
Journal of Urology & Nephrology
Download PDF
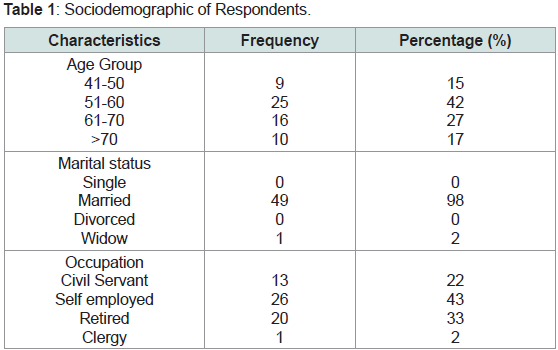 Table 1: Sociodemographic of Respondents.
Table 1: Sociodemographic of Respondents.
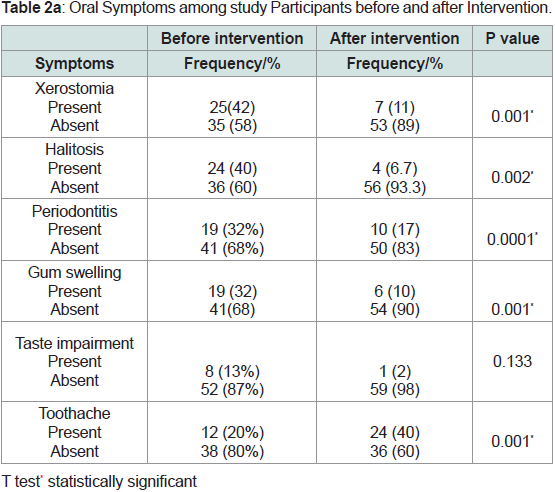 Table 2a: Oral Symptoms among study Participants before and after Intervention.
Table 2a: Oral Symptoms among study Participants before and after Intervention.
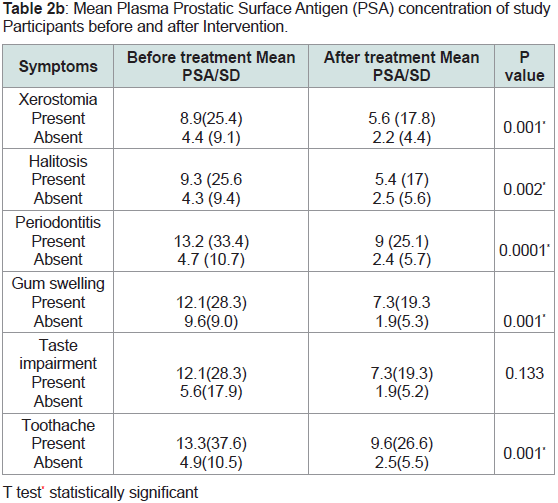 Table 2b: Mean Plasma Prostatic Surface Antigen (PSA) concentration of study
Participants before and after Intervention.
Table 2b: Mean Plasma Prostatic Surface Antigen (PSA) concentration of study
Participants before and after Intervention.
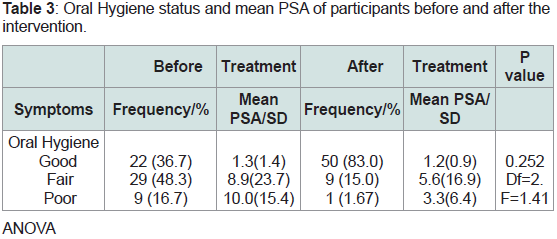 Table 3: Oral Hygiene status and mean PSA of participants before and after the
intervention.
Table 3: Oral Hygiene status and mean PSA of participants before and after the
intervention.
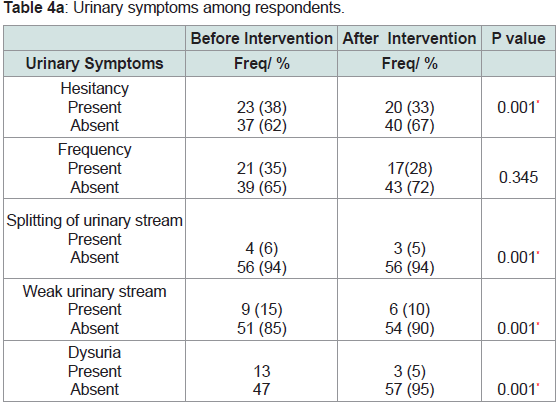 Table 4a: Urinary symptoms among respondents.
Table 4a: Urinary symptoms among respondents.
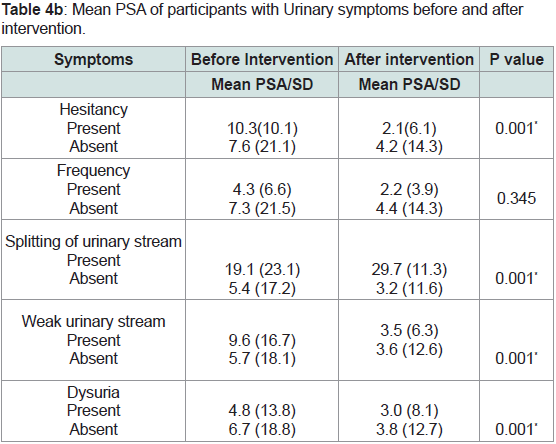 Table 4b: Mean PSA of participants with Urinary symptoms before and after
intervention.
Table 4b: Mean PSA of participants with Urinary symptoms before and after
intervention.
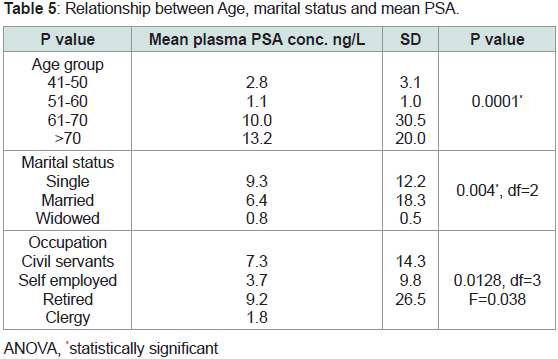 Table 5: Relationship between Age, marital status and mean PSA.
Table 5: Relationship between Age, marital status and mean PSA.
Research Article
The Influence of Oral Health Care on Prevalence of Urinary Symptoms and mean plasma Prostatic Surface Antigen (PSA) concentration in a Population of Nigerian Adult Males
Oyetola EO1*, Afolabi JB2 and Adedeji TA3
1Department of Oral Medicine and Oral Pathology, Obafemi
Awolowo University, Ile Ife, Nigeria
2Department of Child Dental Health, Obafemi Awolowo University,
Ile Ife, Nigeria
3Department of Chemical Pathology, Obafemi Awolowo University,
Ile Ife, Nigeria
*Address for Correspondence: Oyetola EO, Department of Oral Medicine and Oral Pathology,
Obafemi Awolowo University, Ile Ife, Nigeria; E-mail:
phemyhoye12@yahoo.com
Submission: 20 February, 2023
Accepted: 24 March, 2023
Published: 27 March, 2023
Copyright: © 2023 Oyetola EO, et al. This is an open access
article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is
properly cited.
Abstract
Background/Aims and Objectives:
Inflammatory mediators from
ongoing oral infection induce intense immune response that could
lead to the carcinogenesis as well as progression of pathogenesis of
systemic diseases. Development of prostatic carcinoma and presence
of urinary symptoms may be linked to the presence of oral problems.
Methodology:
This is a community based study with longitudinal
study design. The study was done among adult and elderly men in a
south western city in Nigeria (Oshogbo). Participants were randomly
selected from the community using systematic sampling technique.
Their biodata, history of oral and urinary symptoms were recorded. Oral
examination was done, blood samples of participants were collected
and transported to the laboratory for determination of mean plasma
PSA. Oral health education and corresponding treatment of oral
lesions present were done. Prostatic Surface Antigen was measured
in the laboratory using i-chroma Reader, a fluorescence scanning
instrument. Data was analyzed using STATA 16.
Results:
Out of the 72 participants that were recruited for the study,
only 60 participants completed the study, others were lost to follow up
and death. More than half of the participants are in their fifth decade
of life. The most prevalent the oral lesions seen was xerostomia, other
lesion seen were halitosis, candidiasis and periodontitis. The prevalence
oral lesions were significantly reduced after dental intervention.
The mean PSA concentration was highest among participants with
periodontitis, followed by those with split urinary stream. The mean
PSA concentration was also significantly reduced after the dental
intervention. Likewise, urinary symptoms were significantly reduced
after dental intervention, p= 0.001.
Conclusion:
Poor oral hygiene and presence of oral lesions are
associated with raised PSA concentration. Oral health education and
dental treatment were associated with reduced prevalence of oral
and urinary symptoms among males. Mean PSA is highest among
patients with periodontitis. Following dental intervention, mean
PSA concentration and the prevalence of urinary symptoms were
significantly reduced.
Keywords
Oral health care; Oral hygiene; Prostatic surface antigen
(PSA)
Introduction
Prostate cancer is second to lung cancer as the commonest
cause of cancer related cause of death among men worldwide and is
associated with high economic burden, high morbidity and mortality
[1,2]. Prostatic problems present in three major ways: prostate cancer
(PC), benign prostate swelling (benign prostatic hyperplasia, BPH)
and prostatitis. Prostate cancer patients present with constitutional
cancer symptoms as well lower urinary tract obstructive symptoms. There is no evidence yet on how to prevent production of prostate
cancer, but it is possible to reduce the risk by limiting high fat diets,
increase vegetables intake, good exercise, encourage healthy lifestyle
and good control of oral and general health conditions that may lead
to chronic inflammation [3].
Oral health care has been closely linked to prostatic cancer [4].
Chronic inflammation from the oral tissues has been implicated in the
initiation, promotion, and malignant transformation, invasion and
metaplasia in the pathogenesis of prostate cancer [3,5]. Periodontal
disease, an oral problem associated with chronic inflammation of
tooth supporting structures affects about half of the population and is
more prevalent among elders. The diseases are results from reduced
oral health care, presence of poor oral hygiene and influence of local
and systemic condition. Several chronic inflammatory mediators are
released during the pathogenesis of chronic periodontitis and these
compounds can initiate systemic inflammation especially when
there is impaired immunity which is not uncommon as age increases
[5]. Xerostomia and subjective feeling of oral dryness predispose to
chronic mucosa infection because of the lack of anti inflammatory
action of saliva. Patients with xerostomia will hence be predisposed to
chronic mucosa inflammation, dental caries, oral candidiasis among
others; these oral problems release chronic inflammatory products
into the system especially when there are underlying medical
problems [6]. Halitosis, defined as offensive mouth odour, is usually
caused by oral pathology is mostly due to inflammatory processes in
the mouth such as gingival abscess, poor OH, mucositis, tonsillitis
and so on.
Therefore, treating oral lesions reduces the burden of chronic
inflammation, and hence reduce the possibility of initiating the
process of carcinogenesis in prostatic glands studies has shown
specifically that periodontitis is associated with prostatic cancer.
PSA is a serine protein enzyme produced by columnar epithelium
of the prostatic tissue. It is produced by both normal and malignant
cells of the prostate glands. The protein is mostly found in semen but
a small percentage may be found in blood. The chance of developing
cancer goes up as the value goes up. No specific cut off beyond which
cancer will be developed, but generally when the values are more
than 4ng per ml in the blood, the patients are advised to go for PC
screening. PSA is therefore used for screening although it’s essentially
a pointer to the presence of PC and not affirmative.
Although there are scientific reports linking periodontal disease
with PC but there is scarcity of information in African population
where the prevalence of PC is on the increase. More so, there is need
to explore the association between other oral lesions and PSA so as
to discover the possible effects of treating the oral lesions on the PSA
concentration. these are the areas this study is designed to critically
explore. The rising prevalence of PC, increasing associated morbidity
and mortality and lack of information on the roles of oral lesions on
PSA concentration calls for this kind of study. Data from this study
will provide information that will further intensify the need to educate
PC patients on the importance of oral care, needs to be familiar with
self help screening indicators so that the population can be educated
and our patients progress can be monitored, hence this study.
MATERIALS AND METHODS
Study design:
This is a longitudinal study showing the relationship
between the serum PSA concentration, urinary symptoms and oral
lesions among adult men before and after oral health intervention.
Study location:
The study was conducted Ataoja Estate, Oshogbo,
Osun state, Nigeria. Oshogbo is the capital of Osun State, Nigeria. The
surface area of the city is 47km2 with a population of 395,500 people.
Data analysis was done at Chemical pathology laboratory, Obafemi
Awolowo University Teaching Hospitals Complex, Ile Ife, Nigeria.
Subjects:
Study participants were adult men volunteers who
reside at Ataoja Estate, Oshogbo in Osun state, Nigeria.
Sampling technique:
Multistage sampling method was used
to select the sample. The first stage was the selection of one Local
Government from the two LG Areas in Oshogbo town. The two Local
Government (LG) Areas in Oshogbo Township are Oshogbo LG and
Olorunda LG, selection was done using by simple random sampling
method. A non transparent box that containing two wrapped papers,
one marked A (which stands for Oshogbo) and the other marked B
(stands for Olorunda) was prepared. One of the two papers was blindly
taken out of the box to select the LG, and that was found to be Osogbo
Local government (A). The second stage was the selection of streets/
estates from the LG. There are six major Street/Estates in Oshogbo
Local government. One of the six streets was also selected using
simple random method with wrapped papers in a non transparent
box, and the selected Street was Ataoja Estate. All consenting adult
men in Ataoja Estate, Oshogbo that satisfied inclusion criteria were
recruited for this study.
Inclusion criteria:
• Adult men > 40 years old
• Apparently healthy men with no sign of prostatic
inflammation, prostate cancer or prostate enlargement
• Men who had not ejaculated in the last 24 hours
• Men who have not got involved in rigorous exercise like
cycling two days before the testing.
Exclusion criteria:
• Presence of debilitating underlying systemic condition such
as hypertension, diabetes and prostatic cancer
• Men with enlarged prostatic gland
Ethical Consideration:
Permission to carry out the study was
sought and obtained from the Ethical Committee of the Institution.
Each participant also gave their consent before recruitment into the
study. Patients’ information was handled with respect and utmost
confidentiality.
Clinical Data Collection:
Data collection was done using
structured questionnaires which were administered by the researcher
to the participants after obtaining their consent.
The first part of the questionnaire (Section 1) collects information
about participants’ biodata such as name, age, gender, address,
ethnicity, marital status, and present occupation. In section two,
patients’ medical and dental history, as well as presence of urinary
and oral symptoms was recorded.
Sections 3 records clinical oral findings. Patients were made to sit
down comfortably on consulting chair. The presence or the absence of
halitosis was assessed by using organoleptic method. Gingival status
was assessed using gingival index Loe and Silness [7]. Generally,
periodontologist have reported that a tooth is said to have developed
periodontitis when there is associated established pocket of more
than 3 mm depth. For the purpose of this study, teeth with established
pocket more than 3 mm were taken as having periodontitis. Halitosis
was diagnosed based on patients’ subjective feeling of oral dryness,
and any presence of at least one of the following signs: loss of shinning
appearance of the oral mucosa, presence of ropy saliva, loss of salivary
bubbles at the floor of the mouth and reduced saliva flow following
external stimulation of parotid gland.
The Section 4 of the questionnaire records the findings of rectal
examination and the serum prostatic surface antigen (PSA). Patients
with enlarged prostate glands were excluded from the study. Blood
samples were collected using 18 inch gauge hypodermic needle
and were transported to the laboratory for storage at -10°C prior to
analysis.
LABORATORY PROCEDURE:
PSA assay was done at the Point-of-Care Testing (POCT) facility
of at Obafemi Awolowo Teaching Hospitals’ Complex, Ile Ife. The
PSA in the serum was measured using an i-chroma reader which
is a fluorescence scanning instrument, used in conjunction with
various ichroma Immunoassay Tests which are based on antigenantibody
reaction and fluorescence technology. The i-chroma Reader
employs a semiconductor diode laser as the excitation light source
for illuminating the test cartridge membrane (pre-loaded with the
clinical specimen, duly processed according to standard procedure prescribed by the manufacturer-Boditech Med Inc., Germany).
The laser triggers fluorescence from the fluorochrome molecules
embedded on a membrane. The fluorescent light is collected together
with the scattered laser light. Pure fluorescence is filtered from
the mixture of the scattered and fluoresced light. Intensity of the
fluorescence is scanned and converted into an electric signal which
is proportional to the intensity of fluorescence produced on the test
cartridge membrane.
The assay was performed using manufacturer’s instruction as
reported by Luisa et al [8]. 75microgram of serum was mixed with the
supplied pre-measured volume of detector buffer solution containing
fluorescence labeled anti PSA monoclonal antibody and anti rabit IgG.
Thereafter, 75microgram of the resulting mixture was then loaded
into the sample well of a test strip in the machine and cartridge was
incubated at room temperature for 15 minutes. The concentration of
PSA in the sample is directly correlated to the intensity of the scanned
fluoresce reaction which is converted electric into signal that can be
read on the screen of the reader in nanogram per litre.
Treatment interventions:
Health Education: After oral examinations, all patients were
given oral health education and motivation. They were taught tooth
brushing techniques, use of dental floss, diets for maintaining good
oral health, and general skills on how to recognize and provide home
care for common oral problems.
Scaling and Polishing:
All participants were conveyed to the
dental clinic of Obafemi Awolowo University, Ile Ife where scaling
and polishing was done for each of them using Ultrasonic Scaler.
Treatment of Specific Oral Problems:
Specific treatment were
also given to those with oral problems Xerostomia was treated with,
frequent oral sips of water; regular oral sips of water and regular lime
water oral rinse Halitosis- Scaling and polishing, warm saline mouth
bath and referral to periodontologist Candidiasis- Nystatin lozenges
(pastilles) three times daily.
Gingivitis- Scaling and polishing, WSMS and Chlorhexidine
mouth wash
Review:
Daily contacts were made via telephone calls about the
symptoms. Patients were reviewed 4 weeks in the clinic after the first
contact during which oral and urinary symptoms were re evaluated
as well as serum PSA.
Data Analysis:
Data were analyzed using STATA 16 statistical
software (StataCorp, College Station, Texas). Percentages and
proportion were used to describe qualitative variables such as the
distribution of participants with specific oral and dental problem, sex,
ethnicity, occupation and marital status. For continuous variables
such as age and PSA concentration measures of central variables like
mean, median, mode, and range were used for analysis. Comparison
of mean PSA before and after intervention was done after subjecting
the variable to normality tests, since the PSA was not normally
distributed, Mann–Whitney rank sum test and Kruskal-Wallis test
were used for to determine the relationship between mean PSA
before and after intervention, and at various age groups. Statistical
significance will be set at p <0.05.
Results
A total of 72 adult males were recruited for the study, 10
participants were lost due to follow up as a results of relocation and
inability to continue to participate due to impaired health condition.
Also, we lost 2 participants to death during the study period. So,
complete data of only 60 participants were obtained for data analysis.
Sociodemographic of Respondents:
Participants were all adult and elderly males. About half were
in their fifth decade of life. Majority were married with only 1 (2%)
widowed. None was completely dependent and the commonest
occupation was self-employed (21, 42%) (Table 1).
Oral Symptoms among study Participants before and after Intervention:
The most frequent oral lesion seen among study participants
before intervention was xerostomia. Xerostomia was present in one
out of every four participants. Other frequent oral lesions/symptoms
seen before intervention were periodontitis (68%), gum swelling
(32%) and toothache (20%). After dental intervention, the proportion
of participants with xerostomia, periodontitis, gum swelling and
toothache was significantly reduced to 11%, 6.7%, 10% and 40%
respectively Table 2a.
Mean Plasma Prostatic Surface Antigen (PSA) concentration of study Participants before and after Intervention:
Mean plasma PSA of participants was significantly higher
among patients with oral lesions when compared to those without
oral lesions. The highest value was seen among participants with
periodontitis and lowest among patients with halitosis. Statistically
significant reduction was seen in the mean plasma PSA concentration
after dental intervention (Table 2b).
Oral Hygiene status and mean PSA of participants before and after the intervention:
Before dental intervention, more than three out of four
participants presented with either fair oral or poor hygiene status.
After the intervention, the proportion of those with good oral hygiene
increased to 83%% while those with poor oral hygiene significantly
reduced to 1.7%. The lowest mean PSA before intervention was
found among those with good oral hygiene and the highest was found
among those with poor oral hygiene. After the treatment, those with
good oral hygiene still have the lowest PSA while the highest value
was found among those with fair oral hygiene (Table 3).
Urinary symptoms among respondents before and after intervention:
Hesitancy (23, 38%) was the most frequent urinary symptom
observed among the participants before intervention, followed by
frequency (19, 38), Dysuria and weak urinary stream (9, 15). Splitting
of urinary stream was the lowest urinary symptom, present in 7 (14%)
participants. After intervention, significant reduction of urinary
symptoms was observed (Table 4a).
Mean PSA of participants with Urinary symptoms before and after intervention:
Participants with split urinary symptoms have the highest mean
PSA, followed by those with hesitancy and weak urinary stream. After
the intervention, the mean PSA was significantly reduced in patients
with all the reported urinary symptoms (Table 4b)
Relationship between Age, Marital status, Occupation and mean PSA of participants:
Mean PSA is highest among participants older than 70 years and
is lowest among those in their seventh decade of life. The differences
of mean PSA among age group is statistically significant, p=0.0001.
Single participants have the highest mean PSA followed by widowed
participants. The differences were statistically significant, p=0.004.
Mean PSA was highest among retired participants, and lowest among
clergy, the differences were not statistically significant, p=0.0128
Table 5.
Discussion
This study was conducted among male Nigerian population to
explore the relationship between oral health and the mean plasma
PSA concentrations, and to show the effects of dental intervention
on prevalence of oral lesions, urinary symptoms and mean PSA
concentration. The most frequent oral lesion seen in this study was
xerostomia, present in 35% of partcipants. This finding is in agreement
with a Swedish study by Anna Adolfsson et al [9]. Nederfors et al
also reported 28.4% that reported prevalence of 35.2% and 28.4%
respectively among male respondents [10]. A lower prevalence of
(11.1%), however, was reported in Iraq [11]. In additioon to gender,
the prevalence of xerostomia also varies with age, medication use
and the presence of underlying medical problems [10]. Xerostomia
has been attributed to loss of connective tissue cells, acinar cell
reduction, influence of drugs and chronic stress [12,13]. In addition,
men are largely exposed to stress as they struggle to meet their daily
family needs, chronic stress is an idicator of xerostomia. Stress is a
common feature associated with men in African population as it was
obvious in our study Participants [14]. Halitosis is another frequent
oral lesion which was present in 24 (40%) of the partcipants. Halitosis
is attributable to high prevalence of xerostimia, poor oral hygiene
and loss of mucular control for effective tooth brushing which were
seen among the partcipants [15]. Inflammation of periodontal tissues
(periodontitis) is another frequent finding among our participants.
This is due to often neglected oral care, poor oral hygiene and effects
of underlying systemic problems. The presence of periodontitis has
been associated with increased PSA, predisposing the patients to
develop PC.
The mean PSA among unmarried men in this study was 9.4ng/
mL which is significantlly higher than the value for the married
(6.3ng/mL). This finding is consistent with the report of Khan S et al
and Siegel et al [16,17]. Lower values of mean PSA among the married
may be due to the positive effects of sexual exposure on the health
of prostate gland, and due to the vast social support received from
their spouses [16]. Unlike singles, widows and divorcees, married
men are known to show reduced chance of developing PC and a low
incidence of resulting complications [16].
Chronic oral infections have been reported to be closely associated
with increased risk of deveping PC [4]. In this study, partcipants
with good oral hygiene has the lowest mean PSA before dental intervention, and after the dental intervention, the value further
reduces by 100%. Plaque produces bacteria and fungi infections
which has been reported to shows bi directional relationship wiuth
propstatic cancer. The resulting chronic inflammation tends to
increase the PSA production, and subsequently developing of PC,
although the mechanism of cation is still largely unclear [18]. The
fact that significant reduction of mean PSA was observed after dental
intervention is an indication that the presence of dental plaque may
serve as source of irritation that may produce immune response that
may trigger carcinigenesis. Those with poor oral hygiene has the
lowest PSA, even lower than those with poor oral hygiene, at the peak
of inflammatory response ,in addition; periodontopathogenic insult
may not produce additional increase in PSA.
Recent studies have explored the correlation between
periodontitis and PSA levels. Huang et.al revealed that serum PSA
levels in men with periodontitis were not higher after accounting
for age and other factors in a middle-aged and older population in
America. However, Joshi et.al found that PSA levels were higher in
individual in individual with CAL ≥ 2.7mm and moderate/severe
prostatitis than in patients with neither condition. If mean PSA
levels increase with the severity of periodontitis or if periodontal
treatment reduces PSA, we would infer a positive correlation between
periodontitis and PC risk. This is similar to the findings in our study
which showed that PSA levels in individuals with periodontitis were
significantly higher than those in men without periodontitis but did
not correlate significantly with the severity of periodontitits, though
in varaition with another study by Michaud et al. that in PSA-based
PC screening in a US population, periodontitis did not correlate with
PC risk. Overall, the mechanism of periodontitis and elevated PSA
level remains unclear. In the presence of inflammation, the integrity
of the prostate epithelium might be compromised causing more PSA
to leak into the blood. Morote et al.showed that another non-prostatic
source of PSA, such as periodontium, might increase its levels.
Presence of xerostimia also showed significant association with
mean PSA is xerostomia. Mean PSA of patients with xerostomia
reported in this study is 8.9ng/mL, this is above the threshold level
of developing PC [18]. Presence of xerostomia are has linked with
proliferation of oral infection due to the absence of the antiinammatory
functions of saliva. Saliva contains immune subtances that can
reduce inflammatory response and stabilize the rate of proliferation
of chronic infection. Some of the chronic infections that can result
from xerostomia are periodontitis, mucositis, tonsillitis, dental cares,
candidiasis e.t.c [13]. These are oral infections which can be associated
with intense immune response, and that can lead to carcinogenesis.
As shown in this study, treatment of xerostomia leads to the significant
reduction of mean PSA. Good oral health care has been reported to
reduce the risk of developing PC [18].
Generally, the prevalence of lower urinary symptoms increases
with increasing age [19]. Common lower urinary symprms seen
in this study include hesitances, frequency, splitting of urinary
stream, dysuria and difficulty in passing urine. Hesitances was the
lower urinary symptoms, seen in 35% of partcicipants, followed by
frequency (36%) and dysuria (15%). According to Serlin et al, benign
prostatic enlargement is the commonest cause of obstructive urinary
symtpoms among adult males, resposnible for 58% of the cases [20]. The significant reduction of the prevalence of urinary symptoms after
dental treatmemt observed in this study. This finding is in agreement
with Oyetola et al that reported positive relationship between good
oral health and renal sytmpoms in an African population [21]. Oral
pathogens induce chronic inflammation which play vital roles in
the pathogenesis of the urinary diseases and formation of PSA. As
reported in this study, mean PSA was seen to be highest among those
with hesitancy (10.3ng/mL) and frequency (4.4ng/L). The values were
also significantly reduced after the dental intervention in agreement
with the findings by Mao et all that showed significant reduction in
mean PSA in patients without periodontitis compared to those with
periodontitis [18].
The presense of oral chronic inflammatory diseases such as
chronic periodontitis has been reported to be associated with
high plasma PSA concentration and to exhibit potential roles in
pathogenesis of carcinigenssis [18]. Therefore, as reccomemdened
from earlier studies [21,22], routine dental consultations and
accompanied dental interventions will not only relieve the oral
symptoms, but are also advantageous in the management of adult
men that are at risk of developing prostatic carcinoma. This becomes
necessary in developing countries where there are limited resources to
manage prostatic cancers and the associated complications.
Conclusion
This results of this study showed that the presence of poor oral
hygiene, presence of oral lesions (such as periodontitis, halitosis
and xerostomia), and presence of urinary symptoms (such as
splitting urinary symptoms, dysuria and frequency) are associated
with significantly raised PSA concentration. We also conclude that
prompt oral health education, routing scaling and polishing and
prompt treatment of oral lesions tends to reduce the mean PSA as
well as the prevalence of urinary symptoms among adult males. Mean
PSA is highest among patients with periodontitis. Following dental
intervention, mean PSA concentration and the prevalence of urinary
symptoms were significantly reduced.
References
Citation
Oyetola EO, Afolabi JB, Adedeji TA. The Influence of Oral Health Care on Prevalence of Urinary Symptoms and mean plasma Prostatic
Surface Antigen (PSA) concentration in a Population of Nigerian Adult Males. J Urol Nephrol. 2023;10(1): 6.