
Case Report
*Address for Correspondence: Christina Irene Guenter, MD, Head, Clinical Trials Research Group, Clinic for Plastic and Hand Surgery, University Hospital rechts der Isar, Technische Universität München, Ismaninger Str. 22, 81675 München, Germany, Tel: +49 89 4140 6474; Fax: +49 89 4140 6479; E-mail: Christina.Guenter@lrz.tum.de
Citation: Guenter CI, Kern L, Giri S, Machens HG, Bader A. First Results on Three Patients Treated with Topical Recombinant Human Erythropoietin(rhEPO) to Improve Wound Healing in Diabetic Foot Ulcers. J Transplant Stem Cel Biol. 2015;2(1): 4.
Copyright © 2015 Guenter CI, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Transplantation & Stem Cell Biology | ISSN 2374-9326 | Volume: 2, Issue: 1
Submission: 26 November 2014 | Accepted: 17 January 2015 | Published: 22 January 2015
 Patient two (Figure 2) had a slow but stable granulation of the wound; the granulation tissue grew over the exposed bone and tendon. A marked increase of vessel ingrowths into the area of the wound was seen, clearly recognizable by the increasing redness of the wound surface. A biopsy taken before the split skin graft transplantation showed normal granulation tissue, typical for a chronic ulcer. After transplantation she showed a 100% take of the split skin graft; the scar is stable since and presents a smooth texture and fairly reddish color. She can walk without help and participate in many normal daily activities, like going shopping and swimming.
Patient two (Figure 2) had a slow but stable granulation of the wound; the granulation tissue grew over the exposed bone and tendon. A marked increase of vessel ingrowths into the area of the wound was seen, clearly recognizable by the increasing redness of the wound surface. A biopsy taken before the split skin graft transplantation showed normal granulation tissue, typical for a chronic ulcer. After transplantation she showed a 100% take of the split skin graft; the scar is stable since and presents a smooth texture and fairly reddish color. She can walk without help and participate in many normal daily activities, like going shopping and swimming.

Patient three (Figure 3) showed no changes in blood values during the treatment, the granulation and epithelialization of the wound were stable. In addition the remaining wound healed without complications after the free flap transplantation and has a stable scar situation since than. She can walk short distances and participate in most of the normal daily activities wearing special custom-made shoes.

First Results on Three Patients Treated with Topical Recombinant Human Erythropoietin (rhEPO) to Improve Wound Healing in Diabetic Foot Ulcers
Christina I Guenter2*, Larissa Kern1, Shibashish Giri1, Hans-Günther Machens2 and Augustinus Bader1
- 1Stem cell biology and cell technology, Biotechnological-Biomedical Centre (BBZ), Faculty of Medicine, Leipzig University Deutscher Platz, Leipzig, Germany
- 2Clinic for Plastic and Hand Surgery, University Hospital rechts der Isar, Technische Universität, München, Germany
*Address for Correspondence: Christina Irene Guenter, MD, Head, Clinical Trials Research Group, Clinic for Plastic and Hand Surgery, University Hospital rechts der Isar, Technische Universität München, Ismaninger Str. 22, 81675 München, Germany, Tel: +49 89 4140 6474; Fax: +49 89 4140 6479; E-mail: Christina.Guenter@lrz.tum.de
Citation: Guenter CI, Kern L, Giri S, Machens HG, Bader A. First Results on Three Patients Treated with Topical Recombinant Human Erythropoietin(rhEPO) to Improve Wound Healing in Diabetic Foot Ulcers. J Transplant Stem Cel Biol. 2015;2(1): 4.
Copyright © 2015 Guenter CI, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Transplantation & Stem Cell Biology | ISSN 2374-9326 | Volume: 2, Issue: 1
Submission: 26 November 2014 | Accepted: 17 January 2015 | Published: 22 January 2015
Abstract
Chronic wounds not only induce individual distress but also cause enormous and rapidly growing costs for our health care systems and society in general. The fastest growing groups of chronic wounds are Diabetic Foot Ulcers (DFU), due to the fact that the number of diabetics is growing worldwide.The pathophysiology of DFU is complex and necessitates interventions at multiple levels. Several of these intervention levels can be addressed by topical application of recombinant human Erythropoietin hydro gel (rhEPO hydro gel). We report here the cases of 3 adult patients with controlled diabetes and DFU who were treated in a compassionate healing attempt with topical rhEPO-Hydro gel. In addition patients received state-of-the-art diabetes and DFU treatment. In all three patients complete healing of the DFU with stable long term results could be achieved. Based on these observations, rhEPO hydro gel seems to be a promising treatment option for patients with DFU. GCP conform clinical studies will be necessary to confirm these results in a larger population of patients.
Keywords
Diabetic foot ulcer; Chronic wound; rhErythropoiethin; Topical treatmentIntroduction
Chronic wounds affect millions of patients worldwide. In addition to the individual distress, chronic wounds induce enormous and rapidly growing costs for our health care systems and society in general [1]. Therefore medically effective and cost efficient treatment methods are desperately needed.The fastest growing sub-group of chronic wounds are Diabetic Foot Ulcers (DFU) [2,3]. The pathophysiology of DFU is complex and necessitates interventions at multiple levels [4,5]. DFU remain in a chronic inflammatory state (increased amounts of IL-1, TNF-alpha, neutrophils and macrophages) [6,7]. Microcirculation is impaired in DFU due to endothelial dysfunction and low levels of VEGF resulting in decreased angiogenesis [8-10]. A large number of growth factors and their release-regulation are affected in DFU resulting in a non-healing environment [11]. Extracellular matrix formation is disturbed, cell proliferation and migration is impaired [12,13]. Keratinocytes and fibroblasts in diabetic wounds display pathological characteristics. Impaired migration capacity, excessive apoptosis and decreased clone formation capacity of their progenitor cells isolated from chronic wounds were described [14-16].
Supportive treatment of chronic wounds in DFU by biological agents would ideally counter several or all of these problems. A possible candidate for such a supportive treatment is Erythropoietin (EPO). EPO is directly activated by the transcription factors that mediate signaling in hypoxic tissues: HIF-1α, HIF-1α–like factor, HLF (also known as EPAS1) and HIF-2α [17-19]. For EPO antiinflammatory effects have been demonstrated, it has been shown to influence growth factor release regulation, it activates angiogenesis and microcirculation, stimulates extra cellular matrix formation, re-epithelization and stem cell recruitment, and enhances fibroblast and kerationocyte proliferation [20-24]. Furthermore in skin EPO seems to mediate down-regulation of the expression of inflammatory cytokines and degradative enzymes [25]. EPO also works in concert with vascular endothelial growth factor (VEGF). Together they stimulate endothelial cell mitosis and motility, which is important for new vessel growth and wound healing [26]. It has been shown to mobilize circulating bone marrow derived cell populations andmediate vascular repair in both acute and chronic tissue injuries [27,28]. EPO stimulates endothelial progenitor cell proliferation, adhesion, and differentiation to endothelium. Furthermore inhibition of apoptosis provides evidence of a cytoprotective effect [29,30]. In mouse skin the combined presence of EPO receptor and the EPOhetero- receptor was demonstrated on the stem cells of hair follicles [26].
Studies in diabetic animal models have shown that systemically and topically applied EPO can advance the healing process. Elevated VEGF and EGF levels, elevated iNOS-endothelial nitric monoxide synthase (eNOS)-and NO content within the wound tissue, a higher capillary density, as well as higher hyroxyprolin and collagen densities were described after application of EPO. Increase in haematocrit values or other systemic EPO-effects were not reported in these studies [31,32].
We report here on three patients treated as compassionate healing attempts with rhEPO hydro gel as a topical treatment for DFU.
Methods
The healing attempts were conducted according the standards of good clinical practice (as defined in the ICH E6 Guideline for Good Clinical Practice, 1 May 1996), in agreement with the Declaration of Helsinki and with local regulations and local regulatory authorities. Detailed information about the healing attempt was given to the patients and informed consent in written form was obtained before the treatment was performed. An ethics approval was not necessary.In total 3 adult patients (two females, one male) aged 61, 65 and 69 years with controlled type two diabetes mellitus and chronic wounds were treated with topical rhEPO hydro gel. In addition patients received state-of-the-art diabetes and DFU treatment according to S3-guidelines [33]. Dressing changes, wound documentation, photo documentation and control of safety parameters were performed according to the standard treatment regulations of the clinic: Initially a state of the art clinical assessment including physical examination,assessment of perfusion status, polyneuropathy assessment, exclusion of a macroangiopathy requiring treatment, diagnostics for osteomyelitis and if needed other special assessments were performed. A sufficient surgical debridement was performed before the beginning of the treatment. During the debridement biopsies were taken to exclude malignant diseases as course of the ulcers and to diagnose/exclude osteomyelitis.
After application of rhEPO hydro gel the DFUs were dressed with occlusive dressings. Dressing changes and wound controls were performed two to three times per week. Patients received a standardized antithrombotic therapy with body weight-adjusted Low-Molecular-Weight-Heparin s.c. if immobilized.
Clinical wound assessment and photo documentations were performed during the dressing changes.
Patients
Patient one was a 65 year old male with controlled Type II diabetes, a known peripheral artery disease and a history of multiple ulcerations and gangrene, as well as amputations of the 1. toe of the right foot. He presented with a 3x2 cm ulcer directly under the metatarsal joint and an acute infected necrosis of his 3. toe at the left foot. We started with the debridement of the ulcer, than he received in total 6.000 IU rhEPO in hydro gel (3x2.000 IU rhEPO in 10 ml hydrocolloid-hydro gel, Varihesive® hydrogel), during 8 visits, three times per week, during 18 days. After receiving a vital and well granulated wound ground we transplanted a full thickness skin graft to the remaining ulcer and amputated D III due to acute osteomyelitis (Treatment phase: 08/2013 – 09/2013).
Patient two was a 69 year old lady with type II diabetes, obesity (BMI 32), varicose veins, a peripheral artery disease and a variety of allergies including intolerances against several wound dressing materials. She had developed a 10x4 cm ulcer of her lateral malleolus region at her right lower leg with exposure of bone and tendons after she had suffered an open fracture of her lower leg 8 years ago. She had developed a low grade chronic osteomyelitis and a pseudarthrosis of the fibula. She was initially debrided, subsequently she received 3.000 IU rhEPO in 15 ml hydrocolloid-hydro gel (Varihesive® hydrogel) three times per week for 25 weeks thereafter a split skin graft transplantation was performed (Treatment phase: 07/2012-03/2013).
Patient three was a 61 one year old lady with known type II diabetes; she had had lithotripsy of ureter stones, and subsequently developed an urosepsis, acral necrosis, and osteomyelitis of the calcaneal bone. Amputations of the necrotic areas had to be performed and excision of the osteomyelitis at the calcaneal bone. The defect was initially covered with a musculus suralis flap, which failed. Thereafter the patient received 9 times 2.000 IU rhEPO in 10 ml hydrocolloid-hydro gel (Varihesive® hydrogel) once per week. Thereafter the remaining ulcer was treated conservatively for two months. In succession a secondary free flap reconstruction was performed which healed and stayed stable (Treatment phase: 04/2008-07/2008).
Results
All three wounds were closed completely. No significant changes in blood values were seen during the phase of treatment.In patient one (Figure 1) a marked increase of granulation tissue was already seen at the time point of the first dressing change. The wound healed completely within 8 days after the full thickness skin graft transplantation. Since then, the scar stayed stable, he can walk and participate in the normal daily activities wearing a special custom-made shoe.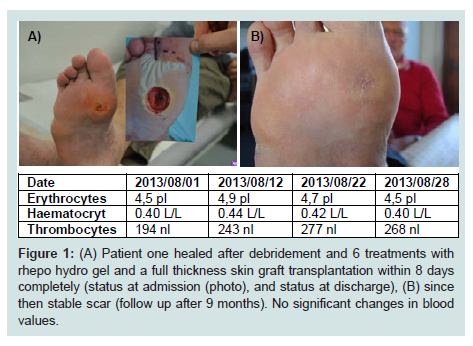
Figure 1: (A) Patient one healed after debridement and 6 treatments with rhepo hydro gel and a full thickness skin graft transplantation within 8 days completely (status at admission (photo), and status at discharge), (B) since then stable scar (follow up after 9 months). No significant changes in blood values.
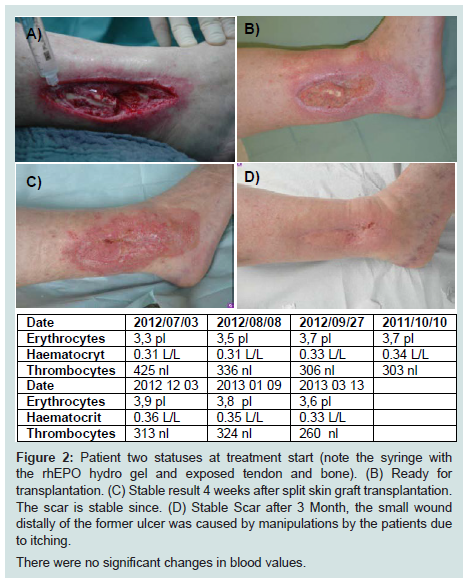
Figure 2: Patient two statuses at treatment start (note the syringe with the rhEPO hydro gel and exposed tendon and bone). (B) Ready for transplantation. (C) Stable result 4 weeks after split skin graft transplantation. The scar is stable since. (D) Stable Scar after 3 Month, the small wound distally of the former ulcer was caused by manipulations by the patients due to itching.There were no significant changes in blood values.

Figure 3: (A) Patient three, status at treatment start. (B) Status before the flap transplantation. (C) The wound healed without complications after the free flap transplantation and has a stable scar situation since. (D) Thus both lower extremities could be preserved.Blood values did not change significantly
Discussion
The use of rhEPO in the treatment of chronic wounds has been described in few patients before [25,34,35]. The only GCP conform trial protocol for a multi-centre study investigating the effects of systemically applied EPO in an acute wound, e.g. severely burned patients was recently published by the authors of this article, who have just finished the follow-up phase [25].High dose systemic administration of rhEPO has been evaluated in a large number of randomized clinical trials in several fields, such as stroke (brain), myocardial infarction (myocardium), acute renal failure (kidney), kidney transplantation (reperfusion injury) but so far all trials failed to confirm the protective potential of high dose systemic applicated rhEPO, despite encouraging preclinical (animal models) results [36,37]. Furthermore in some of the trials an increased mortality was revealed, most of them connected with an increased numbers of thrombo-embolic events in combination with increasing haematocrit and erythrocyte values [29,[30,[38]. As the heamatocratic action of rhEPO is a well known fact of systemically applied rhEPO an increase in haematocrit and erythrocyte values is to be expected. On the contrary low dose topically applied rhEPO has not shown any changes in haematocrit and erythrocyte values, this was evaluated in several animal models and observed by us in the three patients described in this paper [32].
Therefore as discussed in the introduction there are several reasons to believe that topical treatment with low dose rhEPO hydro gel may improve wound healing. rhEPO is a well-known drug used for nearly 30 years in the daily clinical routine in the field of anemia treatment [39]. Therefore possible adverse effects are well known and were accounted for in the three patients reported here. We controlled the blood values in our patients on a regular basis. As we could not see any changes in the laboratory parameters, there was obviously no hematopoietic reaction during our treatments. In combination with increasing haematocrit and erythrocyte values increased numbers of thrombo-embolic events have been described. As we did not see any suspicious changes in the blood values we did not see an indication for premature ending of the treatment [38].
EPO is further known to increase blood pressure in already hypertonic patients [38,40]. Therefore we did not treat any patients with therapy resistant arterial hypertension. Maybe the most serious described side effect of rhEPO in patients with malignant tumors is an activation of tumor-progression. In several trials, where patients were treated with EPO for tumor induced anemia, it could be shown that the mortality rate of the EPO-treated groups was higher than of the non-treated controls [37]. Therefore, we did not treat any patients with known malignant diseases.
Patient age, gender, nutritional status, concomitant illnesses, as well as wound infections have a large influence on the patient’s prognosis and the wound healing. Therefore we considered all mentioned factors carefully and discussed their relevance for our healing attempts. Concomitant illnesses are important factors especially if they interact with EPO. Thus, as stated above, we did not treat patients with illnesses such as hypertension, malignant diseases, active infectious diseases or clinically relevant cardiovascular or systemic diseases etc. which have a known interaction with EPO [6].
As the patients have received different combinations of EPO, surgery and advanced wound management, it can not be postulated at the present state that the successful healing was a direct effect of the rhEPO-treatment.
However the completely healed wounds in all patients and the absence of any EPO related complications or any complications possibly connected to the hydro gel raise the hope that the patients may profit from activation of the EPO-pathway.
GCP conform clinical studies will however be necessary to be able to confirm this assumption in a larger population of patients.
Acknowledgements
We kindly thank our patients to have given written consent to the publishing of the documentation photos.References
- Richter-Kuhlmann E (2012) Zivilisationskrankheiten nehmen zu. D Ärztebl 109: A1376-1377.
- Jeffcoate WJ, Harding KG (2003) Diabetic foot ulcers. Lancet 361: 1545-1551.
- Cowie CC, Rust KF, Ford ES, Eberhardt MS, Byrd-Holt DD, et al. (2009) Full accounting of diabetes and pre-diabetes in the U.S. population in 1988-1994 and 2005-2006. Diabetes Care 32: 287-294.
- Apelqvist J, Ragnarson-Tennvall G, Persson U, Larsson J (1994) Diabetic foot ulcers in a multidisciplinary setting. An economic analysis of primary healing and healing with amputation. J Intern Med 235: 463-471.
- Cavanagh PR, Lipsky BA, Bradbury AW, Botek G (2005) Treatment for diabetic foot ulcers. Lancet 366: 1725-1735.
- Guo S, Dipietro LA (2010) Factors affecting wound healing. J Dent Res 89: 219-229.
- Martin P (1997) Wound healing-aiming for perfect skin regeneration. Science 276: 75-81.
- Kolluru GK, Bir SC, Kevil CG (2012) Endothelial dysfunction and diabetes: effects on angiogenesis, vascular remodeling, and wound healing. Int J Vasc Med 2012: 918267.
- Kämpfer H, Pfeilschifter J, Frank S (2001) Expressional regulation of angiopoietin-1 and -2 and the tie-1 and -2 receptor tyrosine kinases during cutaneous wound healing: a comparative study of normal and impaired repair. Lab Invest 81: 361-373.
- Liu ZJ, Velazquez OC (2008) Hyperoxia, endothelial progenitor cell mobilization, and diabetic wound healing. Antioxid Redox Sig 10: 1869-1882.
- Berlanga-Acosta J (2011) Diabetic lower extremity wounds: the rationale for growth factors-based infiltration treatment. Int Wound J 8: 612-620.
- Mast BA, Schultz GS (1996) Interactions of cytokines, growth factors, and proteases in acute and chronic wounds. Wound Repair Regen 4: 411-420.
- Brem H, Tomic-Canic M (2007) Cellular and molecular basis of wound healing in diabetes. J Clin Invest 117: 1219-1222.
- Usui ML, Mansbridge JN, Carter WG, Fujita M, Olerud JE (2008) Keratinocyte migration, proliferation, and differentiation in chronic ulcers from patients with diabetes and normal wounds. J Histochem Cytochem 56: 687-696.
- Lerman OZ, Galiano RD, Armour M, Levine JP, Gurtner GC (2003) Cellular dysfunction in the diabetic fibroblast: impairment in migration, vascular endothelial growth factor production, and response to hypoxia. Am J Pathol 162: 303-312.
- Hocking AM, Gibran NS (2010) Mesenchymal stem cells: paracrine signaling and differentiation during cutaneous wound repair. Exp Cell Res 316: 2213-2219.
- Wang GL, Jiang BH, Rue EA, Semenza GL (1995) Hypoxia-inducible factor 1 is a basic-helix-loop-helix-PAS heterodimer regulated by cellular O2 tension. Proc Natl Acad Sci USA 92: 5510-5514.
- Wang GL, Semenza GL (1993) Characterization of hypoxia-inducible factor 1 and regulation of DNA binding activity by hypoxia. J Biol Chem 268: 21513-21518.
- Ema M, Taya S, Yokotani N, Sogawa K, Matsuda Y, et al. (1997) A novel bHLH-PAS factor with close sequence similarity to hypoxia-inducible factor 1alpha regulates the VEGF expression and is potentially involved in lung and vascular development. Proc Natl Acad Sci USA 94: 4273-4278.
- Günter CI, Rezaeian F, Harder Y, Lohmeyer JA, Egert S, et al. (2013) Erythropoietin in plastic surgery. Handchir Mikrochir Plast Chir 45: 108-119.
- Brines M, Cerami A (2008) Erythropoietin-mediated tissue protection: reducing collateral damage from the primary injury response. J Intern Med 264: 405-432.
- Guenter CI, Bader A, Dornseifer U, Egert S, Dunda S, et al. (2013) A Multicenter Study on Regenerative Effects of Erythropoietin in Burn and Scald Injuries: study protocol for a randomized controlled trial. Trials 14: 124.
- Arcasoy MO (2008) The non-haematopoietic biological effects of erythropoietin. Br J Haematol 141: 14-31.
- Bader A, Ebert S, Giri S, Kremer M, Liu S, et al. (2012) Skin regeneration with conical and hair follicle sturucture of deep second-degree scaldling injuries via combined expression of the EPO receptor and beta common receptor by local subcutaneous injection of nanosized rhEPO. Int J Nanomedicine 7: 1227-1237.
- Bader A, Lorenz K, Richter A, Scheffler K, Kern L, et al. (2011) Interactive Role of Trauma Cytokines and EPO and their therapeutic potential for acute and chronic wounds. Rejuvenation Res 14: 57-66.
- Buemi M, Galeano M, Sturiale A, Ientile R, Crisafulli C, et al. (2004) Recombinant human erythropoietin stimulates angiogenesis and healing of ischemic skin wounds. Shock 22: 169-173.
- Walker BR, Resta TC, Nelin LD (2000) Nitric oxide-dependent pulmonary vasodilation in polycythemic rats. Am J Physiol Heart Circ Physiol 279: H2382-H2389.
- Bahlmann FH, De Groot K, Spandau JM, Landry AL, Hertel B, et al. (2004) Erythropoietin regulates endothelial progenitor cells. Blood 103: 921-926.
- Amann K, Buzello M, Simonaviciene A, Miltenberger-Miltenyi G, Koch A, et al. (2000) Capillary/myocyte mismatch in the heart in renal failure-a role for erythropoietin? Nephrol Dial Transplant 15: 964-969.
- van der Meer P, Voors AA, Lipsic E, van Gilst WH, van Veldhuisen DJ (2004) Erythropoietin in cardiovascular diseases. Eur Heart J 25: 285-291.
- Galeano M, Altavilla D, Cucinotta D, Russo GT, Calò M, et al. (2004) Recombinant human erythropoietin stimulates angiogenesis and wound healing in the genetically diabetic mouse. Diabetes 53: 2509-2517.
- Hamed S, Ullmann Y, Masoud M, Hellou E, Khamaysi Z, et al. (2010) Topical erythropoietin promotes wound repair in diabetic rats. J Invest Dermatol 130: 287-294.
- Maier-Hasselmann A, Wilm S (2012) Epidemiologie. In: S3-Leitlinie: Lokaltherapie chronischer Wunden bei Patienten mit den Risiken periphere arterielle Verschlusskrankheit, Diabetes mellitus, chronisch venöse Insuffizienz. Edited by Deutsche Gesellschaft für Wundheilung und Wundbehandlung e.V 2012: 1-287.
- Ferri C, Giuggioli D, Sebastiani M, Colaci M (2007) Treatment of severe scleroderma skin ulcers with recombinant human erythropoietin. Clin Exp Dermatol 27: 287-290.
- Keast DH, Fraser C (2004) Treatment of chronic skin ulcers in individuals with anemia of chronic disease using recombinant human erythropoietin (EPO): a review of four cases. Ostomy Wound Manage 50: 64-70.
- Lund A, Lundby C, Olsen NV (2014) High-dose erythropoietin for tissue protection. Eur J Clin Invest 44: 1230-1238.
- Vlachopanos G, Kassimatis TI, Agrafiotis A (2014) Peri-operative administration of high dose recombinant human erythropoietin for delayed graft function prevention in kidney transplantation: a meta-analysis. Transpl Int 17.
- Corwin HL, Gettinger A, Fabian TC, May A, Pearl RG, et al. (2007) Efficacy and safety of epoetin alfa in critically ill patients. N Engl J Med 357: 965-976.
- Jelkmann W (2007) Erythropoietin after a century of research: younger than ever. Eur J Haematol 78: 183-205.
- Gebrauchsinformation: information fürden anwender (2011) NeoRecormon Multidose 50.000 IE. Roche Pharma AG.