
Research Article
*Address for Correspondence Matthew T. Keough, Department of Psychology, Concordia University, PY-239, 7141 Sherbrooke St. West, Montreal, Quebec, Canada, H4B 1R6, Tel: 514-848-2424 ext. 2390; Fax: 514-848-4523;; E-mail: m_keough@live.concordia.ca
Citation: Keough MT, Hines S, Winslade A, O’Connor RM. Negative Urgency and Gender Moderate the Association between Anxiety Sensitivity and Alcohol-Related Problems. J Addiction Prevention. 2015;3(1): 7.
Copyright © 2015 Keough MT, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Addiction & Prevention | ISSN: 2330-2178 | Volume: 3, Issue: 1
Submission: 16 March, 2015 | Accepted: 20 April, 2015 | Published: 25 April, 2015
Negative Urgency and Gender Moderate the Association between Anxiety Sensitivity and Alcohol-Related Problems
Matthew T. Keough1*, Sarah Hines1, Amanda Winslade2, and Roisin M. O’Connor1
- Department of Psychology, Concordia University, Montreal, Québec, Canada Department of Psychology, McGill University, Montreal, Quebec, Canada
*Address for Correspondence Matthew T. Keough, Department of Psychology, Concordia University, PY-239, 7141 Sherbrooke St. West, Montreal, Quebec, Canada, H4B 1R6, Tel: 514-848-2424 ext. 2390; Fax: 514-848-4523;; E-mail: m_keough@live.concordia.ca
Citation: Keough MT, Hines S, Winslade A, O’Connor RM. Negative Urgency and Gender Moderate the Association between Anxiety Sensitivity and Alcohol-Related Problems. J Addiction Prevention. 2015;3(1): 7.
Copyright © 2015 Keough MT, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Addiction & Prevention | ISSN: 2330-2178 | Volume: 3, Issue: 1
Submission: 16 March, 2015 | Accepted: 20 April, 2015 | Published: 25 April, 2015
Abstract
Tension reduction theory states that persons high in anxiety sensitivity (AS) are particularly sensitive to alcohol’s anxiolytic effects and thus may engage in problematic drinking to reduce distress. However, the literature is mixed, suggesting a complex AS pathway to problematic drinking. Elevated AS may promote drinking to alleviate anxiety, while alcohol’s initial aversive physiological effects (e.g., increased heart rate) and potentially negative outcomes may deter use among those high in AS. For anxiety sensitive persons to drink, they must temporarily disregard alcohol’s negative effects and instead focus on the immediate tension-reducing effects of drinking. Accordingly, anxiety sensitive individuals, who act impulsively when anxious (i.e., negative urgency), may be at risk for heavy drinking and experiencing alcohol-related problems. The goal of our study was to test this prediction. Given that gender differences have been consistently documented in the alcohol use literature, we also examined gender as a secondary moderator.Method: Undergraduates (N=346) completed self-reports of AS, negative urgency, and drinking habits.
Results: Moderation analyses revealed that AS positively predicted alcohol-related problems, but only when negative urgency was elevated and this was true for men but not for women. Counter to predictions, the effect of AS on alcohol use was not moderated by negative urgency. However, gender did moderate the AS-alcohol use association, such that AS was negatively associated with alcohol use in men, but was unrelated in women.
Conclusions: We found partial support for our hypotheses. Our findings place anxiety sensitive men, who are also high in negative urgency, at unique risk for alcohol-related problems. Clinical interventions may benefit from concurrently targeting negative urgency to reduce problematic drinking risk among anxiety sensitive men.
Keywords
Anxiety sensitivity; Negative urgency; Alcohol use; Gender; Alcohol-related problemsIntroduction
Anxiety Sensitivity (AS) is an individual difference that may relate to problematic drinking risk. AS is the fear that anxiety-related bodily sensations (e.g., increased heart rate) will lead to catastrophic outcomes, such as physical illness, social embarrassment, and/or a loss of control [1,2]. Those with elevated AS experience frequent and intense anxiety symptoms and research places these individuals at risk for developing anxiety disorders (e.g., panic disorder) [3,4]. Tension reduction theory [5,6] and the stress-dampening hypothesis [7,8] predict that high levels of fear and worry increase the likelihood that a person will use alcohol to cope with these aversive states. Specifically, given that alcohol has anxiolytic effects, those with high levels of AS may be particularly inclined to drink to alleviate anxiety and dampen associated bodily symptoms [9,,10]. Supporting theory,data shows that AS is positively linked to coping-related drinking [11,12] and drinking to cope has been consistently linked with unique risk for alcohol-related problems, irrespective of level of use [13]. Some work also demonstrates that elevated AS is a premorbid risk factor for developing alcohol use disorders later in adulthood [14].While theory predicts that those high in AS may drink alcohol to reduce anxiety, the documented associations between AS and problematic drinking (i.e., alcohol use and experiencing related problems) are mixed [15,17]. These inconsistent findings suggest that the association between AS and problematic drinking is complex. Namely, research shows that alcohol use leads to physiological changes that individuals with elevated AS should find aversive [18,19]. For example, alcohol has been shown to mimic symptoms of anxious arousal (i.e., rapid heart rate, blushing), especially in the early stages of drinking [18]. Thus, while those with elevated AS may drink to reduce anxiety, they may also avoid drinking due to finding these initial physiological effects aversive. Intoxication may also exacerbate fears related to loss of control and social embarrassment, which may further contribute to alcohol avoidance by those high in AS. Overall, the mixed literature and complexity of the AS-pathway suggests a need to examine potential moderators.
To date, there is a paucity of research examining moderators of the effect of AS on problematic drinking behavior. Two existing studies investigated the moderating roles of gender and alcoholrelated motives/cognitions [20,21]. In one study, Novak and colleagues found that AS was unrelated to alcohol use for both men and women and that coping motives for drinking did not moderate the AS-alcohol use association [20]. In a second study, O’Connor et al. found that, for men only, AS was positively linked with alcohol use, but only when tension reduction alcohol expectancies were high [21]. For women, elevated AS was marginally supported as a predictor of reduced alcohol use, but only when cognitive and behavioral impairment alcohol expectancies were high. While these studies represent important steps in the AS-problematic drinking literature, they do not clarify from an individual difference perspective why some persons high in AS may drink alcohol to alleviate anxiety, while others may avoid heavy drinking due to fear of alcohol-related negative outcomes. This suggests the need to examine additional individual difference factors that contribute to AS-related drinking.
For those with elevated AS to drink, they must disregard (at least temporarily) the initial and delayed negative effects of alcohol use and instead focus on the more immediate anxiolytic or tension-reducing effects of drinking. Accordingly, anxiety sensitive individuals, who act impulsively when anxious, should be those at risk for heavy drinking and experiencing alcohol-related problems. The tendency to act rashly when emotionally distressed is referred to as negative urgency [22]. Individuals high in negative urgency display a decreased tolerance for negative emotions and often act in risky ways to reduce distress. With respect to the current study, we propose that negative urgency moderates the association between AS and problematic drinking. Specifically, it is those high in AS, who are also high in negative urgency, that are at particular risk for engaging in spontaneous and risky self-medication drinking. This prediction remains untested in the extant literature.
Men show higher rates of alcohol use and overall alcohol-related problems compared to women [23,24]. Also, while some studies show that women undergraduates relative to men have higher rates of AS [21,25], work by Lawyer and colleagues indicates a stronger association between AS and drinking for coping-related purposes (e.g., alleviate anxiety) among men than among women [26]. Moreover, the study by O’Connor and colleagues also demonstrated that men, who also had strong expectations of tension relief from alcohol, were the ones who drank heavily [21]. In sum, extant work identifies gender as an important moderator of the AS-related pathway to problematic drinking. Accordingly, we examined gender as an additional moderator in our study.
The goal of our study was to clarify the relation between AS and problematic drinking. We aimed to do this by testing the primary moderating role of negative urgency and the secondary moderating role of gender. Based on theory [6,8], we hypothesized that elevated AS would be associated with both increased alcohol use and alcoholrelated problems but only when negative urgency was also elevated. Further, based on extant work examining gender differences [21,26], we expected that when negative urgency was elevated, there would be a stronger link between AS and problematic drinking in men compared to women. Consistent with work on coping-related drinking [13], we tested unique effects from predictors to alcohol use and related problems by controlling for the drinking variable not specified as the outcome.
Materials and Methods
Participants and procedureUndergraduates (N = 346, age range 19-25 years old, 195 women) volunteers were recruited from two large universities, one in Eastern Canada (N = 270) and one in the North West United States (N = 76). Recruitment methods included advertisements via an online participant pool and via flyers posted on campus. The majority of participants were Caucasian (83%). Many students lived in a house/apartment not with family (64%), while 15% lived at home with family; 12% lived in residence hall; and the remaining 9% lived in a fraternity/sorority or campus apartment. Forty-three percent of students reported not having a job outside of school; 49% reported working part-time and the remaining 8% worked full time. Participants completed the measures of this study as part of the baseline assessment for a larger, lab-based experimental study. Because the larger study included alcohol administration (after completion of baseline assessments), only those of legal drinking age (≥19 and ≥21 years old in Canada and USA, respectively) and who were non-abstainers (i.e., > one drink the past month) participated. Participants received course credit or $10/hour as compensation. All study procedures were approved by the Health Services Research Ethics Board at Dalhousie University and by the Institutional Review Board at the University of Washington.
Measures
Anxiety Sensitivity Index [2]: The original 16-item Anxiety Sensitivity Index was used. Participants responded to items (e.g., “It scares me when my heart beats rapidly”) using a 5-point scale, indicating their agreement with each item (1 = Very Little to 5 = Very Much). A sum score was calculated. In line with extant work [2], this subscale had good internal consistency in our sample (α = .85).
Negative urgency [27]: The 12-item urgency subscale of the UPPS Impulsive Behavior Scale was used to assess distress-related impulsivity. Participants responded to items (e.g., “When I am upset, I often act without thinking”) using a 5-point scale, indicating the degree to which each item described them (1 = Not at all to 5 = Extremely). A mean score was calculated. As in previous work [27,28] the internal consistency of this subscale was good in our sample (α = 0.86).
Young Adult Alcohol Consequences Questionnaire (YAACQ) [29]: The YAACQ is a 48-item self-report measure of alcohol-related problems. Participants indicated whether or not they experienced each alcohol-related problem in the past year (1 = yes; 0 = no). Yes responses were summed to provide a total score. Consistent with previous work [30] using tetrachoric correlations, the internal consistency of the YAACQ was excellent in our sample (α = 0.95).
Alcohol consumption [31,32]: Participants indicated their past month typical frequency (0 = not at all in the past 30 days to 7 = every day of the week) and quantity (0 = did not drink at all in the past 30 days to 10 = ten drinks per occasion) of alcohol use. Consistent with previous work [33,34], responses were multiplied to yield a composite indicating total weekly alcohol use.
Results
Data analytic overviewData were screened prior to analyses [35]. There were no missing data and outliers on all variables were replaced with the highest acceptable observation within the + 3SD range (4 outliers on alcohol use, 1 outlier on alcohol-related problems; <1% of data). Next, descriptive statistics and correlations were examined followed by multiple regression analyses to test negative urgency and gender as moderators of the association between AS and problematic drinking. Continuous predictors (AS and negative urgency) were centered prior to creating interaction terms to reduce multicollinearity. Gender was initially coded as women = 0 and men = 1. Statistically supported interaction terms were probed using simple slopes analysis. Consistent with recommendations by Aiken and West (1991) [36], the model was conditioned on high (+1SD above the mean) and low (-1SD above the mean) levels of negative urgency and levels of gender.
Descriptive statistics and correlations
Correlations and descriptive statistics for all variables are presented in Table 1. Relative to extant work on North American drinkers, our sample had comparable mean levels of alcohol use and alcohol-related problems [29,37]. Consistent with some work [38], AS was positively correlated with alcohol-related problems, but not with alcohol use. As expected, negative urgency was positively correlated with both alcohol use and alcohol-related problems. Also, in line with previous work [23,24] and predictions, men consumed more alcohol and experienced more alcohol-related problems than women. Hypothesis testing
Hypothesis testing
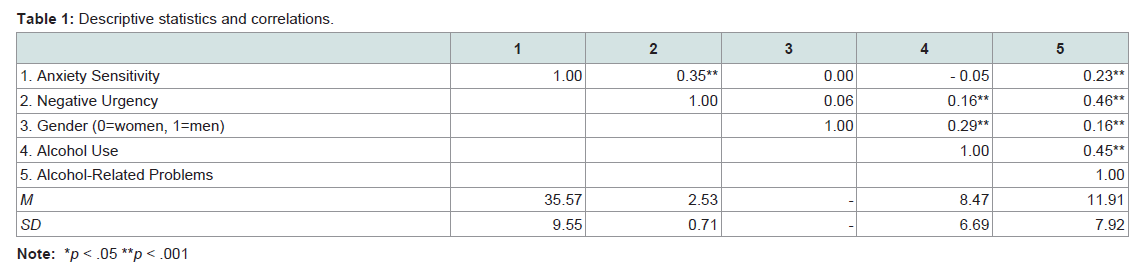
Table 1: Descriptive statistics and correlations.
Two separate regression models were used to test hypotheses. In model one, alcohol use (criterion variable) was regressed on the first order effects of AS, negative urgency, and gender, all two-way interactions, and the three way interaction of interest. The alcohol alcoholrelated problems variable was included as a covariate. This model accounted for approximately 31% of the variance in alcohol use. As seen in Table 2, the AS × Negative Urgency × Gender interaction term was not statistically significant, but statistically significant two-way interaction terms were observed (AS × Gender and Negative Urgency × Gender). Simple slopes analyses of these two-way interactions revealed that AS was a statistically significant negative predictor of alcohol use for men (B = -0.21, t(337) = -3.64, p < 0.001, f2 = 0.05), but not for women (B = -0.04, t(337) = -0.89, p = 0.38, f2 < 0.001). Also, negative urgency was a statistically significant positive predictor of alcohol use for men (B = 1.66, t(337) = 2.07, p = 0.04, f2 = 0.02) but not for women (B = -0.90, t(337) = -1.43, p = .15, f2 < 0.001). In model two, alcohol-related problems (criterion variable) was regressed on the first order effects of AS, negative urgency, and gender, all two-way interactions, and the three way interaction of interest. The alcohol use variable was included as a covariate. This model accounted for 42% of the variance in alcohol-related problems. The three-way AS × Negative Urgency × Gender interaction term received marginal statistical support (p < 0.10) (see Table 2). The three-way interaction term was probed by at high and low levels of negative urgency and by gender. We observed a statistically significant two-way AS × Negative Urgency interaction term when the model was conditioned on men (B = 0.24 [SE = 0.09], b = 0.31, p = 0.01) but not women (B = 0.03 [SE = 0.06], b = 0.04, p = 0.57) gender. Further, as expected, we found that AS was positively associated with alcohol-related problems at high (B = 0.32, t(337) = 3.68, p = 0.00, f2 = 0.04), but not at low (B = -0.02, t(337) = -0.24, p = 0.81, f2 = 0.00), levels of negative urgency in men (see Figure 1). This effect was not supported in women.
In model two, alcohol-related problems (criterion variable) was regressed on the first order effects of AS, negative urgency, and gender, all two-way interactions, and the three way interaction of interest. The alcohol use variable was included as a covariate. This model accounted for 42% of the variance in alcohol-related problems. The three-way AS × Negative Urgency × Gender interaction term received marginal statistical support (p < 0.10) (see Table 2). The three-way interaction term was probed by at high and low levels of negative urgency and by gender. We observed a statistically significant two-way AS × Negative Urgency interaction term when the model was conditioned on men (B = 0.24 [SE = 0.09], b = 0.31, p = 0.01) but not women (B = 0.03 [SE = 0.06], b = 0.04, p = 0.57) gender. Further, as expected, we found that AS was positively associated with alcohol-related problems at high (B = 0.32, t(337) = 3.68, p = 0.00, f2 = 0.04), but not at low (B = -0.02, t(337) = -0.24, p = 0.81, f2 = 0.00), levels of negative urgency in men (see Figure 1). This effect was not supported in women.

Table 2: Testing negative urgency and gender as moderators of the effect of anxiety sensitivity on problematic drinking outcomes.
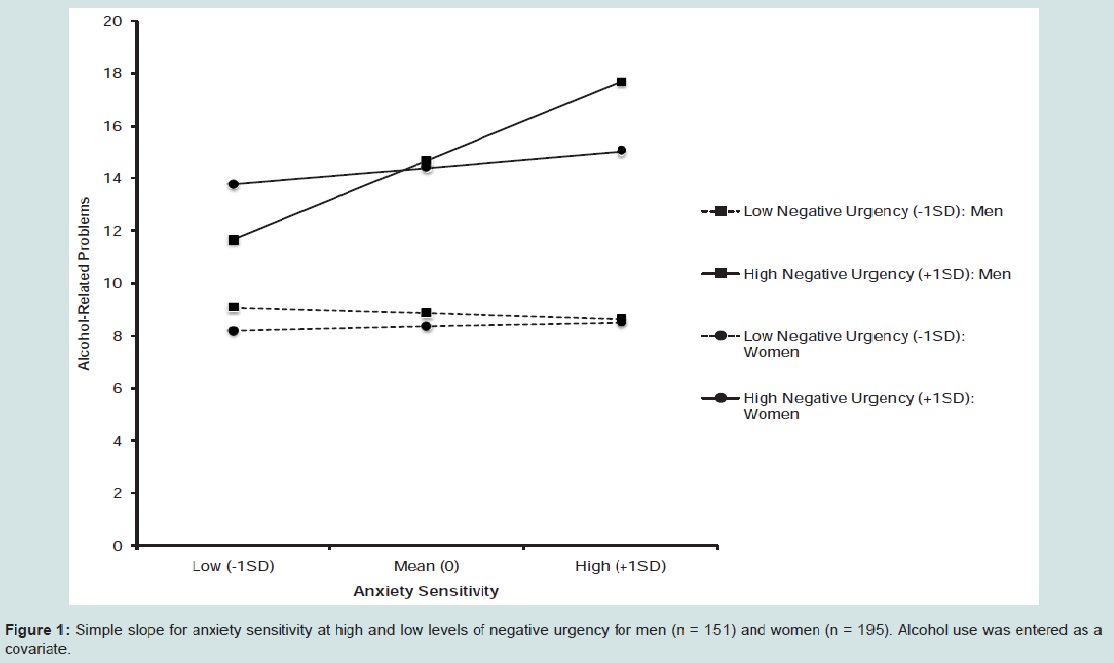
Figure 1: Simple slope for anxiety sensitivity at high and low levels of negative urgency for men (n = 151) and women (n = 195). Alcohol use was entered as a covariate.
Discussion
The primary goal of our study was to clarify the link between AS and problematic drinking. We aimed to accomplish this by testing negative urgency and gender as moderators of the AS-problematic drinking association. Our results partially supported our hypotheses. As expected, we found that elevated AS was associated with increased alcohol-related problems, but only when negative urgency was elevated and this effect was present in men but not in women. Unexpectedly, negative urgency did not moderate the effect of AS on alcohol use, while gender did. Specifically, contrary to prediction, AS was related to reduced levels of alcohol use in men, however, not unexpectedly, AS was unrelated to drinking in women. Also, consistent with previous work on impulsivity and alcohol use [39,40], elevated negative urgency predicted increased drinking in men, but not in women.One important finding from this study was that elevated negative urgency increased risk for alcohol-related problems among men who were relatively high in AS. Due to high negative urgency, the immediate anxiolytic effects of alcohol use should be salient to those who are high in AS, which may cause individuals to engage in risky and disinhibited behaviour (e.g., problematic drinking). While our study aligns with this interpretation, a specific test of alcohol expectancies in this risk model is warranted. Our finding that concurrently high AS and negative urgency is a risk factor for alcohol-related problems for men only fits well with extant findings. Not only are men found to have higher rates of impulsivity relative to women [41] but also impulsivity is found to be a more central influence of problematic drinking for men compared to women [23]. Moreover, a number of studies show that men are at increased risk relative to women for coping- and anxiety-related drinking [21,26,42,43]. Our findings bring these literatures together, suggesting that elevated negative urgency may in part help us understand these gender effects we see in the anxiety-drinking risk pathway.
Counter to predictions, we did not find support for the moderating role of negative urgency on the AS-alcohol use association and unexpectedly elevated AS predicted decreased alcohol use in men. A review of the negative reinforcement-motivated drinking literature indicates that these results are not that surprising. Much of the evidence demonstrates that drinking to alleviate negative affect increases specific risk for alcohol-related problems, irrespective of use [13]. Moreover, the link between coping-related drinking and levels of alcohol use is highly mixed in young adults [44-47]. Without considering gender, we found a null zero-order correlation between AS and typical weekly alcohol use, supporting the commonly reported notion that the link between negative affect and alcohol use is not straightforward [48].
O’Connor and colleagues found that AS was positively related to alcohol use in men but only if they had high tension-reduction expectancies [21]. Accordingly, it could be that the theoretically proposed positive link between AS and alcohol use may depend on additional factors not considered in the present study. To illustrate, theory predicts that heavy drinking among those high in AS should be most reinforcing in contexts where anxious affect is elevated [10]. Supporting this, persons with elevated AS have been shown to drink heavily specifically when negative emotionality is high (e.g., conflict with others) [49] and this relation is stronger for men than for women [26]. We did not consider context-specific use in our models, instead, it is possible that our global measure of weekly alcohol use did not tap heavy drinking of interest – that is, heavy drinking among those high in AS when they are anxious. This may account for why our effects differ from those reported in other studies (e.g., [49]). It would be beneficial for future studies to examine how the interaction between AS and negative urgency plays out in men to predict alcohol use in contexts where emotional distress is high. Our results also indicate that men are likely to drink more (relative to women) if they also have elevated negative urgency. This result aligns with the broad literature on impulsivity and alcohol use (see Dick et al. [50] for a recent review) and suggests that men may be inclined to engage in risky in-the-moment alcohol use due to their intolerance of emotional distress.
Overall, our results indicate that AS is a complex predictor of drinking in men, but may be less relevant to women’s drinking. These results are consistent with numerous studies supporting gender differences in anxiety-related drinking. The clinical literature suggests that men (vs. women) with Panic Disorder are more likely to report drinking for coping reasons [51] and in turn, this type of drinking has been firmly linked with risk for alcohol-related problems (see Kuntsche et al. [31] for a review). While we examined risk at the sub-clinical level of any anxiety disorder, our finding with respect to alcohol-related problems is consistent with this literature. Despite this, the null association between AS and drinking for women was surprising because there is a documented high co-morbidity of anxiety disorders and alcohol use disorders in later adulthood among women [52,53]. Our null findings in women may reflect gender differences in coping styles at the young adulthood stage of development. While the coping literature is complex, some work indicates that women are more likely than men to seek social and emotional support [54], whereas, men tend to use avoidant coping strategies (e.g., alcohol use) [55]. The social nature of university may offer much needed support for anxiety sensitive women – mitigating the need to use alcohol to cope. Anxiety sensitive women may experience a dropoff in social support resources when transitioning out of university, which may cause them to adopt other coping strategies, like alcohol use. Informed by developmental theories of alcohol use risk [56,57], we speculate that alcohol use as a primary coping strategy may unfold over adulthood in anxiety sensitive women. Future work should clarify this by continuing to examine gender-specific etiological models as anxiety sensitive persons – who are also high in negative urgency – move through adulthood.
Our results may help inform clinical intervention and prevention efforts for reducing problematic drinking among those with elevated AS. Evidence-based treatments, such as Cognitive-Behaviour Therapy (CBT [58]) and/or personality-matched interventions [59,60], have been shown to be useful for reducing both AS symptoms, as well as concurrent alcohol use problems. The main rationale behind these treatments is to target AS symptoms using cognitive and behavioral strategies (e.g., psychoeducation, introceptive exposure) and thus allow individuals to become tolerant of anxiety symptoms [58,61,62]. Our results suggest that it may be additionally beneficial to target factors like distress tolerance and behavioural disinhibition to reduce risk for alcohol use and related problems among anxiety sensitive men. This may help slow down the impulsivity of risky distressrelated drinking among these individuals.
There are some notable limitations of this study. First, this study is cross-sectional and we are limited in making assertions about causality. Learning processes (e.g., alcohol expectancies, drinking motives), which unfold over time and through experience, may be important explanatory factors that underlie drinking among those high in AS and high in negative urgency. However, this remains to be explicitly tested in future experimental and longitudinal work. Second, given our quasi-experimental design, we were unable to capture – in the moment – the distress-related shift into impulsive behaviour that is believed to effect problematic drinking in persons high in AS and negative urgency. Accordingly, future work should expand on our models by using experimental methods to assess this shift (anxious mood induction coupled with measurement of impulsivity) and its subsequent impact on in-lab drinking among those high in AS. Finally, we used the original Anxiety Sensitivity Index [2], which captures mainly physiological aspects of AS. Updated work and measures (i.e., the Anxiety Sensitivity Index-3 [63]) indicate that AS is multifaceted and includes physiological, cognitive, and social features. For example, social AS is characterized by fears that publically observable anxiety symptoms will lead to social rejection and ridicule from peers [63] and this may be particularly concerning in university settings where normative drinking is at social events [64]. Possibly, elevated negative urgency may draw attention to the positive social aspects of drinking (e.g., social affiliation, being included by peers) among those high in social AS. Consistent with studies on drinking norms (e.g., [65]), this may lead those high in social AS and negative urgency to overestimate the drinking of their peers, which may increase their own risk for drinking heavily and experiencing related problems. It would be interesting for future studies to examine this possibility – with a continued focus on also understanding gender-specific risk.
In conclusion, the main strength of our study is that we are among the first to examine negative urgency and gender as theoretically relevant moderators of the AS-problematic drinking association. Results indicated that AS is a complex risk factor for drinking behaviour among men, but not among women in our sample. These findings provide insight into contributing factors underlying ASrelated drinking and serve to provide a strong foundation for future empirical testing.
Acknowledgements
This research was funded by a Canadian Institutes of Health Research (CIHR) grant held by R. M. O’Connor. During completion of a portion of this work M. T. Keough was supported by a CIHR Vanier Canada Graduate Scholarship and R. M. O’Connor was supported in part by a CIHR New Investigator award.References
- Peterson RA, Reiss S (1993) Anxiety sensitivity index revised test manual. IDS Publ: Worthington
- Reiss S, Peterson RA, Gursky DM, McNally RJ (1986) Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behav Res Ther 24: 1-8
- Stewart SH (1996) Alcohol abuse in individuals exposed to trauma: a critical review. Psychol Bull 120: 83-112
- Taylor S (1992) How does anxiety sensitivity vary across the anxiety disorders? J Anxiety Disord 6: 249-259.
- Conger JJ (1956) Alcoholism: theory, problem, and challenge. II. Reinforcement theory and the dynamics of alcoholism. Q J Stud Alcohol 17: 296-305.
- Kushner MG, Sher KJ, Beitman BD (1990) The relation between alcohol problems and the anxiety disorders. Am J Psychiatry 147: 685-695.
- Balodis IM, Wynne-Edwards KE, Olmstead MC (2011) The stress–response-dampening effects of placebo. Horm Behav 59: 465-472.
- Sher KJ (1987) Stress response dampening. In: Blaine H, Leonard K, editors. Psychological theories of drinking and alcoholism. Guilford Press: New York.
- Pihl RO, Peterson JB (1995) Alcoholism: the role of different motivational systems. J Psychiatry Neurosci 20: 372-396.
- Stewart SH, Zvolensky MJ, Eifert GH (2001) Negative-reinforcement drinking motives mediate the relation between anxiety sensitivity and increased drinking behavior. Pers Individ Dif 31: 157-171.
- Kushner MG, Thuras P, Abrams K, Brekke M, Stritar L (2001) Anxiety mediates the association between anxiety sensitivity and coping-related drinking motives in alcoholism treatment patients. Addict Behav 26: 869-885.
- Stewart SH, Zeitlin SB (1995) Anxiety sensitivity and alcohol use motives. J Anxiety Disord 9: 229-240.
- Kuntsche E, Knibbe R, Gmel G, Engels R (2005) Why do young people drink? A review of drinking motives. Clin Psychol Rev 25: 841-861.
- Schmidt NB, Buckner JD, Keough ME (2007) Anxiety sensitivity as a prospective predictor of alcohol use disorders. Behav Modif 31: 202-219.
- Krank M, Stewart SH, O'Connor RM, Woicik PB, Wall AM, et al. (2011) Structural, concurrent, and predictive validity of the Substance Use Risk Profile Scale in early adolescence. Addict Behav 36: 37-46.
- Stewart SH, Peterson JB, Pihl RO (1995) Anxiety sensitivity and self-reported alcohol consumption rates in university women. J Anxiety Disord 9: 283-292.
- Zack M, Poulos CX, Fragopoulos F, MacLeod CM (2003) Effects of negative and positive mood phrases on priming of alcohol words in young drinkers with high and low anxiety sensitivity. Exp Clin Psychopharmacol 11: 176-185.
- Lang AR, Patrick CJ, Stritzke WG (1999) Alcohol and emotional response: A multidimensional-multilevel analysis. In: Leonard K, Blane H, editors. Psychological theories of drinking and alcoholism (2nd edn.). New York: Routledge.
- MacDonald AB, Stewart SH, Hutson R, Rhyno E, Loughlin HL (2001) The roles of alcohol and alcohol expectancy in the dampening of responses to hyperventilation among high anxiety sensitive young adults. Addict Behav 26: 841-867.
- Novak A, Burgess ES, Clark M, Zvolensky MJ, Brown RA (2003) Anxiety sensitivity, self-reported motives for alcohol and nicotine use, and level of consumption. J Anxiety Disord 17: 165-180.
- O'Connor RM, Farrow S, Colder CR (2008) Clarifying the anxiety sensitivity and alcohol use relation: considering alcohol expectancies as moderators. J Stud Alcohol Drugs 69: 765-772.
- Cyders MA, Smith GT (2008) Emotion-based dispositions to rash action: positive and negative urgency. Psychol Bull 134: 807-828.
- Nolen-Hoeksema S (2004) Gender differences in risk factors and consequences for alcohol use and problems. Clin Psychol Rev 24: 981-1010.
- Brady KT, Randall CL (1999) Gender differences in substance use disorders. Psychiatr Clin North Am 22: 241-252.
- Stewart SH, Taylor S, Baker JM (1997) Gender differences in dimensions of anxiety sensitivity. J Anxiety Disord 11: 179-200.
- Lawyer SR, Karg RS, Murphy JG, McGlynn FD (2002) Heavy drinking among college students is influenced by anxiety sensitivity, gender, and contexts for alcohol use. J Anxiety Disord 2: 165-173.
- Whiteside SP, Lynam DR (2001) The five factor model and impulsivity: Using a structural model of personality to understand impulsivity. Pers Individ Dif 30: 669-689.
- Magid V, Colder CR (2007) The UPPS Impulsive Behavior Scale: Factor structure and associations with college drinking. Pers Individ Dif 43: 1927-1937.
- Read JP, Kahler CW, Strong DR, Colder CR (2006) Development and preliminary validation of the young adult alcohol consequences questionnaire. J Stud Alcohol 67: 169-177.
- Read JP, Merrill JE, Kahler CW, Strong DR (2007) Predicting functional outcomes among college drinkers: Reliability and predictive validity of the Young Adult Alcohol Consequences Questionnaire. Addict Behav 32: 2597-2610.
- Cahalan D, Cisin IH, Crossley HM (1969) American drinking practices: A national study of drinking behavior and attitudes. New Brunswick, NJ: Rutgers Center of Alcohol Studies.
- Read JP, O’Connor RM (2006) High- and low-dose expectancies as mediators of personality dimensions and alcohol involvement. J Stud Alcohol 67: 204-214.
- Keough ME, O’Connor RM (2014) Clarifying the measurement and the role of the behavioral inhibition system in alcohol misuse. Alcohol Clin Exp Res 38: 1470-1479.
- Wardell JD, O'Connor RM, Read JP, Colder CR (2011) Behavioral approach system moderates the prospective association between the behavioral inhibition system and alcohol outcomes in college students. J Stud Alcohol Drugs 72: 1028-1036.
- Kline R (2009) Becoming a behavioural science researcher: A guide to producing research that matters. Guilford Press: New York.
- Aiken LS, West SG (1991) Multiple regression: Testing and interpreting interactions. Sage: Newbury Park.
- Mackinnon SP, Kehayes IL, Clark R, Sherry SB, Stewart SH (2014) Testing the four-factor model of personality vulnerability to alcohol misuse: a three-wave, one-year longitudinal study. Psychol Addict Behav 28: 1000-1012.
- Chandley RB, Luebbe AM, Messman-Moore TL, Ward RM (2014) Anxiety sensitivity, coping motives, emotion dysregulation, and alcohol-related outcomes in college women: a moderated-mediation model. J Stud Alcohol Drugs 75: 83-92
- Caspi A, Moffitt TE, Newman DL, Silva PA (1996) Behavioral observations at age 3 predict adult psychiatric disorders: Longitudinal evidence from a birth cohort. Arch Gen Psychiatry 53: 1033-1039.
- Rutledge P, Sher KJ (2001) Heavy drinking from the freshman year into early young adulthood: The roles of stress, tension-reduction drinking motives, gender and personality. J Stud Alcohol 62: 457-466.
- Zuckerman M, Kuhlman M (2000) Personality and risk taking: Common biosocial factors. J Pers 68: 999-1029.
- Park CL, Levenson MR (2002) Drinking to cope among college students: prevalence, problems and coping processes. J Stud Alcohol 63: 486-497.
- Cooper ML, Russell M, Skinner JB, Windle M (1992) Development and validation of a three-dimensional measure of drinking motives. J Consult Clin Psych 4: 123-132.
- Cooper ML (1994) Motivations for alcohol use among adolescents: Development and validation of a four-factor model. Addict Behav 6: 117-128.
- LaBrie JW, Ehret PJ, Hummer JF, Prenovost K (2010) Poor adjustment to college life mediates the relationship between drinking motives and alcohol consequences: a look at college adjustment, drinking motives, and drinking outcomes. Addict Behav 37: 379-386.
- Merrill JE, Read JP (2010) Motivational pathways to unique types of alcohol consequences. Psychol Addict Behav 24: 705-711.
- Patrick ME, Lee CM, Larimer ME (2011) Drinking motives, protective behavioral strategies, and experienced consequences: Identifying students at risk. Addict Behav 36: 270-273.
- Read JP, Wood MD, Kahler CW, Maddock JE, Palfai TP (2003) Examining the role of drinking motives in college student alcohol use and problems. Psychol Addict Behav 17: 13-23.
- Samoluk SB, Stewart SH (1998) Anxiety sensitivity and situation-specific drinking. J Anxiety Disord 12: 407-419.
- Dick DM, Smith G, Olausson P, Mitchell SH, Leeman RF, et al. (2010) Understanding the construct of impulsivity and its relationship to alcohol use disorders. Addict Biol 15: 217-226.
- Cox BJ, Swinson RP, Shulman ID, Kuch K, Reichman JT (1993) Gender effects and alcohol use in panic disorder with agoraphobia. Behav Res Ther 31: 413-416.
- Kushner MG, Abrams K, Borchardt C (2000) The relationship between anxiety disorders and alcohol use disorders: a review of major perspectives and findings. Clin Psychol Rev 20: 149-171.
- Norton GR, Norton PJ, Cox BJ, Belik SL (2008) Panic spectrum disorders and substance use. In: Stewart SH, Conrod PJ, editors. Anxiety and substance use disorders: the vicious cycle of comorbidity. Springer: New York pp 81-89.
- Tamres LK, Janicki D, Helgeson VS (2002) Sex differences in coping behavior: a meta-analytic review and an examination of relative coping. Pers Soc Psychol Rev 6: 2-30.
- Cooper ML, Russell M, Skinner JB, Windle M (1992) Development and validation of a three-dimensional measure of drinking motives. Psychol Assess 4: 123-132.
- Arnett J (2005) The developmental context of substance use in emerging adulthood. J Drug Issues 35: 25-254.
- Zimmermann P, Wittchen HU, Hofler M, Pfister H, Kessler RC, et al. (2003) Primary anxiety disorders and the development of subsequent alcohol use disorders: a 4-year community study of adolescents and young adults. Psychol Med 33: 1211-1222.
- Watt M, Stewart SH, Birch C, Bernier D (2006) Brief CBT for high anxiety sensitivity decreases drinking problems, relief alcohol outcome expectancies, and conformity drinking motives: Evidence from a randomized controlled trial. J Ment Health 15: 683-695.
- Conrod PJ, Stewart SH, Pihl RO, Cote S, Fontaine V, et al. (2000) Efficacy of brief skills interventions that match different personality profiles of female substance abusers. Psychol Addict Behav 14: 231-242.
- Conrod PJ, Stewart SH, Comeau N, Maclean AM (2006) Efficacy of cognitive-behavioral interventions targeting personality risk factors for youth alcohol misuse. J Clin Chid Adolesc Psychol 35: 550-563.
- Smits JA, Berry AC, Rosenfield D, Powers MB, Behar E, et al. (2008) Reducing anxiety sensitivity with exercise. Depress Anxiety 25: 689-699.
- Broman-Fulks JJ, Berman ME, Rabian BA, Webster MJ (2004) Effects of aerobic exercise on anxiety sensitivity. Behav Res Ther 42: 125-136.
- Taylor S, Zvolensky MJ, Cox BJ, Deacon B, Heimberg RG, et al. (2007) Robust dimensions of anxiety sensitivity: development and initial validation of the Anxiety Sensitivity Index-3. Psychol Assess 19: 176-188.
- Johnston LD, O'Malley PM, Bachman JG (2000) Monitoring the future national survey results on drug use, 1975-1999. Volume II: College Students and Adults Ages 19-40.
- Neighbors C, Fossos N, Woods BA, Fabiano P, Sledge M, et al. (2007) Social anxiety as a moderator of the relationship between perceived norms and drinking. J Stud Alcohol Drugs 68: 91-96.