
Journal of Syndromes
Download PDF
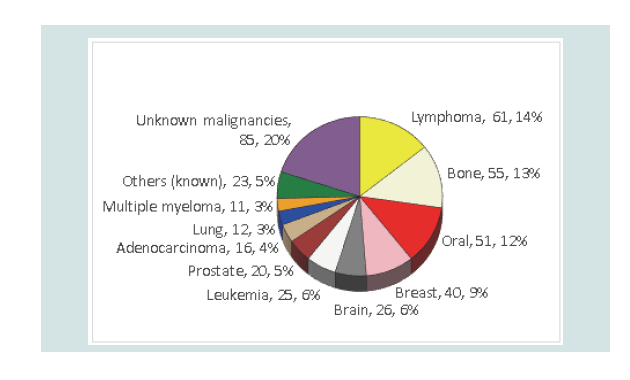 Figure 1: Cancer types and unknown malignancies associated with NCS.
Figure 1: Cancer types and unknown malignancies associated with NCS.
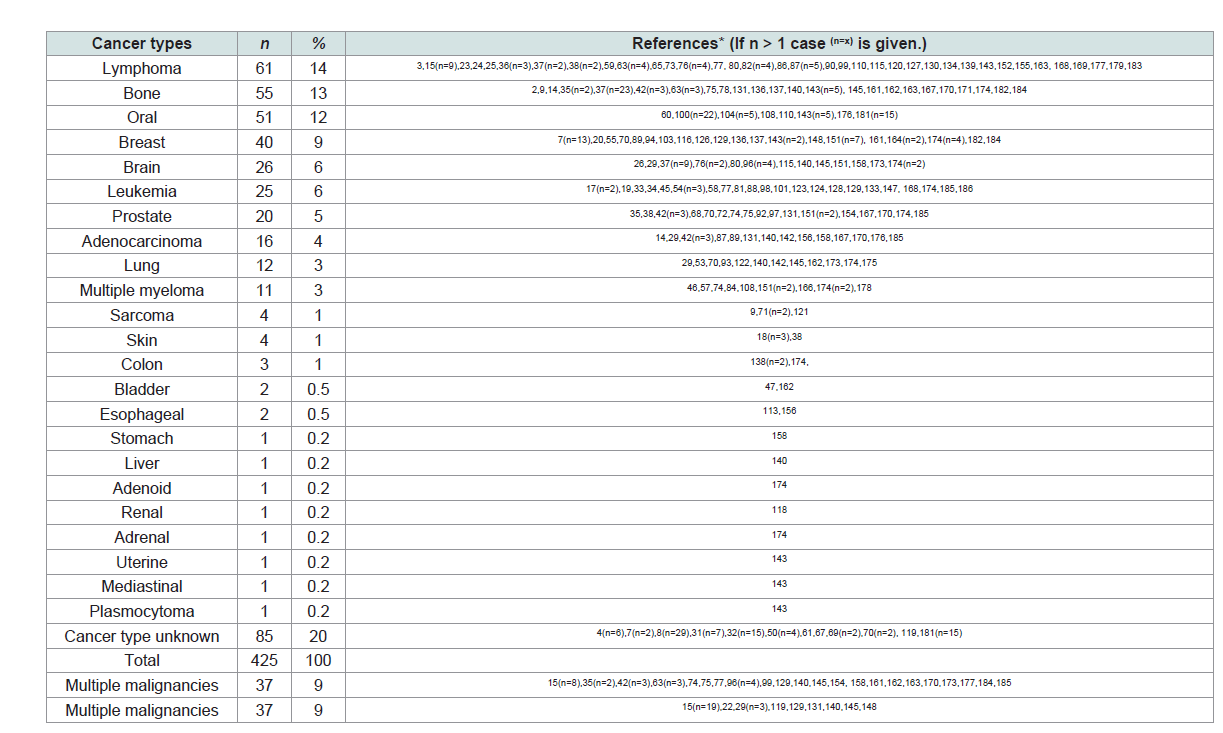 Table 1: NCS related cancer cases.
Table 1: NCS related cancer cases.
Case Report
Numb Chin Syndrome: Diagnostic Significance Over 57 Years and Review of 550 Patients in the Literature Worldwide
Robert E. Brandt1,2*, Akihiro Takeuchi2 and Hirotoshi Kamata3
1MedEd Japan, Tokyo, Japan
2Department of Medical Informatics, Kitasato University School of Medicine, Kanagawa, Japan
3Department of Hematology, Kitasato University School of Medicine, Kanagawa, Japan
*Address for Correspondence: Robert E. Brandt, MedEd Japan, Department of Medical Informatics, Kitasato University School of Medicine, Kanagawa, 3-2-12 Eifuku, Suginami, Tokyo 168-0064, Japan, Tel: +81-3-5930-4568, Fax: +81-42-778-9176; E-mail: robert_e_brandt@hotmail.com
Submission: June 10, 2020;
Accepted: July 17, 2020;
Published: July 21, 2020
Copyright: © 2020 Brandt RE, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Numb Chin Syndrome (NCS) is a heterogeneous condition of mental nerve neuropathy playing in concert with multiple disease mechanisms, but all result in a disruption of unilateral or bilateral facial nerves, fever, and swelling of the lower lip. The NCS has been reported as a prodromal symptom of pending malignancies, a possible precursor of cancer or leukemia, and sometimes merely a benign, painful or annoying, condition. However, any causal relationships between the NCS and malignancy have not been made, were not aggregated, and therefore remain unclear. This thorough review of all the available current literature in the PubMed interface was performed by using the key words, “mental neuropathy,” “mental nerve numbness,” and “numb chin syndrome.” There were 186 peerreviewed articles reporting 550 patients from 28 countries worldwide including 150 benign, 398 malignant, and 2 unknown cases. The seven most common malignancies from high to low frequency were: lymphoma, bone cancer, oral cancer, breast cancer, brain cancer, leukemia, and prostate cancer. While the clinical implications of the NCS are not fully understood, this delineative study will aid physicians confronted and confounded with various malignancies, neuropathies, and cytogenetic abnormalities of patients initially presenting with the
symptom of a numb chin.
Keywords
Numb chin syndrome; Mental neuropathy; Mental nerve numbness; Lymphoma; Leukemia; Brain; Bone; Breast; Prostate; Cancer
Abbreviations
HIV: Human Immunodeficiency Virus; MRI: Magnetic Resonance Imagining; NCS: Numb Chin Syndrome; USA: United States of America
Introduction
Numb Chin Syndrome (NCS) is a set of neuropathological
symptoms including lower facial numbness, due to paralysis of the
distal trigeminal nerve, especially right, unilateral, dysesthesia or
paresthesia (numbness) of the chin, local fever, swelling, redness,
persistent pain, a thickening sensation of the lower lip, and dullness
in the mandible. When contemplating this worldwide, not too rare
disease of the numb chin, a mental image of Rodin’s famous bronze
statue, “The Thinker” comes to mind. He is pressing the back of his
right hand to the right side of his chin, right elbow to his left knee.
Is he applying presure to alleviate some pain, feeling numbness in
his chin, contemplating some kind of worsening condition? Or what?
We wonder. Sitting in this position, what is he thinking?
In the beginning in London, Charles Bell first described this
syndrome in 1830 in a woman with breast cancer and noting mental
nerve anesthesia in patients presenting with trauma to the jaw and
retromandibular tumors [1]. In the United States of America, numb chin was first mentioned as a syndrome, in 1963 as an innocuous
symptom, albeit an ominous one, that would indicate metastasis and
manifest malignancy [2]. In Japan, the NCS was first reported in 1989
as the initial manifestation of a case of Burkitt’s lymphoma [3].
Now, 190 years after Bell’s first mention of it [1], we have attempted
to determine if the fulminant numb chin is an ominous sign of an
upcoming malignancy, a prodromal syndrome of a life threatening
disease, or merely a benign but painful nuisance. Although there have
been various reviews reporting malignancies and diseases associated
with a numb chin, they focus on certan kinds of malignancies, such
as lymphoma, leukemia, lung, breast, brain, bone, and prostrate
cancers, among other major noncancerous maladies. The aim of this
study was, therefore, to summarize all of the reported cases of the
NCS from all over the world for the last 57 years, looking into benign
and malignant cases, to determine if there were any patterns that may
suggest or even prove causality.
Subjects and Methods
An NCS review was performed of all the available current
literature in the PubMed interface, during the 57-year period from
1963 to 2020. The key words “mental neuropathy,” “mental nerve
numbness,” and “numb chin syndrome” generated a considerable
body of literature comprised of 186 relevant, peer-reviewed articles.
The reported cases were manually counted for the various signs and
symptoms, histories, diagnoses, treatments, prognoses, and actual
outcomes.
Results
A retrospective analysis of 186 articles revealing 550 patients,
who presented with signs and symptoms of the NCS at 122 sites in 28
countries throughout Europe (n = 198), North and South America (n
= 177), the Middle East (n = 107) and the Asia/Pacific region (n = 68),
composed this exhaustive study. The range in patients’ ages was from 7 to 82 years old with middle-age to elderly patients affected most and
337 patients for whom age was not reported. Regarding gender, there
were 88 men, 98 women, and 364 patients for whom gender was not
reported.
Patients presenting at the dental office or at their local healthcare
clinic with lower facial numbness in the area of the distal trigeminal
nerve, numbness of the chin, especially the right side, local fever,
swelling, redness, persistent pain, a thickening sensation of the lower
lip, and an aching and dullness in the jawbone, all warrant an MRI.
These signs and symptoms could likely manifest an unknown or as
yet undiagnosed cancer, as discovered in 86 of 550 patients, or they
could be the first prodromal set of symptoms manifesting a systemic
malignancy, as it was for 29 patients in the present series. Worldwide,
of 550 reported NCS patients there were 150 benign cases (27%) and
malignancies in 398 (72%) including 63 deaths (11%). Two cases were
not reported whether they were begin or malignant, and 37 cases (7%)
were of multiple malignancies. These factors caused the discrepancy
between the number of malignancies 398 versus the number of
patients with malignancies (n = 380).
The initial presentation of this group of NCS symptoms helped
physicians diagnose 340 (80%) of 425 cases as one of the 23 cancer
types (Table 1). The seven most common malignancies from high to
low frequency were: lymphoma (n = 61, 15%), bone cancer (n = 55,
14%), oral cancer (n = 51, 13%), breast cancer (n = 40, 9%), brain
cancer (n = 26, 7%), leukemia (n = 25, 6%), and prostate cancer (n =
20, 5%). Moreover, of the 398 (72%) malignancies, there were 37 (9%)
cases of multiple malignancies, 29 (7%) systemic malignancies, and as
many as 85 (20%) unspecified malignancies (Figure 1).
With the advances in diagnostics, although the terminology and
classifications of hematopoetic and lymphoid tumours continue to
evolve and change, the counting in this study was done according
to the diagnoses at the time of each of those published reports.
Lymphoma (n = 61) was subclassified as: B-cell lymphoma (n =
17), Hodgkin (n = 2) and non-Hodgkin lymphoma (n = 8), Burkitt
lymphoma (n = 9), and lymphoblastic lymphoma (n = 2). Leukemia
(n = 25) was subclassified into acute lymphoblastic leukemia (n =
8), acute myeloid leukemia (n = 2), and Burkitt’s leukemia (n = 10).
There were 31 patients presenting with the symptoms of NCS who
were diagnosed as having Burkitt (non-Hodgkin) lymphoma and/
or Burkitt’s leukemia; and 3 of those 13 Burkitt’s leukemia patients
were HIV positive. Noteworthy, there were 11 cases of NCS related to B-cell lymphoma and 1 case of B-cell acute lymphoblastic leukemia
as the precursor to NCS. Multiple myeloma was reported in 11 cases.
There were only 3 cases reported of NCS symptoms related to colon
cancer and, fortunately but inexplicably, no cases of NCS related to
pancreatic, duodenal, small bowel, rectal, or anal cancer. The specific
types of malignancies of 85 (20%) cases were not reported (Table 1).
There were 150 benign NCS cases (27%) resolved with various
therapies such as periapical surgery or resolved for unknown
reasons after 3 to 14 days of being symptomatic, pain, fever, and
numbness, sometimes lasting up to 2 months, as in 1 case of giant
cell arteritis, also called temporal arteritis, successfully treated with
oral Prednisolone [4]. There was only 1 case reported of recurrence,
and that being one of multiple recurrences, four fulminant painful
but benign attacks, over a period of 16 years [5]. Currently, at 70 years
of age, the 5-year follow-up revealed that patient to be asymptomatic
and in good health.
Discussion
This study showed that a numb chin and a fat lip correlated with
malignancy more often than might otherwise be expected in as many
as 398 (72%) of 550 NCS patients. First mention of the syndrome of
the numb chin in the United States of America was in 1963 [2]. In
Spain, in 2008, it was reported that this symptom may be the first
manifestation of systemic cancer [6], a symptom of spread of an
established tumor, or a sign of infiltration in an intraoral lesion [6].
Moreover, in that study, 18 of 22 patients (82%) died before a mean
of 20 months after the initial presentation, further showing that
these symptoms are mostly indicative of very poor prognoses [6]. By
2014, only 6 years later, and as many as 83 cases had been reported
worldwide; and reported in Germany it was reported NCS was a
“rare” and often overlooked symptom of extracranial malignancies
[7].
Beginning in 1963 through 2018, 546 cases were reported around
the world in those 55 years, amounting to an average of 10 new
NCS cases being reported annually. Notwithstanding, Malaysia and
Japan reported the syndrome as seemingly rare in their countries but
manifesting malignancy and morbidity [8,9]. In Malaysia, following
a mastectomy for stage 2 breast carcinoma, a 51-year-old woman
presented with 2 weeks of bilateral lower limb pain and left chin
numbness. She was diagnosed with the NCS secondary to mandibular
tumour metastasis, started on palliative chemotherapy and radiation,
and eventually discharged with the only lingering complaint of a
numb chin [8]. In Japan, the oldest and youngest patients presenting
with NCS symptoms were a 73-year-old patient with prostate cancer
and an 18-year-old boy with Burkitt’s lymphoma/leukemia. They
both were reported as having succumbed to their illnesses in the
hospital [9].
Collectively these results, from 28 countries in this 57-year
longitudinal worldwide study of 186 articles in the medical literature
reporting NCS events and outcomes, could be important to
physicians with respect to performing further examinations to make
more accurate diagnoses and earlier treatment decisions for patients
presenting with the initial symptoms of the NCS. The study revealed
that patients presenting with a numb chin, intractable pain and a
thickening sensation of the lower lip, ought to be carefully followed up for fear of future maladies. Physicians in Germany, Japan, and
Italy, asked if this syndrome was a reflection of malignancy, an
immune-mediated disease, or a harbinger of medication-related
(e.g., bisphosphonate), osteonecrosis of the jaw and methotrexateassociated
lymphoproliferative disorders [7,10,11].
Even though the mechanism of this neurological phenomenon
of the numb chin remains unclear to date, and therefore often
controversial, a significant majority of cases have led to the comorbid
prognoses of malignancies, as evidenced in these 398 patients including
63 (11%) morbidities. In terms of perspective only, the 11% rate of
death for NCS patients is significantly higher than the worldwide
0.7% morbidity rate of patients affected with COVID-19. The NCS
deaths were those at the time of the published reports and therefore
do not indicate the actual number of morbidities to date. However,
with the poor prognoses of the hundreds of patients reported with
these malignancies, there were likely many more morbidities related
to the NCS throughout the world that went unreported. Further,
worthy of note, although there were 16 cases in Taiwan, there were
only 2 cases reported in China and no cases from Russia.
With hundreds of malignancies the world over, the NCS signs
and symptoms were revealed to be prodromal, the first manifestations
in many other severe and debilitating diseases. Of those, perhaps the
most debilitating is multiple sclerosis [7,12-15]. Fortunately, one
case of multiple sclerosis presenting with the symptoms of the NCS in
Germany was successfully treated with interferon-B [14]. In France,
a successful treatment with rituximab was reported in a patient
with mental nerve neuropathy in primary Sjogren’s syndrome, the
autoimmune disease often comorbid with other immune diseases,
especially rheumatoid arthritis and lupus [16]. In the USA, the NCS
was the initial presentation of a posttransplant lymphoproliferative
disorder [17]. In Italy, there were 3 cases of sudden violent, diffuse
pain in the premolar region reported [18]. In the USA, a patient
successfully underwent a transoral surgical resection of an elongated,
calcified, styloid process to relieve the mental nerve paresthesia and
pain caused by the dynamic compression of the alveolar inferior nerve
[19]. In Spain, the NCS was secondary to a solitary schwannoma [20]. And in Japan, a 39-year-old woman suffered a large solitary fibrous
tumor on the infratemporal fossa [21]. Thus, as is well evidenced,
all over the world, there have been and still are hundreds of cases of
NCS as the initial, primary sign of oncoming maladies, the degree of
severity of which becomes evident in time. Therefore, early diagnoses
and adequate treatment are often the difference between life or, if
neglected and undiagnosed, a possible lingering death to cancer – the
difference between remission-free survival or morbidity.
Burkitt lymphoma/leukemia is the most frequent subtype of
hematological malignancies in the NCS. It is highly aggressive and
often presents in extranodal sites and/or as acute lymphoblastic
leukemia. A leukemic phase can be observed in patients with
bulky disease, typically in males, and clearly present as leukemia
with peripheral blood and bone marrow involvement. In the 2016
revision of the fourth edition of the World Health Organization classification of myeloid neoplasms and acute leukemia, Burkitt
leukemia was classified as a subtype of Burkitt lymphoma [22].
Three epidemiological subtypes are recognized, which mainly differ
in geographic distribution. Endemic Burkitt lymphoma occurs in
equatorial Africa and Papua New Guinea, where the jaw and other face
bones are typically the sites of presentation in approximately 50%-
70% of those cases [23,24]. While not reported per se, it is conceivable
that NCS signs and symptoms are physical findings in endemic
Burkitt lymphoma patients. However, sporadic Burkitt lymphoma
and immunodeficiency-associated Burkitt lymphoma tumours in
facial structures, particularly in the jaw are rare. Furthermore, lytic
destruction of an area of bone due to myeloma and lymphoma
is a common symptom because leukemia and multiple myeloma
proliferates in the bone marrow. This explains the physiological
causality and neuropathic association that the NCS is often observed
in patients with various types of hematological malignancies.
In these 57 years, there were 29 reported cases of the numb
chin suspected of being an outright prodromal symptom of various
malignancies. However, as an example of the reverse occurring, a case
was reported of a 22-year-old man who after achieving a complete
5+year remission of CD+20 positive precursor B-ALL, presented with
gradually progressive altered mentation, slurring of speech, and chin
paresthesias over a 72-hour period [25]. His physical exam revealed
poor concentration, dysarthria, diminished sensation over the mental
area, and sialorrhea; however, the remainder of the examination was
unremarkable. There was another case, reported in 2015, of NCS
being the secondary symptom to cancer that had started from gastric
adenocarcinoma and metastasized to the brain as leptomeningeal
carcinomatosis [26]. All the other 548 cases in the present series
were of NCS being the first forewarning, an alarming-type symptom
of what usually turned out to be a malignant and/or metastasizing
disease. Sometimes for physicians unfamiliar with the NCS, these
symptoms were apparently not taken as a red flag or did not sound
an alarm and malignancies or debilitating diseases were manifested at
later stages in the patients’ prognoses.
Remarkably, of 550 cases, 150 (27%) were benign. Moreover,
in the course of compiling these data, it was conjectured that a
significant number of NCS cases worldwide must go unreported
and/or lost to follow-up. There were 10 articles that did not include
any numbers of patients but cautioned physicians about the various
aspects of the NCS and advised them to be on the lookout for these
symptoms. After a 55 year period with an average of 10 new NCS
cases reported annualy, the reporting of NCS cases seems to have
gone silent in 2019 because, to our knowledge, there were no new
cases reported until only one in 2020. That case was in Qatar, of a
30-year-old Indian man with acute myeloid leukemia who, after
being treated and discharged, returned to his home country and was
lost to follow-up [27]. The facts and outcomes of these 550 cases from
28 countries on all 6 continents from around the world, corroborate
those in 2014, in Germany, when it was reported that both benign and
malignant diseases cause the symptoms of this syndrome to flair up,
that there are many misdiagnoses, and, in a large majority of patients,
the symptoms often lead to a revelation of malignancy [7].
When a patient presents complaining of a numb chin, and/
or dysesthesis, fever, and a swelling sensation of the lower lip, the overwelming findings of this report will remind physicians to see
this set of signs and symptoms as “a red flag” and follow up with
sufficient examinations allowing them to make the right call in the
early stages of diseases to help mitigate pending threats. Therefore, we
hope that this study helps guide physicians to delve further into the
reaches of the human nervous system to elucidate the relationships
among the NCS, paralysis of the distal trigeminal nerve, leukemia,
lymphoma, bone, oral, brain, breast, and prostate cancer, metastatic
adenocarcinomas, and various other confounding, life-threatening
neuropathies and cytogenetic abnormalities.
Study limitations
For the purposes of compiling these data and “bean counting”
in this report, we have attempted to extrapolate any and all
duplicated cases in the literature. Likewise, in some articles, there
were omissions discovered wherein the exact data was not reported.
However imperfect, therefore, further quantitative and qualitative
considerations, which may logically and scientifically aply to these
data, can be made by each individual physician.
Conclusion
This 57-year, 28-country, worldwide study of 186 articles revealed
398 (72%) malignacies in 550 patients who suffered the fulminant,
fullblown symptoms of the NCS. Because significant evidence of
causuality remains elusive, this research opens up avenues for
future study, specifically, to examine how the NCS status affects
the prediction of numerous and seemingly unrelated maladies and
malignancies. With a closer look at this syndrome, early detection
may reduce long hospital stays for patients suffering with cancer, and
some deaths may be avoided.
Acknowledgements
We thank Michiel Brandt, MA, Monterey Institute of International
Studies, albeit posthumously, for her 30 years of being “high on life”
and her dedication and inspiration that made this study possible.
Her death was due to an 8-year bout with leukemia. We are also
greatly indebted to Takashi Katakura, PhD, of the Department of
Physiology, Kitasato University School of Medicine, for his technical
assistance.
References
Citation
Brandt RE, Takeuchi A, Kamata H. Numb Chin Syndrome: Diagnostic Significance Over 57 Years and Review of 550 Patients in the
Literature Worldwide. J Syndromes. 2020;5(1): 5.