
Journal of Urology & Nephrology
Download PDF
 where, K = 7.9, μ1 = 27, μ1 = 23, and S = 6.1
where, K = 7.9, μ1 = 27, μ1 = 23, and S = 6.1
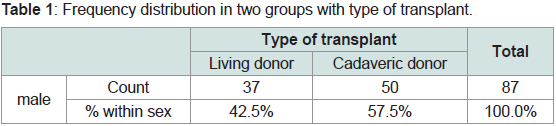 Table 1: Frequency distribution in two groups with type of transplant.
Table 1: Frequency distribution in two groups with type of transplant.
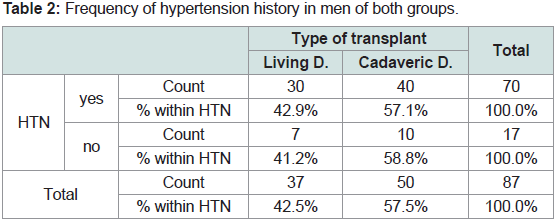 Table 2: Frequency of hypertension history in men of both groups.
Table 2: Frequency of hypertension history in men of both groups.
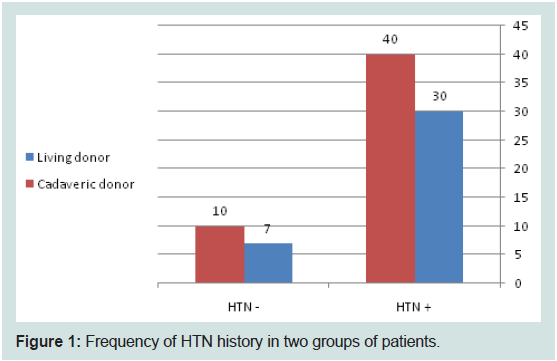 Figure 1: Frequency of HTN history in two groups of patients.
Figure 1: Frequency of HTN history in two groups of patients.
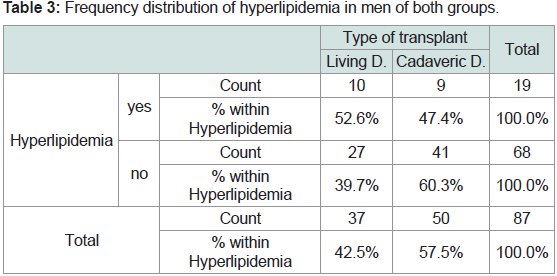 Table 3: Frequency distribution of hyperlipidemia in men of both groups.
Table 3: Frequency distribution of hyperlipidemia in men of both groups.
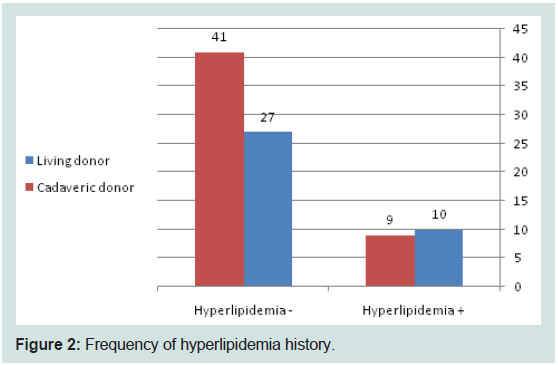 Figure 2: Frequency of hyperlipidemia history.
Figure 2: Frequency of hyperlipidemia history.
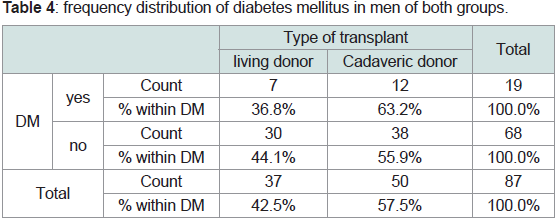 Table 4: Frequency distribution of diabetes mellitus in men of both groups.
Table 4: Frequency distribution of diabetes mellitus in men of both groups.
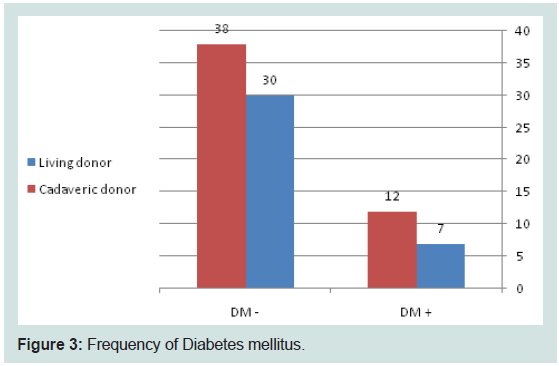 Figure 3: Frequency of Diabetes mellitus.
Figure 3: Frequency of Diabetes mellitus.
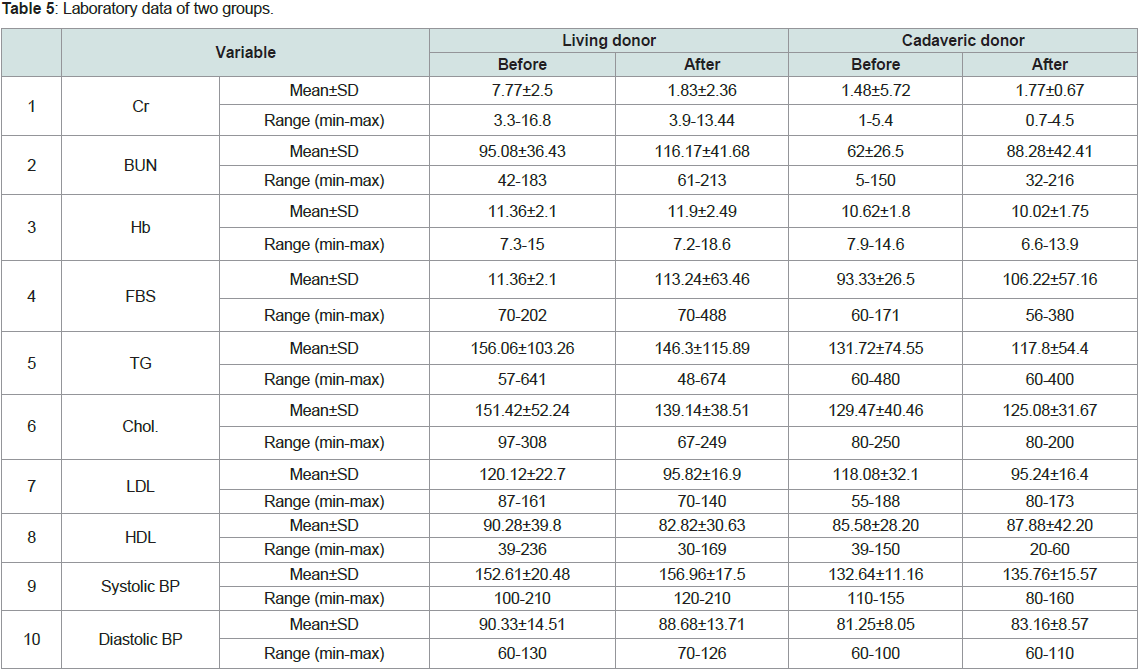 Table 5: Laboratory data of two groups.
Table 5: Laboratory data of two groups.
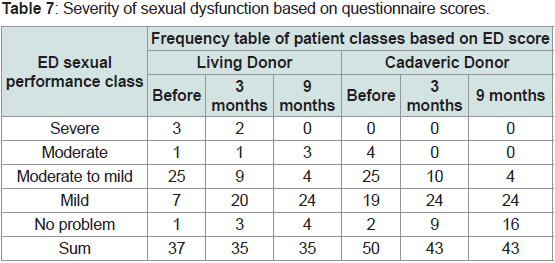 Table 6: sexual dysfunction of men in both groups in three occasions.
Table 6: sexual dysfunction of men in both groups in three occasions.
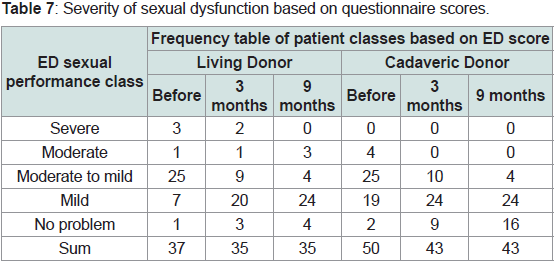 Table 7: Severity of sexual dysfunction based on questionnaire scores.
Table 7: Severity of sexual dysfunction based on questionnaire scores.
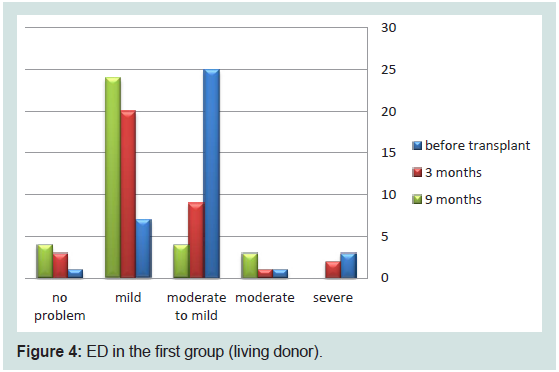 Figure 4: ED in the first group (living donor).
Figure 4: ED in the first group (living donor).
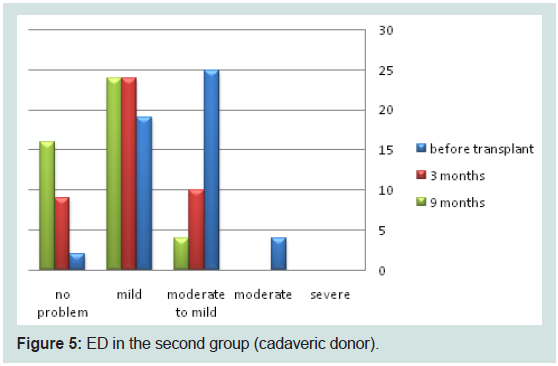 Figure 5: ED in the second group (cadaveric donor).
Figure 5: ED in the second group (cadaveric donor).
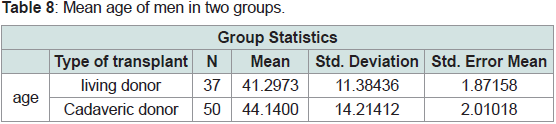 Table 8: Mean age of men in two groups.
Table 8: Mean age of men in two groups.
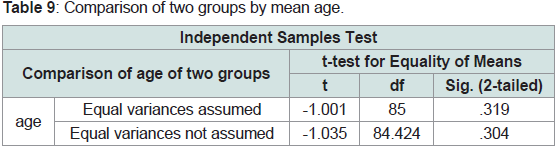 Table 9: Comparison of two groups by mean age.
Table 9: Comparison of two groups by mean age.
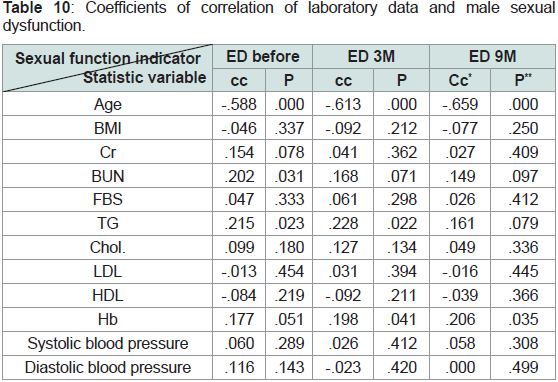 Table 10: Coefficients of correlation of laboratory data and male sexual
dysfunction.
Table 10: Coefficients of correlation of laboratory data and male sexual
dysfunction.
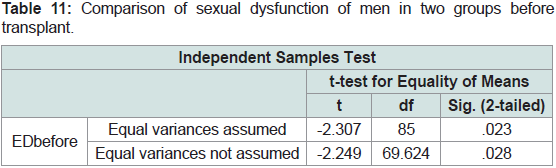 Table 11: Comparison of sexual dysfunction of men in two groups before
transplant.
Table 11: Comparison of sexual dysfunction of men in two groups before
transplant.
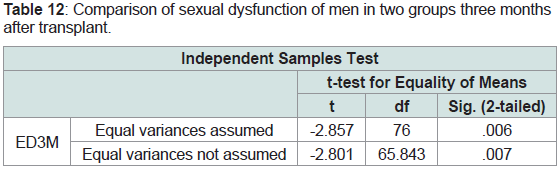 Table 12: Comparison of sexual dysfunction of men in two groups three months
after transplant.
Table 12: Comparison of sexual dysfunction of men in two groups three months
after transplant.
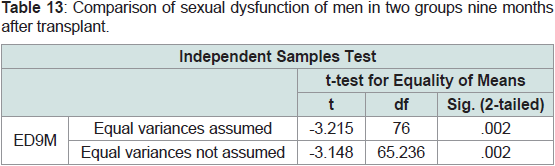 Table 13: Comparison of sexual dysfunction of men in two groups nine months
after transplant.
Table 13: Comparison of sexual dysfunction of men in two groups nine months
after transplant.
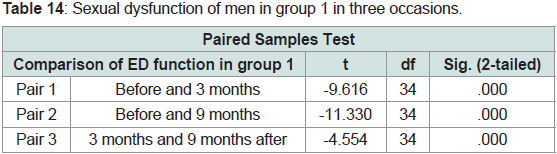 Table 14: Sexual dysfunction of men in group 1 in three occasions.
Table 14: Sexual dysfunction of men in group 1 in three occasions.
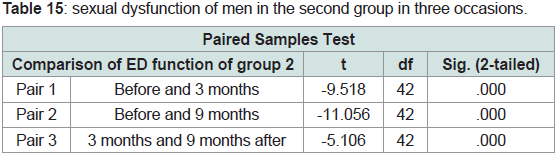 Table 15: Sexual dysfunction of men in the second group in three occasions.
Table 15: Sexual dysfunction of men in the second group in three occasions.
Perspective
Comparison of Sexual Function Changes between Two Groups of Male Kidney Recipients from Living Donor and Cadaveric Donor
Behtash N* and Nikoobakht MR
Sina Hospital, Tehran University of Medical Sciences, Iran
*Address for Correspondence: Behtash N, Sina Hospital, Tehran University of Medical
Sciences, Iran; E-mail: negarbehtash@gmail.com
Submission: 19 September 2022
Accepted: 17 October 2022
Published: 20 October 2022
Copyright: © 2022 Behtash N, et al. This is an open access
article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is
properly cited.
Abstract
Due to high incidence of kidney failure and ESRD cases, the need
for better and more effective treatments increases to increase life
span of patients and their quality of life. One of the useful treatment
methods in patients with severe renal failure is kidney transplantation,
which is performed in two ways: transplantation from a living donor and
transplantation from a cadaveric donor. Considering that almost most
patients with kidney failure who are candidates for kidney transplant
surgery are young or middle-aged, one of the most important
factors affecting their satisfaction with the course of treatment and
quality of life is sexual ability and performance. All the patients who
underwent kidney transplant from living donor or cadaveric donor
from 5/22/2015to 5/22/2015in Sina Hospital constituted the statistical
population of this study. Sampling in this study is simple sampling
and the method used to collect the required data and information
is questionnaire. Independent variables investigated in this study,
which are related to kidney transplant as well as various parameters
of sexual performance of the patients, were collected and recorded
separately according to the approved model of IIEF-15 questionnaire
in Iran for male patients. The data was statistically analyzed by SPSS
software, version 16. Frequency and frequency percentage are used
to describe the qualitative data, and mean and standard deviation
are used to describe the quantitative data collected. Qualitative
variables were analyzed using chi-square test and quantitative
variables were analyzed using t-test. Based on the results obtained,
sexual function of patients improved after transplantation from a living
donor in both groups. Although in the comparison between the two
groups, cadaveric donor patients show better conditions than living
donor patients at all times in factors related to sexual performance,
the difference between the two groups is not statistically significant
in terms of variables related to sexual performance, except for desire.
Keywords
Kidney transplant; Sexual dysfunction; IIEF-5 questionnaire
Introduction
Considering the significant progress of human knowledge in
the field of identifying efficient treatment methods in treatment of
kidney failure, the number of people suffering from this disease who
continue their lives with the help of kidney transplant is increasing.
Currently, a transplanted organ is received in two ways: receiving an
organ from a living donor or receiving an organ from a cadaveric
donor. Despite the increasing number of organ transplants, especially
kidney transplants, there have not been enough studies to compare
or confirm the superiority of one of these two methods. Problems
related to sexual dysfunction are common problems of patients
with kidney failure, which are usually not given enough attention.
A variety of sexual disorders and fertility problems are seen in men
and women with kidney failure, including erectile dysfunction in
men, decreased libido, lack of ovulation, menstrual disorders and
infertility in women [1,2,3]. Pathogenesis of sexual dysfunction in
uremic patients is attributed to hormonal imbalance, vascular and
neurological disorders, drugs and psychological problems [4,5].
Some studies have claimed that more than 50% of men with
kidney failure experience erectile dysfunction during their illness
[6]. There are also evidences of improvement in erectile function of
patients with kidney failure who were undergoing haemodialysis after
kidney transplant, and this improvement rate was higher in patients
who were transplanted at a younger age [7]. ROSAS et al (2001)
estimated the prevalence of erectile dysfunction in haemodialysis
patients at 82% [8]. As noted, sexual dysfunction in CRF patients
is not exclusive to men and can also be seen in affected women.
Menstrual disorders, amenorrhea and subsequent fertility disorders
are among the problems that these patients experience [9]. Toorian
et al (1997) and Kettas et al (2008) in similar studies reported the
prevalence of sexual dysfunction as 90% before dialysis and 60-70%
after dialysis [10,11]. In a study conducted by Rebecca J Muehrer et
al. (2009) at the University of Wisconsin, improvement of sexual
function after kidney transplant and its impact on quality of life of
patients were investigated and significant changes were reported. In
addition, this study emphasized that an underlying disease leading
to kidney failure can also be the cause of sexual dysfunction in these
patients, and sometimes, due to inability to resolve the underlying
cause, a significant improvement in sexual function may not be seen
in a number of patients [12]. Among the common diseases that can
lead to kidney failure, we can mention diabetes and hypertension,
which can cause sexual dysfunction with the mechanism of vascular
disorder and neuropathy. Controlling blood glucose and blood
pressure in these patients will help improve sexual performance.
Although the damage caused by these diseases will remain permanent
in some cases [13].
Among the other theories proposed for erectile dysfunction
in men with CRF, we can mention penile venous insufficiency.
Anastomosis of transplanted renal artery is usually done as end
to end internal iliac artery or end to side external iliac artery. The
risk of venous insufficiency leading to sexual dysfunction in men
with kidney failure transplanted in end-to-end internal iliac artery
anastomosis is 10%; in case of a second transplant and internal iliac
artery anastomosis on the opposite side, this risk is reported as 25-
65% [7,13]. Unlike the studies reviewed so far, other studies have also been conducted, the results of which indicate that kidney transplant
cannot always have a positive effect on improving sexual performance
of patients [2,16]. Considering that most cases of kidney transplant
are performed in middle-aged patients and taking into account the
age of sexual activity of patients, sexual dysfunction is one of the
important issues in the lives of these people, which may not have been
addressed well and necessary measures for treatment have not been
taken due to cultural issues [3]. On the other hand, as we know little
about sexual disorders of women with transplanted kidney failure
or undergoing dialysis, it seems necessary to compare the changes
in sexual function of kidney transplant recipients between two
groups of kidney recipients from living donors and cadaveric donors.
Therefore, this study, while evaluating sexual ability and performance
of kidney transplant patients, tends to compare the changes in sexual
performance of patients who received a kidney from a living donor
with those who received a kidney from a cadaveric donor.
Material & Methods
This project is a cohort study that was done prospectively and
without blinding.
Population, Sample Size and Calculation:
All the patients who underwent kidney transplant from living
donor or cadaveric donor from 5/22/2015 to 5/22/2015 in Sina
Hospital constituted the statistical population of this study. Reference
articles and similar texts were used to determine the sample size. In
this way, if the first type error is equal to 1% and the study power is
81%, in the null hypothesis where the mean of both groups is equal
to 0.27 and in the alternative hypothesis with estimated standard
deviation equal to 6 in both groups and considering the significance
level (α) equal to 0.05 using two-sided/two-sample t-test, we need 37
people in each group. The formula used to calculate sample size is:
Inclusion and Exclusion Criteria:
All patients who received a kidney transplant from both living and
cadaveric donors at Sina Hospital from 5/22/2015 to 5/22/2015were
examined in this project. Patients with the following conditions were
included in the study. It should be noted that exclusion criterion is
not defined for patients due to retrospective nature of the study and
simple sampling.
➢ Patients with appropriate age for sexual activity
➢ Patients with a history of at least 6 months of dialysis before
kidney transplant
➢ Patients with creatinine levels less than 2 after kidney
transplant
Sampling in this study was simple sampling. Due to the
prospective nature of the study, patients who met the inclusion criteria
were included in the study. According to the type of transplanted
kidney donor, the participants were divided into two groups: kidney
recipients from a living donor and kidney recipients from a cadaveric
donor. Blinding has no place in implementation process of this study.
Data Collection Method:
The method used in this study to collect the required data and
information is to complete the questionnaire. An information form
or questionnaire was considered for each patient, which contains
complete personal information of kidney transplant patients.
The independent variables investigated in this study, which are
related to kidney transplant, as well as various parameters of sexual
performance of the patients, were collected and recorded separately
according to the approved model of IIEF-15 questionnaire in Iran for
male patients.
Data Analysis Method:
After finishing the sampling and computerizing the data, the data
was statistically analyzed by SPSS software, version 16.Frequency
and frequency percentage are used to describe the qualitative data of
the study, and mean and standard deviation are used to describe the
quantitative data collected. According to the value of margin of effect,
non-inferiority comparison is made between two groups. Qualitative
variables are analyzed using chi-square test and quantitative variables
are analyzed by t-test (P<0.05).The significance level of all tests is
considered to be 95%.
Results
Due to the difference in the investigation method and the reported
results, a comparison was made between men of two groups, and for
ease of understanding and access; the results of the statistical analysis
are reported separately by group (Table 1).
Total number of male patients in two groups was 87; 37 patients
in group 1 (1 patient rejected and 1 patient died) with a mean age of
41.3 ± 11.38 (in the age range of 22-70 years) and 50 patients in group
2 (1 patient rejected and 6 patients died) with a mean age of 44.14 ±
14.21 (in the age range of 18-72 years).In group 1, the mean duration
of dialysis was 16.3 ± 11.28 months, the minimum duration of dialysis
was 6 months and the maximum was 48 months.In group 2, the men
duration of dialysis was 22.98 ± 19.15 months with a minimum range
of 6 months and a maximum of 108 months.In group 1, the mean
BMI of patients was 24.98 ± 3.77 kg/m2, the minimum of which was
16.50 kg/m2 and the maximum was 32.91 kg/m2. In group 2, the mean
of this index was 24.13 ± 4.22 kg/m2 with a minimum range of 15.90
kg/m2 and a maximum range of 35.46 kg/m2.
Thirty patients in the living donor group and 40 patients in the
cadaveric donor group had a history of hypertension. Statistical
analysis of hypertension history in the examined patients and
frequency chart of the two groups can be seen below (Table 2)
(Figure 1).
Ten patients in the living donor group and 9 patients in the
cadaveric donor group had a history of hyperlipidemia. Statistical
analysis of hyperlipidemia history in the examined patients and
the frequency chart of the two groups can be seen below (Table 3)
(Figure 2).
Seventeen patients in the living donor group and 29 patients in the
cadaveric donor group had a history of diabetes mellitus. Statistical
analysis of diabetes mellitus history in the examined patients and
the frequency chart of the two groups can be seen below (Table 4)
(Figure 3).
Laboratory findings, including creatinine, BUN, hemoglobin,
fasting blood glucose, triglyceride, cholesterol, LDL and HDL, were
examined in all patients. The results of examination of these variables,
separated by the two studied groups, can be seen in Table 5.It should
be noted that in group 1, there were two hepatitis B patients and no
hepatitis C patients were observed. In group 2, one hepatitis B patient
and one hepatitis C patient were observed (Table 5).
During this study, according to the approved questionnaire for
evaluation of sexual performance of men in Iran, various factors were
examined and reported. The results of descriptive analysis of the
factors related to sexual dysfunction of men, which were evaluated
three times before transplantation, 3 months after transplantation and
9 months after that and recorded by the patient in the questionnaire,
as well as severity score of sexual dysfunction is listed in the following
tables (Table 6,7) (Figure 4,5).
In the statistical analysis of the variables in two groups, first the
mean age of the two groups was examined. According to Table 8 and 9 there is no significant difference in mean age of male patients in the
two studied groups (P=0.319) and therefore the male patients in the
two groups have the same age distribution.
By performing multiple regression analysis, the relationship and
Pearson correlation coefficient between some laboratory indicators
and male sexual dysfunction before and after transplantation were
determined and reported.
According to the obtained P-values and correlation coefficients,
there is an inverse relationship between the age of male patients
and sexual performance before transplantation, 3 months later and
9 months later. There is a direct relationship between BUN and
triglyceride levels and sexual function before transplantation. Sexual
performance 3 months after transplantation has a direct relationship
with the level of triglycerides and hemoglobin. Nine months after transplantation, a direct relationship is seen between hemoglobin
and sexual dysfunction. In other cases, there was no significant
relationship (Table 10).
As the main objective of the study, sexual dysfunction of men in
two groups was compared on three occasions, before transplantation,
3 months after transplantation and 9 months later. In the pretransplant
period (P-value=0.028), there is a significant difference in
ED sexual performance between the two groups, and according to
the mean, men in the second group performed better. According to
P-value=0.006, there was a significant difference between the men of
the two groups in ED index at 3 months after transplantation, and
performance of group 2 was better. According to P-value=0.002, there
is a significant difference between ED sexual performance in men of
the two groups at 9 months after transplantation, and according to
the mean, the men of the second group performed better. Finally, it is
shown that the second group (cadaveric donor) compared to the first
group, performed better in all 3 occasions (Table 11,12).
In addition to intergroup comparison, sexual performance was
analyzed separately in each group, among male patients in the same
group, using the Paired Sample T-test, and was compared in three
occasions (Table 13).
According to Table 14, P-value shows that there is a significant
difference in all cases of ED sexual dysfunction comparison in the
group of living donor patients. Considering the increase of the
mean with the increase of time after transplantation, post-transplant
improvement of sexual function is evident.
According to Table 15, P-values show that there is a significant
difference in all cases of ED sexual dysfunction compared in the group of cadaveric donor patients. Considering the increase of the
mean with the increase of time after transplantation, post-transplant
improvement of sexual function is evident. Finally, the obtained
results show that ED sexual function improved after transplantation
in both groups. However, in the comparison between the two groups,
cadaveric donor patients show better conditions than living donor
patients at all times.
Discussion & Conclusion
Problems related to sexual dysfunction are common problems
of patients with kidney failure, which are usually not given enough
attention. Some studies have claimed that more than 50% of men with kidney failure experience erectile dysfunction during their illness
[6]. Considering the significant progress of human knowledge in
the field of identifying efficient treatment methods in treatment of
kidney failure, the number of people suffering from this disease who
continue their lives with the help of kidney transplant is increasing.
As most cases of kidney transplant are performed in middleaged
patients and taking into account the age of sexual activity of
patients, sexual dysfunction is one of the important issues in the
lives of these people, which may not have been addressed well and
necessary measures are not taken due to cultural issues [3]. This study
was designed and implemented to compare the changes in sexual
function between patients who received a kidney from a living donor
and those who received a kidney from a cadaveric donor. By using standardized questionnaires approved in Iran, the variables related to
sexual performance in male patients were investigated in two groups.
The mean duration of dialysis in men of this group was 16.3 ± 11.28
months. This variable for the second group was equal to 22.98 ± 19.15
months for men. According to the inclusion criteria, the minimum
duration of dialysis was 6 months and the maximum duration was
108 months. In the study by Dr. Mehrsai et al., the minimum dialysis
time was 6 months and the maximum was 120 months [7], which is
not significantly different from the present study. In another study in
2013, the studied patients underwent haemodialysis for a minimum
of 7 months and a maximum of 89 months [6]. The existing difference
shows that probably the patients in this study underwent intervention
and kidney transplant operation faster.
In men of the first group, the mean BMI index was 24.98 ± 3.77
kg/m2 with a minimum of 16.50 kg/m2 and a maximum of 32.91 kg/
m2. In men of the second group, the mean of this index was 24.13 ±
4.22 kg/m2 with a minimum range of 15.90 kg/m2 and a maximum
range of 35.46 kg/m2.The mean of serum creatinine level is one of the
variables measured and recorded in patients of both groups, before
and after transplantation. In male patients, the mean baseline level of
creatinine was different in two groups (7.77 ± 2.5 in the first group and
5.48 ± 1.72 in the second group).The average decrease in creatinine in
the cadaveric donor group was slightly higher than the living donor
group (83.36 ± 1.2 in the living donor and 1.77 ± 0.67 in the cadaveric
donor), although again this difference was not statistically significant
(P>0.05).
In a study conducted in 2013 to compare sexual performance
of haemodialysis and kidney transplant patients [20], creatinine
of patients after kidney transplant was reported as 0.9, which was
equal to the control group. The lower mean level of creatinine in the
aforementioned study compared to the previous study can be related
to factors such as the difference in the baseline creatinine level and
physical and gender conditions of population of the two studies,
Because different factors affect the level of creatinine and its clearance
in the body. Therefore, without demographic uniformity, this
variable cannot be compared in various studies. The relationship and
correlation between the investigated variables and sexual function of
male patients were examined separately in both groups.
According to P-values and correlation coefficients obtained in
male patients of both groups, there is an inverse relationship between
the age of patients and sexual performance before transplantation,
3 months later and 9 months later. There is a direct relationship
between BUN and triglyceride levels and sexual function before
transplantation. Sexual performance 3 months after transplantation
has a direct relationship with the level of triglycerides and haemoglobin.
At the time of 9 months after transplantation, a direct relationship is
seen between haemoglobin and sexual dysfunction. Other variables
examined at certain times have no significant relationship with
sexual performance in male patients of both groups.According to the
reports of Dr. Momeni et al.’s [21], age has an inverse relationship
with all gender variables in male patients. This report is consistent
with the present study; considering the decrease in sexual desire
naturally with age, it seems reasonable and has no relationship with
the type of kidney transplant. In the above study, the blood pressure
of patients has a direct relationship with their sexual performance, while the present study reported an inverse relationship between
blood pressure and sexual performance of patients, considering that
the prevalence of sexual dysfunction in the hypertensive population is
more than normal population, the inverse relationship between these
factors is not far from expected and seems logical.
As the main objective of the study, sexual dysfunction of men in
two groups was compared on three occasions, before transplantation,
3 months after transplantation and 9 months later. At the time before
transplantation (P-value = 0.028), there is a significant difference
in ED sexual performance between the two groups, and according
to the mean, men in the first group performed better. According to
P-value=0.006, there was a significant difference between men of
the two groups in ED index 3 months after transplantation, and the
first group performed better. According to P-value=0.002, there is a
significant difference in ED sexual performance between men of the
two groups at 9 months after transplantation; according to the mean,
the men of the first group performed better. Finally, it is shown that
the first group (living donor) compared to the second group, had a
better sexual performance in all 3 occasions, although this difference
is only statistically significant for desire.
According to Brancoet al., although the living donor group is
better than the cadaveric donor group in terms of improving sexual
dysfunction, relationship satisfaction, and orgasm, this difference is
only statistically significant regarding the satisfaction. These results
are roughly consistent with the current study and show that, in
general, sexual function of patients after kidney transplantation from
a living donor is somewhat better than that of patients receiving
from a cadaveric donor. As Barroso et al reported, due to the
prevalence of sexual dysfunction in patients with ESRD following
uremia and other factors, sexual function of patients improves after
kidney transplantation compared to hemodialysis [17], and it was
reported that the difference in desire of kidney transplant candidates
is significantly higher. This review is consistent with the upcoming
study and shows the effect of kidney transplant on desire.
Again, an intra-group investigation was conducted in order to
investigate the process of changing sexual performance in men of
both groups. According to Table 4-36, P-value shows that there is a
significant difference in all cases of ED sexual dysfunction comparison
in the group of living donor patients; considering the increase of
the mean with the increase of time after transplantation, improved
sexual function of patients after transplantation is evident. According
to Table 4-37, P-values show that there is a significant difference
in all cases of ED sexual dysfunction comparison in the group of
cadaveric donor patients; considering the increase of the mean with
the increase of time after transplantation, improved sexual function
of patients after transplantation is evident. Finally, sexual function of
the living donor patients improved after transplantation. Although
in the comparison between the two groups, cadaveric donor patients
show better conditions than living donor patients at all times in
factors related to sexual performance, the difference between the two
groups is not statistically significant in terms of variables related to
sexual performance, except in desire.
References
Citation
Behtash N, Nikoobakht MR. Comparison of Sexual Function Changes between Two Groups of Male Kidney Recipients from Living Donor and
Cadaveric Donor. J Urol Nephrol. 2022;9(1): 7.