
Case Report
*Address for Correspondence: Roger Kurlan, Atlantic Neuroscience Institute, Overlook Medical Center, 99 Beauvoir Ave. Summit, NJ 07901, USA, Tel: 908-522-2089; Fax: 908-522-6147; E-mail: roger.kurlan@atlantichealth.org
Citation: Wolf A, Earnhardt MC, Rabin ML, Ganihong I, Kurlan R. Possible Migraine-Associated Parkinsonism. J Parkinsons Dis Alzheimer Dis. 2016;3(1):3.
Copyright © 2016 Wolf A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Parkinson’s disease & Alzheimer’s disease| ISSN: 2376-922X | Volume: 3, Issue:1
Submission: 09 February, 2016 | Accepted: 07 March, 2016 | Published: 13 March, 2016
 Case 2: This 66-year-old woman has been experiencing severe frontal migraines since age 27. She has visual auras of transient complete blindness and associated symptoms of yawning, nausea, and photophobia. Previous treatments include zolmitriptan, butalbital, hydrocodone, and ondansetron. Current treatment includes topiramate (100 mg/day), aspirin (1000 mg/day), nortriptyline (100 mg/day), and botulinum neurotoxin injections into the face and neck muscles. She previously averaged 6-8 migraine days per month but improved to 1-2 migraine days per month with the current therapy. At age 60, she developed resting and action tremor with impaired dexterity of the left hand. The tremor became bilateral and she developed micrographia, stooped posture, bradykinesia, and dystonia of the feet and hands. There was no history of RSBD or cardiac or peripheral vascular disease, and she had no vascular risk factors. MRI of the brain (unavailable) was reported to show bifrontal subcortical microvascular changes consistent with migraine.
Case 2: This 66-year-old woman has been experiencing severe frontal migraines since age 27. She has visual auras of transient complete blindness and associated symptoms of yawning, nausea, and photophobia. Previous treatments include zolmitriptan, butalbital, hydrocodone, and ondansetron. Current treatment includes topiramate (100 mg/day), aspirin (1000 mg/day), nortriptyline (100 mg/day), and botulinum neurotoxin injections into the face and neck muscles. She previously averaged 6-8 migraine days per month but improved to 1-2 migraine days per month with the current therapy. At age 60, she developed resting and action tremor with impaired dexterity of the left hand. The tremor became bilateral and she developed micrographia, stooped posture, bradykinesia, and dystonia of the feet and hands. There was no history of RSBD or cardiac or peripheral vascular disease, and she had no vascular risk factors. MRI of the brain (unavailable) was reported to show bifrontal subcortical microvascular changes consistent with migraine.
Two Patients with Migraine and Parkinsonism: A Possible Relationship?
Allyson Wolf, Mary Cathryn Earnhardt, Marcie L.Rabin, Ivana Ganihong and Roger Kurlan*
- Atlantic Neuroscience Institute, Overlook Medical Center, 99 Beauvoir Ave. Summit, NJ 07901, USA
*Address for Correspondence: Roger Kurlan, Atlantic Neuroscience Institute, Overlook Medical Center, 99 Beauvoir Ave. Summit, NJ 07901, USA, Tel: 908-522-2089; Fax: 908-522-6147; E-mail: roger.kurlan@atlantichealth.org
Citation: Wolf A, Earnhardt MC, Rabin ML, Ganihong I, Kurlan R. Possible Migraine-Associated Parkinsonism. J Parkinsons Dis Alzheimer Dis. 2016;3(1):3.
Copyright © 2016 Wolf A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Parkinson’s disease & Alzheimer’s disease| ISSN: 2376-922X | Volume: 3, Issue:1
Submission: 09 February, 2016 | Accepted: 07 March, 2016 | Published: 13 March, 2016
Abstract
Migraine is linked to an increased occurrence of neurological movement disorders including Parkinsonism. We describe two women with chronic, severe migraine with aura who later in life developed Parkinsonism. In both cases, brain neuroimaging showed sub cortical micro vascular changes characteristic of migraine. Notably, both cases also have family histories of migraine and Parkinsonism, suggesting a genetic contribution. Chronic migraine may promote Parkinsonism by vascular mechanisms, though abnormalities in dopamine neurotransmission and brain iron deposition may also play a role. Longstanding and severe migraine with aura may be a factor in the development of Parkinsonism, particularly in women.Keywords
Migraine; Headache; Parkinsonism; Parkinson’s disease; Vascular parkinsonismIntroduction
A number of studies have identified an increased frequency of migraine in association with certain movement disorders including essential tremor, Tourette’s syndrome, Sydenham’s chorea, and restless legs syndrome [1]. The recently published AGES-Reykjavik population-based cohort study found that individuals with midlife migraine, particularly those with aura, were more likely to report parkinsonian symptoms and/or be diagnosed with Parkinson’s disease (PD) later in life compared to controls [2]. Also, women experiencing migraine with aura were more likely to have a parent or sibling with PD. We now describe two patients with longstanding, severe migraine headaches with aura who later also developed Parkinsonism, and we discuss a potential etiological role for migraine in this process.Report of Cases
Case 1: This 71 year-old woman has been experiencing severe, monthly migraines since age 11. These migraines are described as pressure headaches in the forehead that occur following intense, 20-30 minute visual auras. Associated symptoms include nausea, photophobia, and exhaustion. Due to side effects, she avoids medications to treat the migraines and instead, sleeps during the episodes (5-7 hours). She developed right hand resting tremor, micrographia, and imbalance at age 68 and was diagnosed with PD. There was no history of rapid eye movement sleep behavior disorder (RSBD) or cardiac or peripheral vascular disease, and she had no vascular risk factors. Magnetic resonance imaging (MRI) of the brain showed generalized atrophy with microvascular ischemic abnormalities of the basal ganglia and periventricular white matter (Figure 1). Over time, she developed bilateral Parkinsonism, depression, cognitive impairment, and after three years, druginduced visual hallucinations. Levodopa (450 mg/day) produces only modest benefit and does not influence migraine symptoms. Both the patient’s mother and maternal first cousin experienced chronic, severe migraines and were also diagnosed with PD.
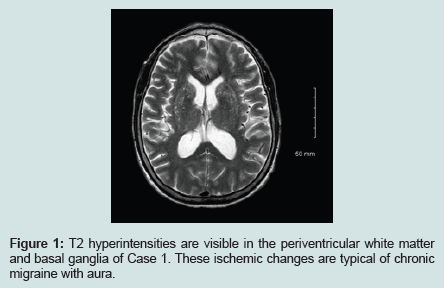
Figure 1: T2 hyperintensities are visible in the periventricular white matter and basal ganglia of Case 1. These ischemic changes are typical of chronic migraine with aura.
She was diagnosed with possible vascular Parkinsonism. Her motor problems improved with levodopa (450 mg/day) and symptoms have remained fairly stable over four years of observation. Levodopa therapy does not influence her symptoms of migraine. The patient’s mother was diagnosed with essential tremor and her paternal grandmother was diagnosed with PD. Her daughter has chronic migraines.
Discussion
We have presented two cases of women with longstanding, severe migraine with aura who later developed Parkinsonism. Although these conditions may have arisen independently, it is possible that migraine has an etiological role in the appearance of Parkinsonism. Perhaps the most likely mechanism by which migraine could induce Parkinsonism is through vascular processes. Current understanding of the pathophysiology of migraine points to a vasculopathic process. Activation of the trigeminovascular system and the subsequent release of calcitonin gene-related peptide is thought to cause migraine headache and its associated symptoms [3]. Aura is thought to be the result of cortical spreading depression accompanied by an initial increase, followed by a sustained decrease, in local cerebral blood flow [3]. Thus, the presence of aura points to an ischemic process.A wide range of vascular diseases have been associated with migraine, in particular migraine with aura, independent of any other singular vascular risk factor [4]. Included are myocardial infarction, stroke, subclinical stroke-like brain lesions, and white matter hyperintensities [5]. Recently, analyses of two genome-wide association studies revealed a shared set of genetic loci between migraine and coronary artery disease [6]. Our two cases had family histories of migraine and Parkinsonism, suggesting a genetic contribution.
Regions of focal white matter hyperintensities, like those observed in our cases, are the most frequently seen abnormality on brain magnetic resonance imaging (MRI) of patients with migraine [7], with an increased prevalence of such lesions among females [8]. These deep white matter lesions have been ascribed to either microvascular ischemic disturbances, impaired clearance or relocation of embolitic particles [7,8] or migraine-associated endothelial dysfunction in combination with platelet aggregation [9]. MRI studies have shown that the vascular abnormalities caused by repeated migraine attacks can be cumulative and that higher number of lesions is seen more often in migraine with higher frequency [10]. We conclude that these findings suggest that migraine can be a progressive disorder capable of causing advancing damage to the brain. It is then reasonable to conclude that chronic migraine may result in sufficient cumulative small vessel cerebrovascular damage to induce progressive conditions such as Vascular Parkinsonism (VP).
Vascular parkinsonism (VP) can mimic the features of PD [11,12] and is a possible diagnosis for our patients, mainly due to the neuroimaging signs of small vessel cerebrovascular disease, compatible clinical features, and the strong history of migraine, a known vasculopathic condition. Though typically attributed to small vessel atherosclerotic or hypertensive cerebrovascular disease affecting the basal ganglia, our cases suggest that migraine may play an etiologic role in the development of VP. However, we cannot exclude a diagnosis of idiopathic PD as VP and PD are not mutually exclusive diagnoses. Studies have suggested that between 1-3% of patients clinically diagnosed with PD are found to instead have VP at autopsy, and 20-30% of patients are found to have both pathologies [12]. Migraine appears to be a possible cause for VP in our cases given that the neuroimaging features seen are commonly observed in patients with migraine [7,8], migraine has been linked to cerebrovascular brain damage, neither patient had typical vascular risk factors, and our patients had particularly severe and/or long lasting migraine. In addition, neither of our cases had RSBD, which is commonly associated with synucleinopathies, perhaps making idiopathic PD less likely.
Diffuse subcortical white matter lesions have been observed in up to 88% of patients with VP, and generalized brain atrophy has been seen in up to 69% of cases [12]. The white matter changes associated with VP are thought to represent regions of chronic or periodic partial ischemia [11], as occurs with chronic migraine. Vascular Parkinsonism appears to progress faster when the white matter lesions occur within the periventricular and deep subcortical regions [13]. Lesions in these areas may disrupt the fiber tracts connecting the basal ganglia and the motor cortex, thereby inhibiting the striatothalamocortical motor system and causing Parkinsonism [14].
The modest degree of microvascular pathology as assessed by MRI raises questions about purely vascular mechanisms. Consideration should also be given to dopaminergic processes, as dopamine has long been considered to play a complex role in the pathophysiology of migraine [15]. Symptoms associated with migraine such as excessive yawning, nausea, and vomiting may be related to dopaminergic stimulation, and pharmacologic studies suggest that migraine patients have increased sensitivity to dopamine agonists [16]. However, the nature of the dopamine abnormalities that may link migraine and Parkinsonism remains unclear. Our cases reported no change in their migraine symptoms in response to levodopa therapy.
Another potential mechanism through which migraine may induce parkinsonism relates to brain iron metabolism [2]. Brain imaging studies have found that, when compared to controls without migraine, chronic migraine is associated with an increased accumulation of free iron within deep brain nuclei [8,17]. This may occur in response to the recurrent activation of nociceptive networks during migraine attacks, resulting in increased free radical damage in this region [18]. Increased iron accumulation in the substantia nigra has consistently been reported in association with PD [19] and it has been proposed that iron induces oxidative stress and dopaminergic neuronal death as a major component of the neurodegenerative process in PD [19]. Also, under oxidative conditions, iron more readily binds α-synuclein, resulting in accelerated aggregation. This interaction causes the accumulated iron to enter a redox active state in the cytosol, resulting in elevated free radical levels and oxidative damage [20]. In this way, deep brain iron accumulation in association with chronic migraine could induce Parkinsonism on a neurodegenerative basis. It is possible that all three mechanisms, vascular, dopamine-related, and iron deposition-related, may coexist in chronic migraine to contribute to the development of Parkinsonism.
In conclusion, chronic, severe migraine, particularly in women and those with aura, might contribute to the development of Parkinsonism later in life. While a disturbance of cerebral blood flow may be the most likely mechanism, changes in dopamine neurotransmission and increased deposition of deep brain iron may also be involved. The positive family histories in our cases suggest that hereditary factors may be important and that future genetic studies would likely be of value.
References
- d’Onofrio F, Barbanti P, Petretta V, Casucci G, Mazzeo A, et al. (2012) Migraine and movement disorders. Neurol Sci 33 Suppl 1: S55-S59.
- Scher AI, Ross GW, Sigurdsson S, Garcia M, Gudmundsson LS, et al. (2014) Midlife migraine and late-life parkinsonism: AGES-Reykjavik study. Neurology 83: 1246-1252.
- Ferrari MD, Klever RR, Terwindt GM, Ayata C, van den Maagdenberg AM (2015) Migraine pathophysiology: lessons from mouse models and human genetics. Lancet Neurol 14: 65-80.
- Sacco S, Pistoia F, Degan D, Carolei A (2015) Conventional vascular risk factors: their role in the association between migraine and cardiovascular diseases. Cephalalgia 35: 146-164.
- Schurks M, Rist PM, Bigal ME, Buring JE, Lipton RB, et al. (2009) Migraine and cardiovascular disease: systematic review and meta-analysis. BMJ 339: b3914.
- Winsvold BS, Nelson CP, Malik R, Gormley P, Anttila V, et al. (2015) Genetic analysis for a shared biological basis between migraine and coronary artery disease. Neurol Genet 1: e10.
- Colombo B, Dalla Libera D, Comi G (2011) Brain white matter lesions in migraine: what’s the meaning? Neurol Sci 32 Suppl 1: S37-S40.
- Kruit MC, Van Buchem MA, Launer LJ, Terwindt GM, Ferrari MD (2009) Migraine is associated with an increased risk of deep white matter lesions, subclinical posterior circulation infarcts and brain iron accumulation: the population based MRI CAMERA study. Cephalalgia 30: 129-136.
- Tietjen GE (2009) Migraine as a systemic vasculopathy. Cephalalgia 29: 987-996.
- Lipton RB, Pan J (2004) Is migraine a progressive brain disease? JAMA 291: 493-494.
- Balash Y, Korczyn AD (2007) Vascular parkinsonism. Handb Clin Neurol 84: 417-425.
- Sibon I, Fenelon G, Quinn NP, Tison F (2004) Vascular parkinsonism. J Neurol 251: 513-524.
- Chang CM, Yu YL, Ng HK, Leung SY, Fong KY (1992) Vascular pseudoparkinsonism. Acta Neurol Scand 86: 588-592.
- de Laat KF, van Norden AG, Gons RA, van Uden IW, Zwiers MP, et al. (2012) Cerebral white matter lesions and lacunar infarcts contribute to the presence of mild parkinsonian signs. Stroke 43: 2574-2579.
- Charbit AR, Akerman S, Goadsby PJ (2010) Dopamine: what’s new in migraine? Curr Opin Neurol 23: 275-281.
- Barbanti P, Fofi L, Aurilia C, Egeo G (2013) Dopaminergic symptoms in migraine. Neurol Sci 34 Suppl 1: S67-S70.
- Kruit MC, Launer LJ, Overbosch J, van Buchem MA, Ferrari MD (2009) Iron accumulation in deep brain nuclei in migraine: a population-based magnetic resonance imaging study. Cephalalgia 29: 351-359.
- Welch KM (2009) Iron in the migraine brain; a resilient hypothesis. Cephalalgia 29: 283-285.
- Dexter DT, Wells FR, Lees AJ, Agid F, Agid Y, et al. (1989) Increased nigral iron content and alterations in other metal ions occurring in brain in Parkinson’s disease. J Neurochem 52: 1830-1836.
- Wolozin B, Golts N (2002) Iron and Parkinson’s disease. Neuroscientist 8: 22-32.