
International Journal of Otorhinolaryngology
Download PDF
Case Report
*Address for Correspondence: Dr. Mohamad A Bitar, MD, FACS, FAAP, Department of ENT Surgery, The Children’s Hospital at Westmead, Locked Bag 4001, Westmead NSW 2560, Australia, Fax: +61298452078 ; E-mail: mbitar-md@hotmail.com
Citation: Bitar MA, Kamal M, Rameh C. A Vallecular Thyroglossal Duct Cyst Presenting with Persistent Unexplained Cough in a Toddler. Inter J Otorhinolaryngology. 2014;1(1): 3.
Copyright © 2014 Bitar et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolaryngology | ISSN: 2380-0569 | Volume: 1, Issue: 1
Submission: 01 October 2014 | Accepted: 15 November 2014 | Published: 17 November 2014
 Examination under anesthesia
Examination under anesthesia
 Though the plan was to marsupialize the cyst, the wall was found to be thicker than a usual VC, so decision was made to excise the mass. Excision was carried out with good hemostasis and with minimal cauterization to avoid postoperative edema. The specimen was removed in one piece (Figure 3).
Though the plan was to marsupialize the cyst, the wall was found to be thicker than a usual VC, so decision was made to excise the mass. Excision was carried out with good hemostasis and with minimal cauterization to avoid postoperative edema. The specimen was removed in one piece (Figure 3).
 Postoperative course & follow-up: The patient tolerated the procedure well and the postoperative period was uneventful with no airway compromise, with good tolerance of oral food intake. Interestingly, the cough subsided immediately postoperatively. The patient has been followed up for 8 years with no recurrence.
Postoperative course & follow-up: The patient tolerated the procedure well and the postoperative period was uneventful with no airway compromise, with good tolerance of oral food intake. Interestingly, the cough subsided immediately postoperatively. The patient has been followed up for 8 years with no recurrence.

A Vallecular Thyroglossal Duct Cyst Presenting with Persistent Unexplained Cough in a Toddler
Mohamad A. Bitar123*, Mohammad Kamal4 and Charbel Rameh1,5
- 1Department of Otolaryngology-Head & Neck Surgery, American University of Beirut, Lebanon
2Department of Pediatrics and Adolescent Medicine, American University of Beirut Faculty of Medicine & Medical Center, Beirut, Lebanon
3The Children’s Hospital at Westmead, Sydney Medical School, University of Sydney, Australia
4American University of Beirut School of Medicine & Medical Center, Lebanon
5Currently in Private Practice, Beirut, Lebanon
*Address for Correspondence: Dr. Mohamad A Bitar, MD, FACS, FAAP, Department of ENT Surgery, The Children’s Hospital at Westmead, Locked Bag 4001, Westmead NSW 2560, Australia, Fax: +61298452078 ; E-mail: mbitar-md@hotmail.com
Citation: Bitar MA, Kamal M, Rameh C. A Vallecular Thyroglossal Duct Cyst Presenting with Persistent Unexplained Cough in a Toddler. Inter J Otorhinolaryngology. 2014;1(1): 3.
Copyright © 2014 Bitar et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolaryngology | ISSN: 2380-0569 | Volume: 1, Issue: 1
Submission: 01 October 2014 | Accepted: 15 November 2014 | Published: 17 November 2014
Abstract
Laryngeal cysts involving the valleculae are rare but well known cause of upper respiratory obstruction. Vallecular cysts are uncommon lesions seen in the pediatric population and mostly present within the first few weeks of life. They may present with diversity of clinical signs and symptoms including failure to thrive, stridor and respiratory distress. Thyroglossal duct cyst, on the other hand, is the most common pediatric congenital anomaly that usually presents as a midline anterior neck mass but may occur anywhere from the foramen cecum to the suprasternal region. We hereby report a case of thyroglossal duct cyst occurring in the vallecular region mimicking a vallecular cyst in a pediatric patient with unexplained cough.Introduction
Cysts involving the vallecular regions are uncommon lesions and represent 10.5% to 20.1% of all laryngeal cysts [1]. Vallecular cysts (VC) are rare lesions mostly encountered in the pediatric age group and usually present within the first few weeks of life [2,3]. Clinical presentation is variable and they may be asymptomatic mass, or may present with inspiratory stridor, failure to thrive, poor feeding, cyanotic spells, recurrent cough, abnormal hoarse cry, regurgitation of feeds, dyspnea, supralaryngeal obstruction and sudden infant death [2,3]. The mechanical effect on breathing of an infant can be explained by the inferior-posterior displacement of the epiglottis caused by the enlarging mass, or by mass effect on the hypopharynx [4]. This effect is more profound in the neonates who have a relatively smaller airway volume that makes it more prone to collapse [5], resulting in stridor [6,7] or apnea [5].We hereby present a 4-year-old girl who presented with chronic cough refractory to medical treatment and was found to have a VC that, on final pathology turned out to be a thyroglossal duct cyst (TGDC) occupying the valleculae.
Case Presentation
Clinical signs and symptomsA 4-year-old girl presented with a history of persistent unexplained cough refractory to conventional medical therapies. No other symptoms were reported. On physical examination, the oral cavity was intact with no observed abnormalities. Neck exam revealed no masses. Flexible fiberoptic laryngoscopy: a 1x1 cm mass was visualized occupying the vallecular region. The mass appeared smooth with normal-colored overlying mucosa and notable displacement of the epiglottis posteriorly.
Imaging & laboratory tests
Computed tomography scan revealed a cystic lesion filling the valleculae and displacing the epiglottis posteriorly with protrusion into the airway and minimal extension into base of tongue (Figure 1). Thyroid function tests were normal, and ultrasound of the neck showed normal size and position of the thyroid gland.
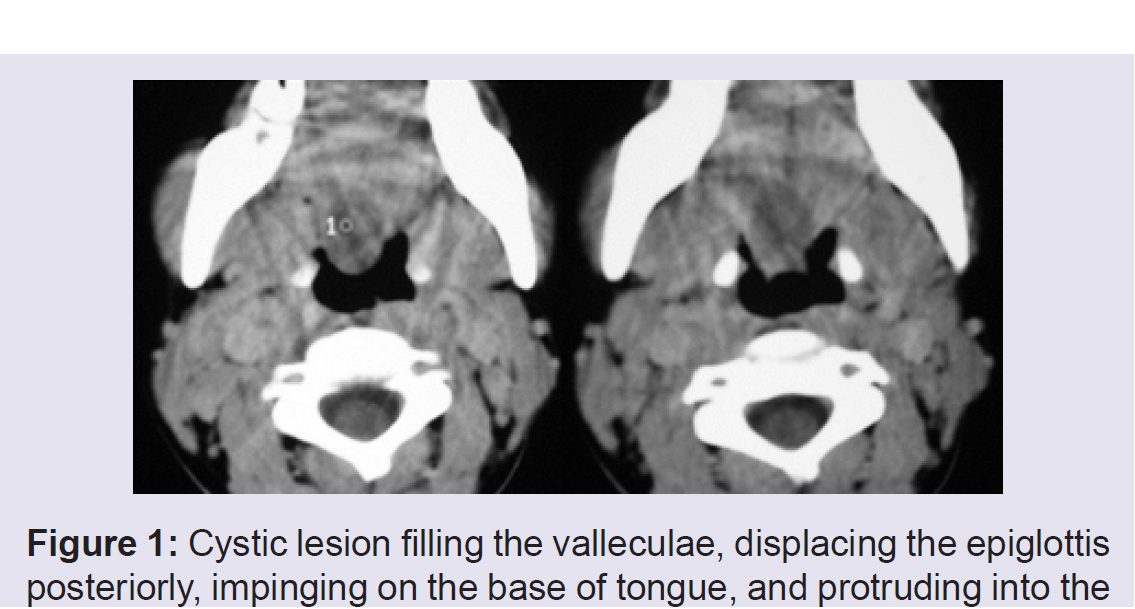
Figure 1: Cystic lesion filling the valleculae, displacing the epiglottis posteriorly, impinging on the base of tongue, and protruding into the airway lumen.
Direct laryngoscopy and bronchoscopy were performed revealing normal airway apart from the vallecular cyst.
Procedure & operative findings
The patient underwent excision of the cyst through suspension microlaryngoscopy, using a long micro-needle cautery (Figure 2).

Figure 2: Excision of the cyst through suspension microlaryngoscopy, using a long micro-needle cautery.
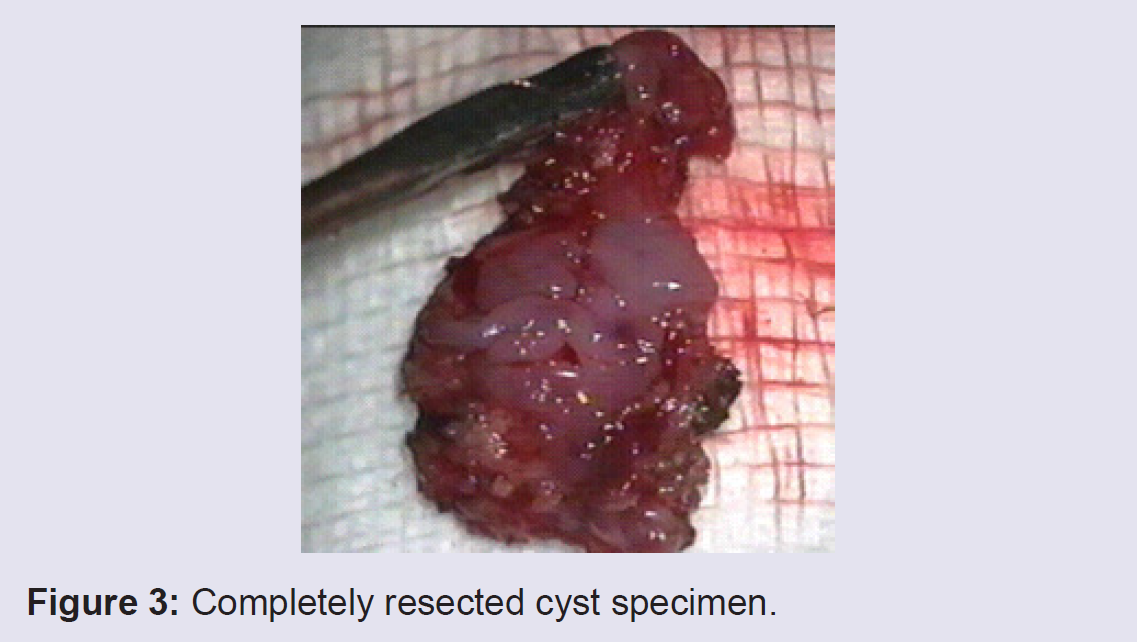
Figure 3: Completely resected cyst specimen.
Histopathology
Histological evaluation of the specimen revealed squamous epithelium lined cyst with thyroid tissue, which is consistent with TGDC (Figure 4).
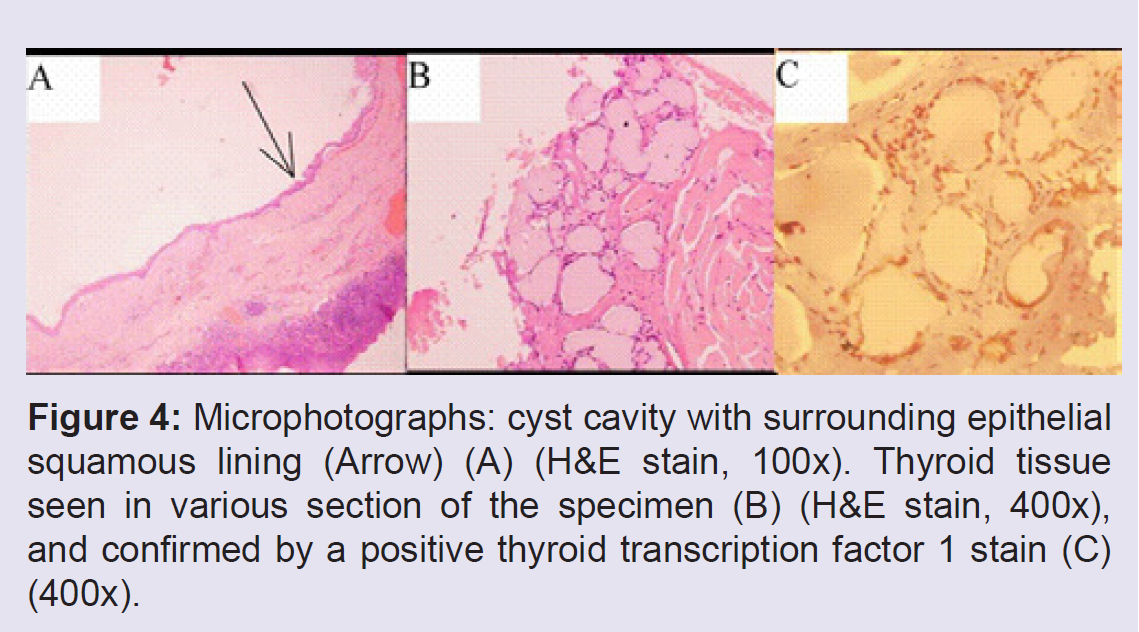
Figure 4: Microphotographs: cyst cavity with surrounding epithelial squamous lining (Arrow) (A) (H&E stain, 100x). Thyroid tissue seen in various section of the specimen (B) (H&E stain, 400x), and confirmed by a positive thyroid transcription factor 1 stain (C) (400x).
Discussion
The most commonly encountered lesion in the vallecular region is a VC. Differential diagnosis of vallecular mass includes lingual tonsils, lymphoma, lingual thyroid, lingual (TGDC), hemangioma, lymphangioma, teratoma, and dermoid cyst [2,3,5,6,8], with VC being the most common. The pathogenesis of VC involves the obstruction of a submucousal gland in the valleculae leading to a mucus retention cyst [3]. A definitive diagnosis is made endoscopically and confirmed by pathology. Work up may include computed tomography scan, magnetic resonance imaging, lateral neck x-ray, and barium esaphogram. Thyroid nuclear imaging and thyroid function test can help rule out ectopic thyroid tissue [2,3,9].The TGDC, on the other hand, is a common cause of a congenital neck mass in the pediatric age group [9]. Thyroglossal duct cysts can arise anywhere from foramen cecum in the tongue to the suprasternal region [10,11]. Embryologically, the thyroid gland develops as an epithelial proliferation on the midline at the anterior floor of pharynx and then migrates from the foramen cecum inferiorly to its final position anterior to the upper portion of the trachea in the 7th week of gestation. The duct eventually involutes, but the epithelial remnants could be left behind anywhere along the migratory pathway and aberrant pathway may result in a TGDC being developed at unusual sites [9-11]. It is primarily managed by surgical excision [9,10].
Vallecular cysts are usually found in the vallecular area or attached to the epiglottis. They have also been called epiglottic cyst, base-of the- tongue cyst, and congenital cyst [2]. The location of the cyst we encountered and the appearance on the computed tomography scan was highly suggestive of a VC. During the surgery, we found that the bulk of the lesion was based in the valleculae with impingement on the base of the tongue without apparent extension into the lingual tissue. The pathology result was unexpected given that the mass was distant from the foramen cecum and there was no apparent tract connecting the lesion to the cyst.
Suh et al. differentiated between a vallecular cyst and what they called an “internal TGDC” in that location by relying on the position of the lesion with respect to the foramen cecum [12]. A cyst buried in the tongue base and close to the hyoid bone or the foramen cecum was classified as “internal” TGDC. Otherwise, it was considered a VC, being the most common cyst in the valleculae. Pathologically, both lesions are lined by a similar epithelium, and thus, relying on the presence of thyroid tissue is important to differentiate between them as this is present in 46% of the TGDCs [13].
Allard et al. reported in a meta-analysis that 2.1% of TGDC were lingual, 24.1% suprahyoid, 60.9% between hyoid and thyroid cartilage, and 12.9% suprasternal [11,14]. Similar distribution was reported by Brousseau et al., Ren et al. and Ahuja et al. reported 47.8% infrahyoid TGDC in pediatrics [11,15,16]. Although approximately 50% of TGDCs are located close or just inferior to the body of the hyoid bone, they may also be found at the base of tongue or close to the thyroid cartilage [17]. Cases of TGDCs were also reported in the floor of the mouth and larynx [8], It is unknown what exactly triggers the epithelial remnant to proliferate into a cyst, but inflammation, infection and mucous retention are likely to cause the mass to get bigger [8,11].
Based on location alone, our lesion would be classified as a VC; however, the presence of thyroid tissue qualifies it as a TGDC. To the best of our knowledge, this is the first reported vallecular TGDC. Nonetheless, it is possible that such lesions may have been previously reported as VC because of the absence of thyroid tissue; others may have been reported as lingual TGDCs because of extension into the base of tongue.
The importance of differentiating between a VC and TGDC lies in the fact that both lesions are managed differently. Vallecular cysts are mostly managed by de-roofing and marsupialization [5,18] using cold knife, cup forceps, or CO2 laser. Recurrence of VC is rare if marsupialization is done properly. However, TGDCs are associated with risk of recurrence of about 5-15% [9]. Thus, TGDCs require complete surgical excision and sometimes necessitate a combined intraoral and extraoral approach [19]. In our case, the lesion was managed conservatively, as the cyst was shelling out with ease, along with the high preoperative and intraoperative suspicion of a VC and not TGDC, given its location.
Vallecular masses, in general, have been associated with laryngomalacia [4,7] but that was not encountered in our case. When large enough, they can also displace the epiglottis and obscure the airway [4], and thus require extra care during intubation. Possible intraoperative complications include cyst rupture and possible aspiration pneumonia, edema, and bleeding [4]. Although our cyst leaked during excision, this did not compromise the dissection nor resulted in aspiration. In contrast, cyst’s rupture somewhat facilitated exposure as it was obstructing the surgical view through the laryngoscope and making the dissection more difficult.
Conclusion
We reported a child with an unusual presentation of a vallecular lesion that turned out to be a TGDC presenting in an unusual location. Although these cysts are rare, the surgeon must be aware of their presence and may consider excision of the cyst rather than marsupializing it if its wall is thicker than a usual VC or it has a significant extension into the base of tongue. Definitive diagnosis is made by histological examination. Recurrences of VC may be due to the fact that they were in reality TGDCs.References
- Romak JJ, Olsen SM, Koch CA, Ekbom DC (2010) Bilateral vallecular cysts as a cause of Dysphagia: case report and literature review. Int J Otolaryngol 2010: 697583.
- Gutiérrez JP, Berkowitz RG, Robertson CF (1999) Vallecular Cysts in Newborns and Young Infants. Pediatr Pulmonol 27: 282-285.
- Mahajan V, Mathew JL, Singh M, Gupta R, Das A (2008) Vallecular cyst-revisited. Indian J Pediatr 75: 1081-1082.
- Cheng KS, Ng JM, Li HY, Hartigan PM (2002) Vallecular cyst and laryngomalacia in infants: report of six cases and airway management. Anesth Analg 95: 1248-1250.
- Hsieh WS, Yang PH, Wong KS, Li HY, Wang EC, et al. (2000) Vallecular cyst: an uncommon cause of stridor in newborn infants. Eur J Pediatr 159: 79-81.
- Yao TC, Chiu CY, Wu KC, Wu LJ, Huang JL (2004) Failure to thrive caused by the coexistence of vallecular cyst, laryngomalacia and gastroesophageal reflux in an infant. Int J Pediatr Otorhinolaryngol 68:1459-1464.
- Shah M, Mehta A (2006) Neonatal vallecular cyst. Indian Pediatr 43: 652.
- Nakayama S, Kimachi K, Nakayama K, Ikebe T, Ozeki S (2009) Thyroglossal Duct Cyst Occurring in the Floor of the Mouth: report of 2 cases. J Oral Maxillofac Surg 67: 2690-2693.
- Burkart CM, Richter GT, Rutter MJ, Myer CM 3rd (2009) Update on the Endoscopic Management of Lingual Thyroglossal Ducts Cysts. Laryngoscope 119: 2055-2060.
- Sathish C, Nyamannawar BM, Mohanty S, Correa MM, Das K (2008) Atypical thyroglossal duct anomalies. Int J Pediatr Otorhinolaryngol 72: 1353-1357.
- Ren W, Zhi K, Zhao L, Gao L (2011) Presentations and management of thyroglossal duct cyst in children versus adults: a review of 106 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 111: e1-6.
- Suh MW, Sung MW (2004) Apnea spells in an infant with vallecular cyst. Ann Otol Rhinol Laryngol 113: 765.
- Chandra RK, Maddalozzo J, Kovarik P (2001) Histologic characterization of the thyroglossal tract: implications for surgical management. Laryngoscope 111: 1002-1005.
- Allard RH (1982) The thyroglossal cyst. Head Neck Surg 5: 134-146.
- Brousseau VJ, Solares CA, Xu M, Krakovitz P, Koltai PJ (2003) Thyroglossal duct cysts: presentation and management in children versus adults. Int J Pediatr Otorhinolaryngol 67: 1285-1290.
- Ahuja AT, King AD, King W, Metreweli C (1999) Thyroglossal duct cysts: sonographic appearances in adults. AJNR Am J Neuroradiol 20: 579-582.
- Sadler TW (2004) Langman's Medical Embryology. Congenital Abnormalities Embryology (9th ed) Lippincott Williams & Wilkins, Philadelphia, USA.
- Tuncer U, Aydogan LB, Soylu L (2002) Vallecular cyst: a cause of failure to thrive in an infant. Int J Pediatr Otorhinolaryngol 65: 133-135.
- Sattar AK, McRae R, Mangray S, Hansen K, Luks FI (2004) Core excision of the foramen cecum for recurrent thyroglossal duct cyst after Sistrunk operation. J Pediatr Surg 39: E3-5.
- Tibesar RJ, Thompson DM (2003) Apnea spells in an infant with vallecular cyst. Ann Otol Rhinol Larnygol 112: 821-824.