
Research Article
*Address for Correspondence: Dr. Rosalyn Lang, Ph.D, Assistant Professor, North Carolina A & T State University, Department of Biology 1601 East Market Street, Greensboro, NC 27411, USA, Tel: (336) 285-2158; Fax: (336) 256-2743; E-mail: rlangwal@ncat.edu
Dr. Goldie S. Byrd, Ph.D, Professor of Biology and Dean for the College of Arts and Sciences at North Carolina A&T State University; 1601 East Market Street, A411 General Classroom Building, Greensboro, NC 27411,USA, Tel: (336) 334-7806 ; Fax: (336) 334-7173.
Citation: Lang R, Kelkar VA, Byrd JR, Starks T, Edwards CL, et al. Beyond the Barriers: Factors that Influence African Americans to Participate in Research. J Parkinsons Dis Alzheimer Dis. 2014;1(1): 4.
Copyright © 2014 Lang et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Parkinson’s disease and Alzheimer's disease | ISSN: 2376-922X | Volume: 1, Issue: 1
Submission: 15 October 2014 | Accepted: 08 December 2014 | Published: 10 December 2014
 In order to determine if any particular types of research studies may be avoided by this cohort, we asked “what type of health-related for selection which included survey, focus groups, clinical trials, blood/genetic studies, and other. Each participant was able to select all studies that applied to their research experiences. More than 45% of participants have participated in research requiring survey completion and more than 30% had participated in clinical trials. No category was left blank; however, the focus groups option was the lowest selected of all the choices. Table 2 also shows results from the question “If you gave a sample, what type of sample was collected?” Of the 101 participants that responded to these questions, 64% responded that a sample was collected, and 84% indicated the type of sample that was given during the health related research study. Twenty-one (18%) of the 119 participants had not given a sample, but stated they would still participate if they had to give a sample. Blood was the sample that was reported to be given the most; however, responses were recorded in all categories. We asked “What motivated you to participate in the study?” The choices included relative with disease, I have/had the disease, monetary compensation, civic duty, and other. Having a relative with the disease appeared to be the greatest motivator for participation. However, there was not a significant difference across selections and categories of age, gender and education level. Less than 20 (40%) out of 50 participants, who responded to this question, had received monetary compensation. Monetary compensation was the least selected motivator for participation across every category in age, gender and education level. There are no significant differences among these motivations across age, gender or education level groups. Again, the studies for participation were varied and included Alzheimer’s, Allergies, Asthma, Arthritis, Blood, Bone Marrow, Cancer Obesity, Blood Pressure, HIV/AIDS, Diabetes, Stroke, etc.
In order to determine if any particular types of research studies may be avoided by this cohort, we asked “what type of health-related for selection which included survey, focus groups, clinical trials, blood/genetic studies, and other. Each participant was able to select all studies that applied to their research experiences. More than 45% of participants have participated in research requiring survey completion and more than 30% had participated in clinical trials. No category was left blank; however, the focus groups option was the lowest selected of all the choices. Table 2 also shows results from the question “If you gave a sample, what type of sample was collected?” Of the 101 participants that responded to these questions, 64% responded that a sample was collected, and 84% indicated the type of sample that was given during the health related research study. Twenty-one (18%) of the 119 participants had not given a sample, but stated they would still participate if they had to give a sample. Blood was the sample that was reported to be given the most; however, responses were recorded in all categories. We asked “What motivated you to participate in the study?” The choices included relative with disease, I have/had the disease, monetary compensation, civic duty, and other. Having a relative with the disease appeared to be the greatest motivator for participation. However, there was not a significant difference across selections and categories of age, gender and education level. Less than 20 (40%) out of 50 participants, who responded to this question, had received monetary compensation. Monetary compensation was the least selected motivator for participation across every category in age, gender and education level. There are no significant differences among these motivations across age, gender or education level groups. Again, the studies for participation were varied and included Alzheimer’s, Allergies, Asthma, Arthritis, Blood, Bone Marrow, Cancer Obesity, Blood Pressure, HIV/AIDS, Diabetes, Stroke, etc.

Beyond the Barriers: Factors that Influence African Americans to Participate in Research
Rosalyn Lang1*, Vinaya A. Kelkar2, Jennifer R. Byrd1, Takiyah Starks1, Christopher L. Edwards3 and Goldie S. Byrd1*
- 1Department of Biology, North Carolina, A&T State University,USA 2Department of Mathematics & Statistics, Elon University, USA 3Duke Pain Medicine, Medical Director, Biofeedback Laboratory and Director, Chronic Pain Management Program, Durham, NC, USA
*Address for Correspondence: Dr. Rosalyn Lang, Ph.D, Assistant Professor, North Carolina A & T State University, Department of Biology 1601 East Market Street, Greensboro, NC 27411, USA, Tel: (336) 285-2158; Fax: (336) 256-2743; E-mail: rlangwal@ncat.edu
Dr. Goldie S. Byrd, Ph.D, Professor of Biology and Dean for the College of Arts and Sciences at North Carolina A&T State University; 1601 East Market Street, A411 General Classroom Building, Greensboro, NC 27411,USA, Tel: (336) 334-7806 ; Fax: (336) 334-7173.
Citation: Lang R, Kelkar VA, Byrd JR, Starks T, Edwards CL, et al. Beyond the Barriers: Factors that Influence African Americans to Participate in Research. J Parkinsons Dis Alzheimer Dis. 2014;1(1): 4.
Copyright © 2014 Lang et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Parkinson’s disease and Alzheimer's disease | ISSN: 2376-922X | Volume: 1, Issue: 1
Submission: 15 October 2014 | Accepted: 08 December 2014 | Published: 10 December 2014
Abstract
The objective of the paper is to describe educational profiles and motivations for health related research study participation of a distinct minority cohort, in a non-clinical setting. Many respondents (n=119) participated in at least two studies and reported that the main motivator was having a relative with the studied disease. More than 65% of this cohort had earned a bachelor degree or higher compared to 40% of those that had not participated in a health related research study. This study also documented that African Americans who participate in health related research studies are civic minded individuals that understand informed consent and are willing to submit a variety of biological samples for research.Introduction
Barriers to minority participationResearch participation by African Americans (AA) and other minority groups is critical and necessary in order for research to offer more specific information on how minorities are affected by pharmacological and non pharmacological treatments and interventions for chronic and other illnesses. According to Research America, a significant percentage (more than 60%) of African Americans polled said participating in clinical research trials is important as compared to 57% of Hispanic and 47% of non-Hispanic White respondents; however, the numbers for minority participation in documented clinical trials continue to be low. 1 Reports have shown that less than 3% of the general population enrolls in cancer clinical trials which indicates an even larger problem with research inclusion for diseases that have less promising treatment options such as Alzheimer’s disease [2-4]. Alzheimer’s is closely linked to diabetes and is only now beginning to be considered a health disparity. As with other health disparities, African Americans are twice as likely to suffer with Alzheimer’s disease as White Americans [5]. In addition, African Americans are 29 percent more likely to die from heart disease and stroke, and are twice as likely to have diabetes as Whites [6,7]. Based on data from the National Health and Nutrition Survey, African Americans and Hispanic Americans suffer from health disparities such as hypertension, cardiovascular disease and diabetes at higher rates than other ethnic groups. These statistics underscore the need for greater inclusion of minority groups in health related research and are in juxtaposition with the low representation of minorities in clinical research studies. Minority participation in research studies is relevant to understanding and treatment of health disparities and other chronic conditions that impact underserved communities. For example, anti hypertensive clinical trials have found that African Americans, when trying to control symptoms of hypertension to a manageable level, see more benefit with a combination drug therapy than other ethnic groups [8,9]. In addition, Alzheimer’s researchers recently found a gene segment in African American samples that correlates with clinical Alzheimer’s disease; this gene alteration has not been found in Caucasian samples [10]. The previous results support the idea that not all groups respond the same to medications. These results also highlight the need for greater inclusion of minority groups in research studies and the need to get insight into who actually participates in research and why they participate.
Willingness of minorities to participate
Many studies have emphasized the barriers to research participation faced by minority groups. Several studies have described these barriers as both individual and community barriers and emphasized the need to recognize, understand and overcome these barriers in order to address recruitment and retention of African Americans in genetic research studies. Individual barriers include time, money, work, as well as existing medical problems [11-14]. Community barriers include the lack of knowledge about research participation as well as the fear of research and associated establishments and its exploitation of vulnerable populations. Trust has been shown to be a greater barrier for African American males than females; however, even with knowledge of the Public Health Study in Tuskegee, and other self-described barriers, both groups participated in research and stated that they would likely participate again. In addition to the legacy of historical atrocities, several studies have identified issues that serve as solutions to the obstacles in AA participation, such as relationship building, diversity of the recruitment team and funding and education [15,16]. Other studies have suggested that a “lack of information and understanding” of the actual study or lack of understanding of the informed consent document that accompanies most studies leads to low participation among minority groups and suggest that including more flexible methods of gaining consent should be a part of the recruitment process. These methods may include reading the consent document and recording a verbal consent, family vs. individual consent and use of a DVD to enhance the consent process [17,18].
In our previous paper, we reported that while younger African Americans (less than 40 years of age) say that they are willing to participate, African Americans 40 years and older have actually participated in more health related research studies [14]. We want to expand on this study to describe those individuals that have actually participated in health related research studies and outline their experiences and motivations for participation. The objective of the current paper is to describe motivations, profiles and experiences of a distinct cohort of minority participants, in a non-clinical setting, and give a snapshot of who actually participates in health related research studies and why they participate. The overarching goal was to determine the main motivator(s) for participation. In addition, our aims were to 1. Identify the socio-demographic profiles of the participants; 2. Analyze motivation for participation of study subjects; 3. Determine the types of studies that this cohort participated in and are willing to participate in; and 4. Understand participants’ experiences as research study subjects in this process. This current study is one of the largest cross-sectional survey studies conducted in a non-clinical setting, to assess the perceptions of African Americans (AA) and outline the demographics of AA individuals that have experience participating in health related research studies. Participants in this study were part of a cluster sampling of individuals that expressed interest in sharing information about their research experiences. The data discussed in this paper are from individuals that have direct experience in health related research study participation. This paper offers more information about the demographics of participants and addresses certain perceived and real barriers of participation and provides information needed to improve minority participation. In general, this can be useful to inform both the research and medical communities on methods for improving minority access to clinical trials and other health related research studies.
Methods
Survey developmentThe methods used in conducting this study have been published [14]. Briefly, a survey instrument was developed to perceptions of African Americans and their experiences with research participation. The survey consisted of 20 common questions for research study participants (RSP) and non-research study participants (NRSP), with an additional 15 questions only for those who had participated in a clinical or health related research study (HRRS). The focus on this paper will be on those individuals with previous research experience (RSP). Questions were designed with multiple choice answers and written fill in the blank responses. The questions were designed on a middle school reading level and pilot tested on a particularly small group of North Carolina Agricultural &Technical State University students and faculty for readability and content in order to improve the validity of the instrument.
Study population and procedures
We ascertained an intergenerational sample of African American adults that spanned all socioeconomic groups in the Triad region of North Carolina. To reach the demographic of interest in a nonclinical setting, those AA adults in hospitals and health clinics were excluded from this study. Cluster sampling was used to define groups representing different demographic clusters in order to reach a wider range of the AA community. Clusters included: Academic: faculty, staff at historically black colleges or universities (HBCUs), African American sororities and fraternities; Community: congregations from random samples of primarily AA churches; beauty parlors and barber shops with AA clienteles, community centers with AA participants at health fairs, civic organizations’ meetings and other community events attended predominantly by AA adults. Surveys were administered by an interdisciplinary team of trained public health specialists that were community stakeholders with experience in facilitating educational outreach activities in these communities. Participants completed the survey forms independently; however, administrators were available to answer any questions regarding the survey instrument or study. The survey allowed for multiple selections in the questions addressing study type, motivation for participation and sample given. The survey was constructed to include “other” options to allow participants to include items not written into the survey for the answer. Study participants were not given incentives or reimbursements for completing the survey. This study was approved by the North Carolina A & T State University’s Institutional Review Board (IRB).
Statistical analysis
Data were collected from 2009 to 2010 in a de-identified state for all subjects surveyed. Demographic data collected included age, gender, level of education and place of residence. Both descriptive and inferential statistical analyses were included in the analysis. Data were analyzed using multivariate statistical methods since the goal of this study was to understand the role, if any, of multiple variables (including demographic and others) on participation of African Americans in health related research studies. For those who reported previous research participation (RSP), questions assessed the following: (1) knowledge, if any, of well known health studies (such as the Tuskegee Syphilis Study (TSS), Framingham Heart Study (FHS), Women’s Health Initiative (WHI), etc.); (2) willingness to participate again in the future; (3) type of study in which they had participated; (4) disease associated with the study; (5) participation experience; and (6) motivation for participation. Our earlier paper, focused on individuals who reported having no previous research participation experience (NRSP; Lang et al. 2013).
Results
The following results are focused on the sample of participants (n=119) that have health related research study experience. Table 1 contain demographic information of the study participants and focuses on participants that answered yes to the question “Have you ever participated in a health related research study?” Of those 119, 105 (88%) responded yes. Of those that answered yes, 38% were male and 47% were in the age range of 40 to 59 years of age; more than 20% were younger than 40 years of age , and 18% were age 60 and above. All had at least a high school diploma or college degree. Sixty-four percent had participated in 1, 18% in 2, 15% in 3, and approximately 2% had participated in more than 3 research studies. The diseases or disorders that were studied included the following: Diabetes, Blood Pressure, Cancer, Alzheimer’s disease, kidney disease, lupus, organ donation, obesity, seizures, weight loss/management, and national studies such as the Twins Study and the Framingham Heart Study.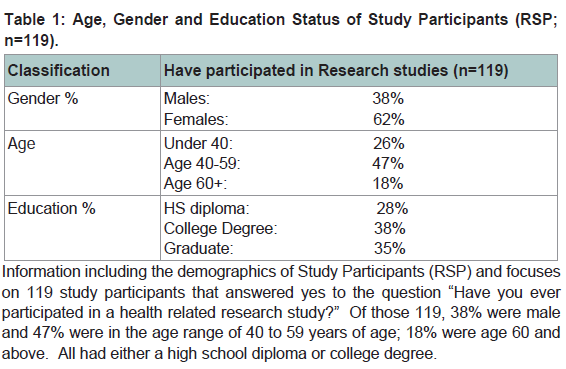
Table 1: Age, Gender and Education Status of Study Participants (RSP;n=119).Information including the demographics of Study Participants (RSP) and focuses on 119 study participants that answered yes to the question “Have you ever participated in a health related research study?” Of those 119, 38% were male and 47% were in the age range of 40 to 59 years of age; 18% were age 60 and above. All had either a high school diploma or college degree.
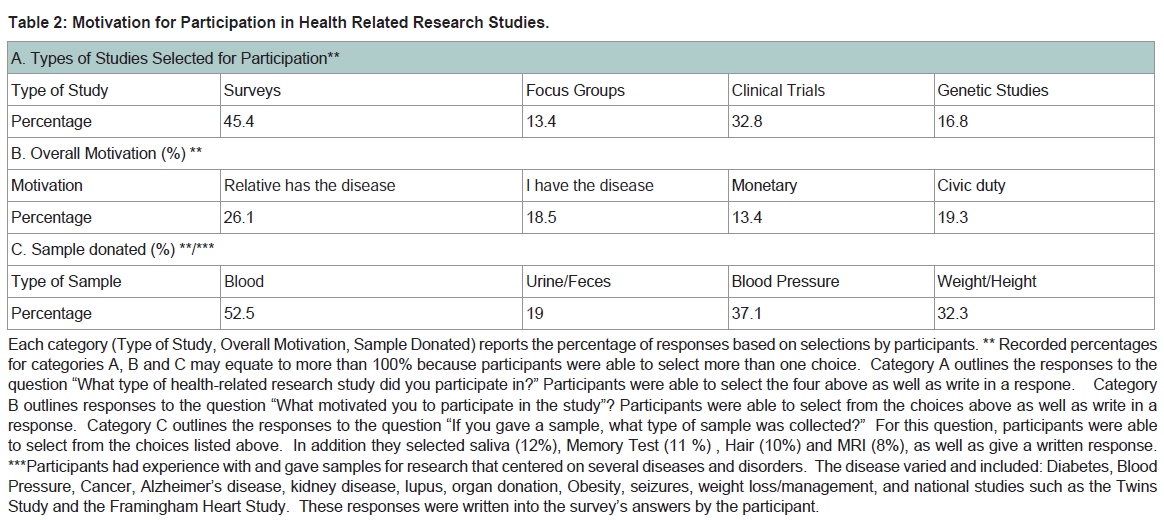
Table 2: Motivation for Participation in Health Related Research Studies.Each category (Type of Study, Overall Motivation, Sample Donated) reports the percentage of responses based on selections by participants. ** Recorded percentages for categories A, B and C may equate to more than 100% because participants were able to select more than one choice. Category A outlines the responses to the question “What type of health-related research study did you participate in?” Participants were able to select the four above as well as write in a respone. Category B outlines responses to the question “What motivated you to participate in the study”? Participants were able to select from the choices above as well as write in a response. Category C outlines the responses to the question “If you gave a sample, what type of sample was collected?” For this question, participants were able to select from the choices listed above. In addition they selected saliva (12%), Memory Test (11 %) , Hair (10%) and MRI (8%), as well as give a written response.***Participants had experience with and gave samples for research that centered on several diseases and disorders. The disease varied and included: Diabetes, Blood Pressure, Cancer, Alzheimer’s disease, kidney disease, lupus, organ donation, Obesity, seizures, weight loss/management, and national studies such as the Twins Study and the Framingham Heart Study. These responses were written into the survey’s answers by the participant.
Discussion
The current study describes a population of older African Americans that have participated in health-related research studies and were willing to participate in future health related research studies. A wide range in age and education was captured by this cohort. This cohort consented to participate in different types of procedures from less invasive (weight/height measurement) to more invasive (blood, memory assessments), and had a very good understanding of the informed consent process and information. More importantly, having a family member with the disease or performing their civic duty were the main motivators for this group. In this cohort, more than 65% of the participants had knowledge of the National Public Health Study on Untreated Syphilis. Knowledge of past research atrocities, involvement with invasive procedures and the need to give different types of specimens all failed to deter this group from wanting to participate in health related research studies [18,19]. These results encourage us to look at other factors or barriers to research participation in a willing group of individuals with no previous research participation experience. It is necessary to highlight that African American communities are heterogeneous, and there are few studies to describe those that do participate in research studies and also make suggestions for effective recruitment models of heterogeneous minority populations. Moreover, African Americans may take into account benefits of participation as well as family, ethical and legal issues when considering research participation [20-22]. Incorporating a model that allows for community involvement and constant communication with research participants is important for establishing trust and relationship building between researchers and communities. However, addressing barriers to research access by minority groups remains vitally important in health related research studies. Determining measures that address specific vulnerabilities within the minority population may be a way to address access and to fully understand barriers to research participation. It is necessary to identify the sources of vulnerability and to use these issues to improve recruitment of minorities for clinical research [23-25].A limitation of this study was the inclusion of all age groups. It would be interesting to see, within a larger cohort of African American elders, if the motivation for participation would remain the same. It would also be necessary to expand the choices for motivation and to assess what other issues may support research participation within different sub populations. This study could have emphasized motivations in an older or elder population and assessed differences for motivation for different age groups. Another limitation is that participants were not surveyed in the midst of their research experience. We asked for information after participation was complete which, in some cases, may have been months or years later. In the future we plan to pursue more detailed questions regarding research experiences from individuals that are zero to 3 months from their research experience which may provide very unique information about the experience, their motivation and how the experience may be improved to have the greatest impact. The results presented in this study are not intended to offer a uniform view of African Americans perspectives in clinical research participation; however, they do offer a glimpse at who is likely to participate and substantiates what we already know which is that African Americans are willing and do actually participate in research.
Conclusions
In order to reach minorities across the life span, activities should be implemented such as providing transportation, appropriate compensation, education and awareness about the disease which empowers individuals to make informed decisions about their health and health care, and may lower barriers to research participation. This study recognizes that considering the cultural or community relevance of the research study as well as engaging the community and its stakeholders may lower barriers to research participation.Acknowledgements
Funding for this article was made possible (in part) by P20MD000546 from the National Center on Minority Health and Health Disparities. The views expressed in written conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention by trade name, commercial practices, or organizations imply endorsement by the U.S. Government.References
- (2013) Research America.
- Vicini F, Nancarrow-Tull J, Shah C, Chmielewski G, Fakhouri M, et al. (2011) Increasing accrual in cancer clinical trials with a focus on minority enrollment: The William Beaumont Hospital Community Clinical Oncology Program Experience. Cancer 117: 4764-4771.
- Wendler D, Kington R, Madans J, Van Wye G, Christ-Schmidt H, et al. (2006) Are racial and ethnic minorities less willing to participate in health research? PLoS Med e19.
- Tejeda HA, Green SB, Trimble EL, Ford L, High JL, et al. (1996) Representation of African-Americans, Hispanics, and whites in National Cancer Institute cancer treatment trials. J Natl Cancer Inst 88: 812–816.
- (2013) The Office of Minority Health.
- Schiller JS, Lucas JW, Ward BW, Peregoy JA (2012) Summary health statistics for U.S. adults: National Health Interview Survey, 2010. Vital Health Stat 10: 252.
- (2013) The Center for Information and Study on Clinical Research Participation.
- Flack JM, Nasser SA, Levy PD (2011) Therapy of hypertension in African Americans. Am J Cardiovasc Drugs 11: 83-92.
- Ferdinand KC, Armani AM (2007) The management of hypertension in African Americans. Crit Pathw Cardiol 6: 67-71.
- Reitz C, Jun G, Naj A, Rajbhandary R, Vardarajan BN, et al. (2013) Variants in the ATP-binding cassette transporter (ABCA7), apolipoprotein E ϵ4,and the risk of late-onset Alzheimer disease in African Americans. JAMA 309: 1483-1492.
- Ngozi Ejiogu, Norbeck HH, Mason MA, Comwell BC, Zonderman AB, et al. (2011) Recruitment and retention strategies for minority or poor clinical research participants: lessons from the healthy aging in neighborhoods of diversity across the life span study. Gerontologist 51: S33-S45.
- Christopher S, Watts V, McCormick AK, Young S (2008) Building and maintaining trust in a community-based participatory research partnership. Am J Public Health 98: 1398-1406.
- Corbie-Smith G, Thomas SB, Williams MV, Moody Ayers S (1999) Attitudes and beliefs of African Americans toward participation in medical research. J Gen Intern Med 14: 537-546.
- Lang R, Kelkar VA, Byrd JR, Edwards CL, Pericak Vance M, et al. (2013) African American participation in health-related research studies: indicators for effective recruitment. J Public Health Manag Pract 19: 110-118.
- Byrd GS, Edwards CL, Kelkar VA, Phillips RG, Byrd JR, et al. (2011) Recruiting intergenerational African American males for biomedical research Studies: a major research challenge. J Natl Med Assoc 103: 480-487.
- Corbie-Smith G, Williams IC, Blumenthal C, Dorrancem J, Estroff SE, et al. (2007) Relationships and communication in minority participation in research: multidimensional and multidirectional. J Natl Med Assoc 99: 499-498.
- Dunlop AL, Leroy ZC, Logue KM, Glanz K, Dunlop BW (2011) Preconsent Education and Consent Processes improved African Americans' willingness. J Clin Epidemiol 64: 872-877.
- Quinn SC1, Garza MA, Butler J, Fryer CS, Casper ET, et al. (2012) Improving Informed Consent with Minority Participants: Results from Researcher and Community Surveys. J Empir Hum Res Ethics 7: 44-55.
- Joseph M (2012) Unger Practice Management. Unger JM.
- McDonald JA, Barg FK, Weathers B, Guerra CE, Troxel AB, et al. (2012) Understanding participation by African Americans in cancer genetics research. J Natl Med Assoc 104: 324-330.
- Kennedy BR, Mathis CC, Wood AK (2007) African Americans and their distrust of the health care system: healthcare for diverse populations. J Cult Divers 14: 56-60.
- Gross CP, Filardo G, Mayne ST, Krumholz HM (2005) The impact of socioeconomic status and race on trial participation for older women with breast cancer. Cancer 103: 483-491.
- Williams MM, Meisel MM, Williams J, Morris J (2010) An Interdisciplinary Outreach Model of African American Recruitment for Alzheimer’s Disease Research. Gerontologist 51: 134-141.
- Spruill I (2010) Enhancing recruitment of African-American families into genetic research: lessons learned from Project SuGar. J Comm Genet 1: 125-132.
- Diaz VA, Mainous AG, McCall AA, Geesey ME (2008) Factors affecting research participation in African American college students. Fam Med 40: 46-51.