Clinical Image
Double Barrel Wet Colostomy for Urinary and Fecal Diversion
Yu-Hao Xue and Chih-Hsiung Kang*
- Department of Urology, Chang Gung Memorial Hospital-Kaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan, Republic of China
*Address for Correspondence: Chih-Hsiung Kang, Department of Urology, Chang Gung Memorial Hospital - Kaohsiung Medical Center, Chang Gung University College of Medicine, Taiwan,E-mail: chkang5801@gmail.com
Citation: Kang CH, Xue YH. Double Barrel Wet Colostomy for Urinary and Fecal Diversion. J Urol Nephrol. 2017;4(2): 1.
Journal of Urology & Nephrology| ISSN: 2380-0585 | Volume: 4, Issue: 2
Submission: 30 October, 2017| Accepted: 06 November, 2017 | Published: 10 November, 2017
Submission: 30 October, 2017| Accepted: 06 November, 2017 | Published: 10 November, 2017
Abstract
A 60-year-old male who had a history of spinal cord injury received loop colostomy for fecal diversion and cystostomy for urinary diversion. Because he was diagnosed with muscle invasive bladder cancer, radical cystectomy and double barrel wet colostomy was conducted. Computed tomography showed simultaneous urinary and fecal diversion and stone formation in the distal segment of colon conduit with urinary diversion.
Keywords
Double barrel wet colostomy; Urinary diversion; Fecal diversion
Introduction
In patients with an advanced primary or recurrent carcinoma, double-barreled wet colostomy can be used for pelvic exenteration and urinary tract reconstruction. It is a technique that separate urinary and fecal diversion with a single abdominal stoma. Distal end of the colon was sectioned and closed and bilateral ureters were implanted into the formed colon conduit. This technique can reduce ascending infection by avoiding fecal reflux to pelvis.
Clinical Image
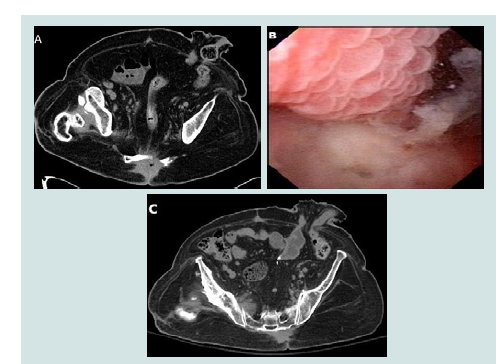
A 60-year-old male presented to the emergency department with bloody urine in urinary bag for one day. He had a history of spinal cord injury due to traffic accident with paraplegia for over 30 years. He received loop colostomy for fecal diversion and cystostomy for urinary diversion. Computed Tomography (CT) showed loop colostomy with both the proximal limb and the distal limb open into the common stoma opening (Figure 1A). Fibero cystoscopy showed irregular papillary tumors over posterior wall (Figure 1B). He was diagnosed with muscle invasive bladder cancer by transurethral resection of bladder tumour and radical cystectomy with pelvis lymph node dissection was done. Pathology report showed urothelial carcinoma with squamous differentiation, high grade, TNM stage: pT2a N0 stage II. Additionally double barrel wet colostomy was conducted. Distal end of the colon was sectioned and closed at about 13 cm distal to the stoma and bilateral ureters were implanted into the formed colon conduit. CT after six months showed simultaneous urinary and fecal diversion and stone formation in the distal segment of colon conduit with urinary diversion (Figure 1C). The formation of calculi might be due to urinary stasis after urinary surgical diversion.
Bilateral hydroureters and mild hydronephrosis were noted and we suspected the calculi impacted in bilateral ureteto-colostomy anastomosis sites. After lithotripsy of the stones in colon conduit by cystoscopy, hydronephrosis improved and the patient continued be monitored with smooth condition.