
Journal of Cancer Sciences
Download PDF
Research Article
*Address for Correspondence: Ginocchi Laura, MD, Division of Medical Oncology, Azienda USL Toscana Nord Ovest, Nuovo Ospedale delle Apuane (NOA), Massa, Italy, Tel: +39-3281990760; E-mail: lauraginocchi@hotmail.it
Citation: Ginocchi L, Valsuani C, Sara L, Ceccherini C, Pedata M, et al. Gemcitabine-Capecitabine Chemotherapy Plus Intra-Arterial Epirubicin-Cisplatin in Pancreatic Cancer Patients after FOLFIRINOX First Line Chemotherapy: A Retrospective Analysis. J Cancer Sci. 2016;3(2): 5.
Copyright © 2016 Ginocchi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cancer Sciences | ISSN: 2377-9292 | Volume: 3, Issue: 1
Submission: 11 August, 2016 | Accepted: 03 September, 2016 | Published: 09 September, 2016
Materials (patients) and methods: We retrospectively collected data of 41 locally advanced/metastatic pancreatic cancer patients underwent to FOLFIRINOX first line chemotherapy and subsequently treated with Gemcitabine-Capecitabine chemotherapy plus Intraarterial Epirubicin-Cispatin (EC-GEMCAP).
Results: Treatment was well tolerated, without dose reductions or delays. Hematologic and no hematologic grade 3-4 toxicities were 39% and 12.2%. Twenty, 2 and 12 patients obtained a stability/partial response/progression disease respectively, with a disease control rate in 22 patients. One patient with locally advanced disease underwent to radically surgery after 6 cycles of EC-GEMCAP. Median OS was 16.9 months (95% CI: 14.7-19.0) with OS rates at 6, 12 and 24 months of 95.1%, 80.5% and 31.7%. As regards second-line therapy, median OS was 8.9 months (95% CI: 6.9-10.9). OS rates at 6, 12 and 24 months were 61%, 80.5% and 31.7%. EC-GEMCAP median PFS was 4.1 months (95% CI: 3.1-5.1).PFS rates at 6 and 12 months were 41.5% and 19.5%.
Conclusions: EC-GEMCAP proved to be a viable treatment in terms of toxicity and activity and it could be considered a therapeutic option also in poor performance status patients.

We administered a total of 181 cycles of EC-GEMCAP therapy, median per patients: 3 cycles (range 1-15). Globally, treatment was well tolerated, without dose reductions or delays. All grade hematologic and no-hematologic toxicities were 65.8% and 34.1%, grade 3-4 were 39% (leucocytopenia 24.4%, thrombocytopenia 14.6%) and 12.2% (fatigue 2.4%, vomiting 7.3%, diarrhoea 2.4%), respectively (Table 2).
RECIST assessment was possible in 35 of 41 patients (6 patients progressed during the first 2 cycles): 20 patients (57.1%) obtained disease stability and 2 patients (5.7%) a partial response, with a disease control rate in 22 patients (62.3%). Twelve patients (37.1%) had a progression disease (Table 3).
One patient with locally advanced disease underwent to radically surgery after 6 cycles of ECGEMCAP therapy.CA 19.9 response was evaluable for 33 patients: it was reduced in 11 (33.3%) patients (of these, normalized in 1 (3%)), stable in 9 patients (27.3%) and increased in 13 (39.4%).After a median follow-up of 16.9 months (range 4.2-56.9 months) since diagnosis, median OS was 16.9 months (95% CI: 14.7-19.0) with a OS rates at 6, 12 and 24 months of 95.1%, 80.5% and 31.7%, respectively (Figure 1).

As regards second line therapy, after median follow-up of 8.9 months (range 0.6-48.5 months) median OS was 8.9 months (95% CI: 6.9-10.9) (Figure 2). The OS rates at 6, 12 and 24 months were 61%, 80.5% and 31.7%, respectively. EC-GEMCAP median PFS was 4.1 months (95% CI: 3.1-5.1) (Figure 2). The PFS rates at 6 and 12 months were, respectively, 41.5% and 19.5%.

Gemcitabine-Capecitabine Chemotherapy Plus Intra- Arterial Epirubicin-Cisplatin in Pancreatic Cancer Patients after FOLFIRINOX First Line Chemotherapy: A Retrospective Analysis
Ginocchi Laura1*, Valsuani Chiara1, Sara Lucchesi2, Ceccherini Claudio3, Pedata Mariangela1, Della Seta Roberta1, Federici Francesca1, Orlandi Massimo1, Venturini Savigliana1, Fiorentini Giammaria4, Cantore Maurizio5 and Mambrini Andrea1
- 1Division of Medical Oncology, Azienda USL Toscana Nord Ovest, Nuovo Ospedale delle Apuane (NOA), Massa (MS), Italy
- 2UOC Oncologia Medica, Azienda USL Toscana Nord Ovest, P.O. F. Lotti, Pontedera (PI)
- 3UO Radiologia Interventistica, Azienda USL Toscana Nord Ovest, Nuovo Ospedale delle Apuane (NOA), Massa (MS)
- 4UO Oncologia Medica, Azienda Ospedaliera Ospedali Riuniti Marche Nord, Ospedale San salvatore, Muraglia, Pesaro (PU)
- 5UO Oncologia Medica, Azienda Ospedaliera Poma, P.O. di Mantova (MN)
*Address for Correspondence: Ginocchi Laura, MD, Division of Medical Oncology, Azienda USL Toscana Nord Ovest, Nuovo Ospedale delle Apuane (NOA), Massa, Italy, Tel: +39-3281990760; E-mail: lauraginocchi@hotmail.it
Citation: Ginocchi L, Valsuani C, Sara L, Ceccherini C, Pedata M, et al. Gemcitabine-Capecitabine Chemotherapy Plus Intra-Arterial Epirubicin-Cisplatin in Pancreatic Cancer Patients after FOLFIRINOX First Line Chemotherapy: A Retrospective Analysis. J Cancer Sci. 2016;3(2): 5.
Copyright © 2016 Ginocchi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cancer Sciences | ISSN: 2377-9292 | Volume: 3, Issue: 1
Submission: 11 August, 2016 | Accepted: 03 September, 2016 | Published: 09 September, 2016
Abstract
Background: Most pancreatic cancer patients have disease recurrence/progression within 6 months from firstline chemotherapy end. Today, there is no a standard of care of second-line therapy.Materials (patients) and methods: We retrospectively collected data of 41 locally advanced/metastatic pancreatic cancer patients underwent to FOLFIRINOX first line chemotherapy and subsequently treated with Gemcitabine-Capecitabine chemotherapy plus Intraarterial Epirubicin-Cispatin (EC-GEMCAP).
Results: Treatment was well tolerated, without dose reductions or delays. Hematologic and no hematologic grade 3-4 toxicities were 39% and 12.2%. Twenty, 2 and 12 patients obtained a stability/partial response/progression disease respectively, with a disease control rate in 22 patients. One patient with locally advanced disease underwent to radically surgery after 6 cycles of EC-GEMCAP. Median OS was 16.9 months (95% CI: 14.7-19.0) with OS rates at 6, 12 and 24 months of 95.1%, 80.5% and 31.7%. As regards second-line therapy, median OS was 8.9 months (95% CI: 6.9-10.9). OS rates at 6, 12 and 24 months were 61%, 80.5% and 31.7%. EC-GEMCAP median PFS was 4.1 months (95% CI: 3.1-5.1).PFS rates at 6 and 12 months were 41.5% and 19.5%.
Conclusions: EC-GEMCAP proved to be a viable treatment in terms of toxicity and activity and it could be considered a therapeutic option also in poor performance status patients.
Introduction
Pancreatic cancer is the fourth leading cause of cancer death in men and women [1], the fifth in Europe [2]. Surgery is the only potential curative therapy and radically resection represents an important prognostic factor with an overall survival advantage in negative surgical margins patients. Unfortunately, only 10-20% of cases meeting criteria for localized and resectable disease (stage I or II) following diagnosis, while 30-40% of patients have a locally advanced or borderline resectable disease [3] and are candidates in medical treatment, due to high risks of occult metastasis and positive surgical margin in case of surgery. The 50-60% of pancreatic cancer is already metastatic at diagnosis, thus medical therapy remains the only alternative that can prolong survival, which, however, does not exceed 11 months in the most active regimens (FOLFIRINOX) [4]. Poor prognosis is mainly due to biological cancer aggressiveness and the low sensitivity to medical treatments, as systemic chemotherapy and radiotherapy. Previously studies showed pancreatic cancer sensitive to locoregional chemotherapy, due to increasing drug delivery [5-9] and consequent therapeutic efficacy strengthening in adjuvant and metastatic setting [10-14].Although recent advances have improved outcomes in first line therapy, the vast majority of patients have disease recurrence or progression within 6 months, as concern the most active regimens FOLFIRINOX and nab-paclitaxel gemcitabine association [4,15]. Today, there is no a standard of care in this setting and, unfortunately, treatment options in subsequent lines are limited, partly because patient clinical condition are deteriorated and chemotherapy is often burdened by significant side effects.
Relying on these premises and on the results of previously studies, which demonstrated efficacy and safety of intra-arterial chemotherapy, we retrospectively investigated the role of gemcitabine/capecitabine plus intra-arterial epirubicin-cisplatin (EC-GEMCAP) after FOLFIRINOX first line chemotherapy.
Patients and Methods
Patients diagnosed with histologically or citologically surgical unresectable, locally advanced or metastatic pancreatic adenocarcinoma treated with FOLFIRINOX first line chemotherapy, from January 2011 to May 2014 where eligible for analysis.They had to have age 18 to 75 years, ECOG performance status ≤2 and adequate organ function (leukocyte count >3500/μL, haemoglobin ≥10.0 g/dL, serum creatinine < 1.25 times upper limit of normal (ULN), transaminases and alkaline phosphatase < 2.5 times ULN, bilirubin < 1.5 times ULN).
Staging included abdominal sonography, total abdomen and chest CT scan. Weight, performance status, CA 19-9 levels, and side effects were evaluated at study entry and after each cycle of regional therapy. An abdomen and chest CT scan was repeated every 3 treatment cycles. All patients gave their informed consent according to our institutional guidelines.
Treatment plan
On day 1, epirubicin 35 mg/mq and cisplatin 42 mg/mq were administered into celiac axis by bolus injection through a catether inserted in the femoral artery with the Seldinger method.
Capecitabine was given orally at the fixed dose of 650 mg/mq twice a day, on days 2-15.
Gemcitabine was administered on day 2 of each cycle at a starting dose of 1,000 mg/mq (intravenously, over 30 minutes). Treatment was repeated every 28 days, until evidence of progression disease or in event of unacceptable toxicity, or in case of patient request.
In addition, an antiemetic (granisetron 8 mg) and an H2-receptor antagonist (famotidine 40 mg) were given intravenously.
Adverse events were recorded according to the National Cancer Institute of Canada common toxicity criteria (NCIC-CTC). The epirubicin and/or cisplatin and/or capecitabine dosage was adjusted, delayed or omitted for toxic effects ≥ grade 2, based on protocol guidelines.
The response was evaluated after 3 cycles using abdomen and chest CT scan according to Response Evaluation Criteria in Solid Tumors (RECIST), 1.1 version. In cases of clinical response, independent of CT scan response, further 3 cycles were administered.
Statistics
Demographic and clinical characteristics were retrospectively recorded in database and summarized by medians and frequencies, as appropriate.
The primary end-point was PFS, defined as the time interval between EC-GEMCAP beginning and time of disease progression based on imaging studies or death, whichever occurred first. OS was defined as the time interval between EC-GEMCAP beginning and time of death or last follow-up.
PFS and OS were estimated by Kaplan-Meier method.
A clinical response was defined as an improvement in symptoms present at the beginning of treatment and was based on the investigators’ evaluation. The objective response rate was calculated as the sum of complete and partial responses. The disease control rate was defined as the sum of complete and partial responses and stable disease.
SPSS for Windows version 13 was used for data analysis.
Results
From January 2011 to May 2014, we identified 41 patients with locally advanced or metastatic pancreatic cancer treated with FOLFIRINOX first line chemotherapy. A total of 80 cycles of FOLFIRINOX was administered, a median of 8 cycles for each patient (range 4-14). Ten patients also received loco-regional treatment: surgery, radiotherapy alone, radiotherapy associated to gemcitabine and termablation in 2, 2, 4 and 2 patients, respectively. Twenty seven patients (65.9%) progressed during or after first line treatment, with a median PFS of 5.2 months (range 1.6-15 months), while 14 patients (34.1%) had a stable disease.At the beginning of second line treatment, 13 patients presented a stage III and 28 a stage IV disease. Median age was 56 years (range 42-71) and ECOG PS was 0/1/2 in 26, 8 and 7 patients (Table 1).
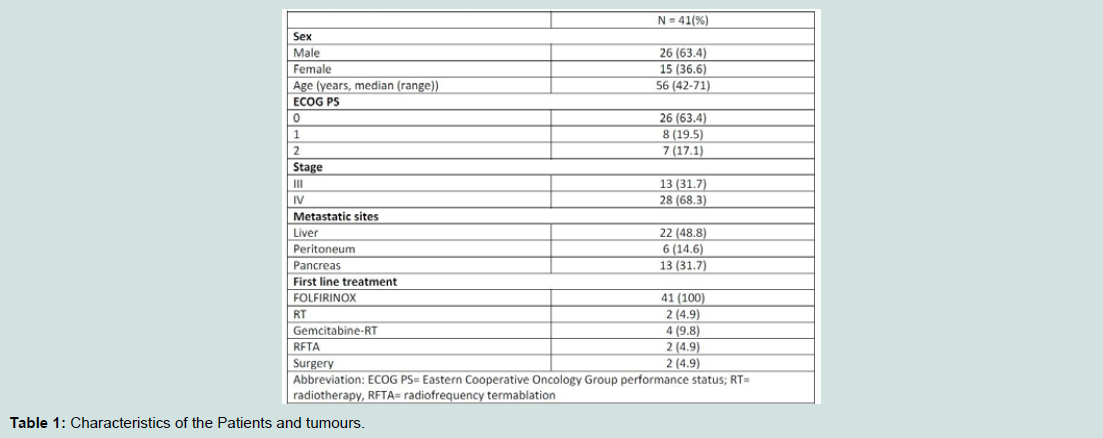
Table 1: Characteristics of the Patients and tumours.

Table 2: Safety evaluated according to National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) v 4.03.

Table 3: Efficacy of gemcitabine-capecitabine plus intra-arterial epirubicin-cisplatin therapy in 35 evaluable patients.
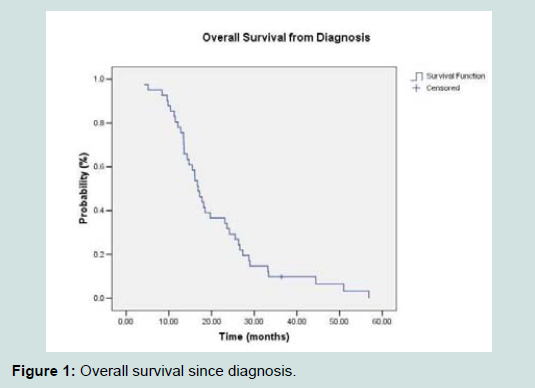
Figure 1: Overall survival since diagnosis.
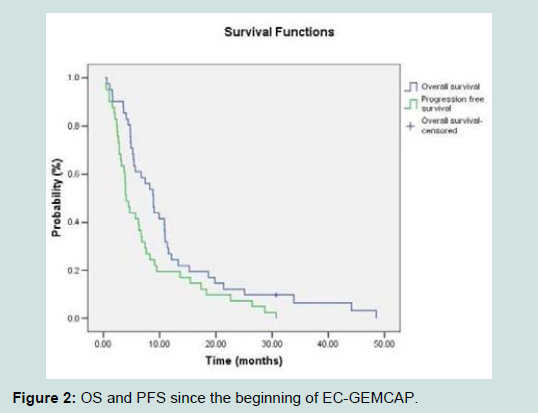
Figure 2: OS and PFS since the beginning of EC-GEMCAP.
Discussion
Although many improvements have been made in the treatment of locally advanced pancreatic cancer, median overall survival reaches only 11.1 months for FOLFIRINOX and 8.5 months for nab-paclitaxel and gemcitabine [4,15], with recurrence or progression disease within 6 months from chemotherapy end. Since many patients are still fit, a second line treatment might be a reasonable choice after first line chemotherapy progression. Of course, a second line should take into account not only the previous treatments, but even patient physical condition, residual toxicity and potential side effects of other regimens.Today, there is no consensus second line chemotherapy regimen [16]. Many phase 2 or 3 second line chemotherapy trials tested several drugs, such as gemcitabine, 5-fluorouracile, oxaliplatin, cisplatin, taxoter, irinotecan, liposomal irinotecan, nab-paclitaxel, alone or in combination, after a based gemcitabine (alone or in combination) or 5-flourouralice plus cisplatin first line chemotherapy, showing a median PFS of 2.3 months (range 1.5-5.1) and a median OS of 4.82 months (range 3.3-9.9) [17-26].
Regarding second line chemotherapy after FOLFIRINOX, in the Conroy et al. study 80 patients received gemcitabine (82.5%) or a gemcitabine based chemotherapy (12.5%), while 85 patients in gemcitabine first line chemotherapy group received a second line with FOLFOX (49.4%), or gemcitabine plus cisplatin (17.6%), or a regimen of fluorouracil and leucovorin plus cicplatin (16.5%), or FOLFIRINOX (4.7%) [4]. Interesting, no difference in median OS was noted between the groups (4.4 month in each arm) from the introduction of second line therapy.
Most recently, Portal et al. reported results on 57 patients prospectively treated with nabpaclitaxel and gemcitabine after FOLFIRINOX failure [27]. During the recruitment period, 110 patients stopped FOLFIRINOX for progression or toxicity, and 77 (70%) of them were eligible to receive nab-paclitaxel plus gemcitabine. A total of 248 cycles were administered (median per patient 4, range 1-12). Treatment was stopped in 42 patients (74%) due disease progression (40 patients) or unacceptable toxicity (2 patients). Grade 3-4 toxicities occurred in 21 patients (38%) and consisted mainly of haematological adverse effects (neutropenia: 12.5%; thrombocytopenia: 6.5%; anaemia: 3.5%, asthenia: 9%, neurotoxicity: 12.5%). No toxic deaths occurred. Thirty-eight patients (67%) had a transient or permanent dose reduction (gemcitabine 49%, nab-paclitaxel 64%) because of asthenia (32%), haematological toxicities (45%) or peripheral neurotoxicity (29%). Seven patients (12.5%) had to stop Nab-paclitaxel permanently because of peripheral neurotoxicity [4], hematological toxicity [2] or asthenia [1]. As regard efficacy, a clinical response was observed in 19 patients (33%), clinical stability in 21 patients (37%) and clinical progression in 17 patients (30%). Nab-paclitaxel plus gemcitabine resulted in an improvement in pain and asthenia in 63% of patients.
After a median follow-up of 17.5 months (range 5-45) since the beginning of FOLFIRINOX and 6 months (range 0.7-16 months) since the beginning of Nab-paclitaxel plus gemcitabine, median OS was 8.8 months (95% CI: 6.2-9.7). The OS rates at 6 and 12 months were, respectively, 69% (95% CI: 0.53-0.80) and 15% (95% CI: 0.03-0.36). Median PFS was 5.1 months (95% CI: 3.2-6.2). The PFS rates at 6 and 12 months were, respectively, 39% (95% CI: 0.25-0.52) and 6% (95% CI: 0.01-0.23). Median OS and PFS since the beginning of firstline chemotherapy (FOLFIRINOX) was 18 months (95% CI: 16-21.2) and 14 (95% CI: 12.8-15.4) months respectively.
Similarly, Caparello et al. conducted a prospective evaluation of 71 patients who underwent second line chemotherapy after modified FOLFIRINOX [28]. Likewise to the report by the French colleagues, 66% of the progressed patients were able to start a second-line treatment, with a combination regimen in 52% of the cases. Unfortunately, second-line treatment did not provide such encouraging results, achieving a median PFS of only 2.5 months, a median OS of 6.2 months and even a lower disease control rate compared with the report published by Portal et al (34% vs 58%), after a median follow up of 20.1 months. Of note, baseline patient characteristics in the two series were similar, with the sole exception of PS, as we included only 2.8% of patients with ECOG PS 2. Also in 13 patients (18%) treated with gemcitabine plus nab-paclitaxel after FOLFIRINOX, results disappointed in terms of both activity (RR: 7%; DCR: 23%) and survival (median PFS: 1.95 months; median OS: 5.4 months).
Regarding our study, we retrospectively analysed data about a homogeneous group of 41 patients treated with FOLFIRINOX first line chemotherapy and all underwent to EC-GEMCAP second line treatment after FOLFIRINOX failure (27 (65.9%) patients) or stable disease (14 (34.1%) patients). After a median follow-up of 16.9 months (range 4.2-56.9 months) since diagnosis, median OS was 16.9 months (95% CI: 14.74-19.0) with a OS rates at 6, 12 and 24 months of 95.1%, 80.5% and 31.7%, respectively.
As regards second line therapy, after median follow-up of 8.9 months (range 0.6-48.5 months) median OS was 8.9 months (95% CI: 6.9-10.9). The OS rates at 6, 12 and 24 months were 61%, 80.5% and 31.7%, respectively. EC-GEMCAP median PFS was 4.1 months (95% CI: 3.1-5.1). The PFS rates at 6 and 12 months were, respectively, 41.5% and 19.5%.
Although these data are lower, the finally median OS was similar to that emerged in the Portal trials (8.9 months, 95% CI: 6.9-10.9, vs 8.8 months, 95% CI: 6.2-9.7, respectively). Also DCR was similar in both studies (62.3% vs 58%). Interesting, EC-GEMCAP was well tolerated, without dose reductions or delays. Grade 3-4 EC-GEMCAP hematologic and no-hematologic toxicities were 39% (leucocytopenia 24.4%, thrombocytopenia 14.6%) and 12.2% (fatigue 2.4%, vomiting 7.3%, diarrhoea 2.4%), respectively (Table 2), which has definitely helped to maintain a discreet ECOG PS during all treatment, avoiding the deterioration of the general conditions that often lead to early discontinuation of therapy and bad prognosis.
Finally, anecdotal, the case of a patient with locally advanced disease underwent to radically surgery after 6 cycles of EC-GEMCAP therapy. The patients are still alive from the diagnosis of April 2012, with a OS of 51 months. Intra-arterial therapy could in fact contribute to a better cytoreductive effect for the purposes surgery, without giving sequelae of peritumoral tissues, as often happens after radiation therapy.
Of course, our trial has several limitations as the retrospective nature, the number of sample, the lack of a randomization design and quality of life evaluation, but showed than EC-GEMCAP may be a viable second line therapeutic alternative after FOLFIRINOX, also in patients without optimal general conditions.
On the basis of these results, considering the most effective therapeutic potential of new drugs, we have planned two studies of chemotherapy with nab-paclitaxel-gemcitabine plus Intra-arterial Epirubicin-Cispatin as neoadjuvant and second line therapy in pancreatic cancer patients.
References
- Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, 2013. CA Cancer J Clin 63: 11-30.
- Ferlay J, Parkin DM, Steliarova-Foucher E (2010) Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer 46: 765-781.
- Hidalgo M (2010) Pancreatic cancer. N Engl J Med 362: 1605-1617.
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, et al. (2011) FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 364: 1817-1825.
- Aigner KR, Muller H, Bassermann R (1990) Intra-arterial chemotherapy with MMC, CDDP and 5-FU for non resectable pancreatic cancer: A phase II study. Reg Cancer Treat 3: 1-6.
- Link KH, Gansauge F, Pillash J, Rilinger N, Büchler MW, et al. (1994) Regional treatment of advanced nonresectable and of resected pancreatic cancer via celiac axis infusion. Dig Surg 11: 414-419.
- Muchmore JH, Preslan JE, George WJ (1996) Regional chemotherapy for inoperable pancreatic carcinoma. Cancer 78(3 Suppl): 664-673.
- Fiorentini G, Poddie D, Ricci S, Leoni M, Cantore M, et al. (1996) Intra-aortic stop-flow infusion (IASFI) with hypoxic abdominal perfusion (HAP) in UICC stage III/IV pancreatic carcinoma (PC): Report of a phase II study. Reg Cancer Treat 9: 88-91.
- Cantore M, Fiorentini G, Bassi C, Molani L, Aitini E, et al. (1997) Intra-arterial chemotherapy for stage-III/IV pancreatic cancer. Dig Surg 14: 113-118.
- Muchmore JH (1995) Treatment of advanced pancreatic cancer with regional chemotherapy plus hemofilatration. Semin Surg Oncol 11: 154-167.
- Link KH, Gansauge F, Pillasch J, Beger HG (1997) Multimodal therapies in ductal pancreatic cancer: The future. Int J Pancreatol 21: 71-83.
- Mambrini A, Sanguinetti F, Pacetti P, Caudana R, Iacono C, et al. (2006) Intra-arterial infusion of 5-fluorouracil, leucovorin, epirubicin and carboplatin (FLEC regimen) in unresectable pancreatic cancer: results of a ten-year experience. In Vivo 20(6A): 751-755.
- Cantore M, Serio G, Pederzoli P, Mambrini A, Iacono C, et al. (2006) Adjuvant intra-arterial 5-fluoruracil, leucovorin epirubicin and carboplatin with or without systemic gemcitabine after curative resection for pancreatic adenocarcinoma. Cancer Chemother Pharmacol 58: 504-508.
- Mambrini A, Pacetti P, Del Freo A, Seta RD, Pezzuolo D, et al. (2009) Gemcitabine-capecitabine plus intra-arterial epirubicin-cisplatin in preatreated pancreatic cancer patients: a phase I study. Anticancer Res 29: 1547-1549.
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, et al. (2013) Increased survival in pancreatic cancer with nab-Paclitaxel plus gemcitabine. N Engl J Med 369: 1691-1703.
- Rahma OE, Duffy A, Liewehr DJ, Steinberg SM, Greten TF (2013) Second-line treatment in advanced pancreatic cancer: a comprehensive analysis of published clinical trials. Ann Oncol 24: 1972-1979.
- Dahan L, Bonnetain F, Ychou M, Mitry E, Gasmi M, et al. (2010) Combination 5-fluorouracil, folinic acid and cisplatin (LV5FU2-CDDP) followed by gemcitabine or the reverse sequence in metastatic pancreatic cancer: final results of a randomised strategic phase III trial (FFCD 0301). Gut 59: 1527-1534.
- Gill S, Ko YJ, Cripps MC, Beaudoin A, Dhesy-Thind SK, et al. (2014) PANCREOX: A randomized phase 3 study of 5FU/LV with or without oxaliplatin for second-line advanced pancreatic cancer (APC) in patients (pts) who have received gemcitabine (GEM)-based chemotherapy (CT). J Clin Oncol 32(Suppl): 5s.
- Hosein PJ, de Lima Lopes G Jr, Pastorini VH, Gomez C, Macintyre J, et al. (2013) A phase II trial of nab-Paclitaxel as second-line therapy in patients with advanced pancreatic cancer. Am J Clin Oncol 36: 151-156.
- Oettle H, Riess H, Stieler JM, Heil G, Schwaner I, et al. (2014) Second-line oxaliplatin, folinic acid, and fluorouracil versus folinic acid and fluorouracil alone for gemcitabine-refractory pancreatic cancer: outcomes from the CONKO-003 trial. J Clin Oncol 32: 2423-2429.
- Pelzer U, Schwaner I, Stieler J, Adler M, Seraphin J, et al. (2011) Best supportive care (BSC) versus oxaliplatin, folinic acid and 5-fluorouracil (OFF) plus BSC in patients for second-line advanced pancreatic cancer: a phase III-study from the German CONKO-study group. Eur J Cancer 47: 1676-1681.
- Portal A, Pernot S, Siauve N, Landi B, Lepe`re C, et al. (2014) Sustained response with gemcitabine plus Nab-paclitaxel after folfirinox failure in metastatic pancreatic cancer: report of an effective new strategy. Clin Res Hepatol Gastroenterol 38: e23-e26.
- Soares HP, Bayraktar S, Blaya M, Lopes G, Merchan J, et al. (2014) A phase II study of capecitabine plus docetaxel in gemcitabine-pretreated metastatic pancreatic cancer patients: CapTere. Cancer Chemother Pharmacol 73: 839-845.
- Von Hoff D, Li CP, Wang-Gillam A, Bodoky G, Dean A, et al. (2014) NAPOLI-1: Randomized phase 3 study of MM-398 (NAL-IRI), with or without 5-fluorouracil and leucovorin, versus 5-fluorouracil and leucovorin, in metastatic pancreatic cancer progressed on or following gemcitabine-based therapy. Ann Oncol 25(Suppl 2): S105-S106.
- Yoo C, Hwang JY, Kim JE, Kim TW, Lee JS, et al. (2009) A randomised phase II study of modified FOLFIRI.3 vs modified FOLFOX as second-line therapy in patients with gemcitabine-refractory advanced pancreatic cancer. Br J Cancer 101: 1658-1663.
- Zaanan A, Trouilloud I, Markoutsaki T, Gauthier M, Dupont-Gossart AC, et al. (2014) FOLFOX as second-line chemotherapy in patients with pretreated metastatic pancreatic cancer from the FIRGEM study. BMC Cancer 14: 441.
- Portal A, Pernot S, Tougeron D, Arbaud C, Bidault AT, et al. (2015) Nab-paclitaxel plus gemcitabine for metastatic pancreatic adenocarcinoma after folfirinox failure: an AGEO prospective multicentre cohort. BMC Cancer 113: 989-995.
- Caparello C, Vivaldi C, Fornaro L, Musettini G, Pasquini G, et al. (2016) Second-line therapy for advanced pancreatic cancer: evaluation of prognostic factors and review of current literature. Future Oncol 12: 901-908.