Ural B, Karaagaoglu E, Anlar B (1998) Turkish children's performance on Denver II: effect of sex and mother's education. Dev Med Child Neurol 40: 411-416.
- Gaylord N, Chyka DL, Lawley G (2012) Developmental evaluation of preschool children: a service-learning experience for nursing students. J Nurs Educ 51: 710-713.
- Polat S, Okuyaz C, Hallioğlu O, Mert E, Makharoblidze K (2011) Evaluation of growth and neurodevelopment in children with congenital heart disease. Pediatr Int 53: 345-349.
- Elmahdy H, El-Mashad AR, El-Bahrawy H, El-Gohary T, El-Barbary A, et al. (2010) Human recombinant erythropoietin in asphyxia neonatorum: pilot trial. Pediatrics 125: 1135-1142.
- Schatz J, McClellan CB, Puffer ES, Johnson K, Roberts CW (2008) Neurodevelopmental screening in toddlers and early preschoolers with sickle cell disease. J Child Neurol 23: 44-50.
- Mirrett PL, Bailey DB Jr, Roberts JE, Hatton DD (2004) Developmental screening and detection of developmental delays in infants and toddlers with fragile X syndrome. J Dev Behav Pediatr 25: 21-27.
- Schirmer CR, Portuguez MW, Nunes ML (2006) Clinical assessment of language development in children at age 3 years that were born preterm. Arq Neuropsiquiatr 64: 926-931.
- Tur BS, Küçükdeveci AA, Kutlay S, Yavuzer G, Elhan AH, et al. (2009) Psychometric properties of the WeeFIM in children with cerebral palsy in Turkey. Dev Med Child Neurol 51: 732-738.
- Aly H, Khashaba MT, Nada A, Hasanen BM, McCarter R, et al. (2009) The role of complement in neurodevelopmental impairment following neonatal hypoxic-ischemic encephalopathy. Am J Perinatol 26: 659-665.
- Glascoe FP, Byrne KE, Ashford LG, Johnson KL, Chang B, et al. (1992) Accuracy of the Denver-II in developmental screening. Pediatrics 89: 1221-1225.
- Johnson KL, Ashford LG, Byrne KE, Glascoe FP (1992) Does Denver II produce meaningful results? Pediatrics 90: 477-479.
- Theeranate K, Chuengchitraks S (2005) Parent's Evaluation of Developmental Status (PEDS) detects developmental problems compared to Denver II. J Med Assoc Thai 88: 188-192.
- Alpern GD (2007) Developmental Profile 3 (DP-3) Manual. A WPS Test Report. California: Western Psychological Services.
- Savasir I, Sahin N (1995) Wechsler İntelligence Scale for Children-Revised (WISC-R) Turkish Handbook. Ankara: Turkish Psychological Association Publications.
- Ensor R, Devine RT, Marks A, Hughes C (2013) Mothers' cognitive references to two-year-olds predict theory of mind at ages 6 and 10. Child Dev 85: 1222-1235.
- Voigt RG, Llorente AM, Jensen CL, Fraley JK, Barbaresi WJ, et al. (2007) Comparison of the validity of direct pediatric developmental evaluation versus developmental screening by parent report. Clin Pediatr (Phila) 46: 523-529.
- Brachlow A, Jordan AE, Tervo R (2001) Developmental screenings in rural settings: a comparison of the child development review and the Denver II Developmental Screening Test. J Rural Health 17: 156-159.
- Guevara JP, Gerdes M, Localio R, Huang YV, Pinto-Martin J, et al. (2013) Effectiveness of developmental screening in an urban setting. Pediatrics 131: 30-37.
- Ertem IO, Pekcici EB, Gok CG, Ozbas S, Ozcebe H, et al. (2009) Addressing early childhood development in primary health care: experience from a middle-income country. J Dev Behav Pediatr 30: 319-326.
- Bruck I, Tahan TT, Cruz CR, Martins LT, Antoniuk SA, et al. (2001) Developmental milestones of vertically HIV infected and seroreverters children - Follow up of 83 children. Arq Neuro-Psiquiatr 59: 691-695.
- Woodward BJ, Papile LA, Lowe JR, Laadt VL, Shaffer ML, et al. (2011) Use of the ages and stages questionnaire and Bayley Scales of Infant Development-II in neurodevelopmental follow-up of extremely low birth weight infants. J Perinatol 31: 641-646.
- Bayoglu BU, Bakar EE, Kutlu M, Karabulut E, Anlar B (2007) Can preschool developmental screening identify children at risk for school problems? Early Hum Dev 83: 613-617.
- Oygür N, Sönmez O, Saka O, Yeğin O (1998) Predictive value of plasma and cerebrospinal fluid tumour necrosis factor-alpha and interleukin-1 beta concentrations on outcome of full term infants with hypoxic-ischaemic encephalopathy. Arch Dis Child Fetal Neonatal Ed 79: F190-F193.
- Aly H, Khashaba MT, El-Ayouty M, El-Sayed O, Hasanein BM (2006) IL-1beta, IL-6 and TNF-alpha and outcomes of neonatal hypoxic-ischemic encephalopathy. Brain Dev 28: 178-182.
- Liu J, Feng ZC (2010) Increased umbilical cord plasma interleukin-1 beta levels was correlated with adverse outcomes of neonatal hypoxic-ischemic encephalopathy. J Trop Pediatr 56: 178-182.
- Cadman D, Chambers LW, Walter SD, Feldman W, Smith K, et al. (1984) The usefulness of the Denver Developmental Screening Test to predict kindergarten problems in a general community population. Am J Public Health 74: 1093-1097.
- Greer S, Bauchner H, Zuckerman B (1989) The Denver Developmental Screening Test: how good is its predictive validity? Dev Med Child Neurol 31: 774-781.
- Glascoe FP (2001) Are overreferrals on developmental screening tests really a problem? Arch Pediatr Adolesc Med 155: 54-59.
- Laing GJ, Rossor EB (1999) ‘Health assessment’ at school entry: performance of a system based on school nurse interviews. Child Care Health and Dev 25: 421-428.