
Special Issue: Plastic and Reconstructive Surgery
Review Article
*Address for Correspondence: Alessio Baccarani, MD FACS, Division of Plastic Surgery, Modena University Hospital, University of Modena and Reggio Emilia, Largo Pozzo 71, 41124 Modena, Italy, E-mail: alessio.baccarani@unimore.it
Citation: Baccarani A, De Santis G. Mandible Reconstruction: A Review Article. J Surgery. 2015; S(1): 7.
Copyright © 2015 Baccarani A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Special Issue: 1
Submission: 31 March 2015 | Accepted: 02 June 2015 | Published: 06 June 2014

 The goals of oromandibular reconstruction, the restoration of form and function, have not changed. The restoration of form has long been achieved with osteocutaneous free flap reconstruction predictably producing mandible continuity with living bone. Surgeons can expect similar or even improved postoperative appearance even after large resections. Functional results have not been as good as did morphology, despite the fact that highly functional outcomes have been routinely delivered for decades. Optimal restoration of function involves mastication, deglutition and the management of oral secretions. The return of adequate mouth opening, intraoral lubrication and sensation in the mouth and in the distribution of the mental nerve are necessary. The soft tissue replacements with skin or mucous membrane need to be thin and pliable enough that they do not inhibit the mobility of the remaining oral and pharyngeal structures such as the tongue and the palate. Dentition can now be reliably restored with osseointegrated implants. No current single technique can restore sensation and lubrication, but a combination of flaps can now approach almost complete functional restoration.
The goals of oromandibular reconstruction, the restoration of form and function, have not changed. The restoration of form has long been achieved with osteocutaneous free flap reconstruction predictably producing mandible continuity with living bone. Surgeons can expect similar or even improved postoperative appearance even after large resections. Functional results have not been as good as did morphology, despite the fact that highly functional outcomes have been routinely delivered for decades. Optimal restoration of function involves mastication, deglutition and the management of oral secretions. The return of adequate mouth opening, intraoral lubrication and sensation in the mouth and in the distribution of the mental nerve are necessary. The soft tissue replacements with skin or mucous membrane need to be thin and pliable enough that they do not inhibit the mobility of the remaining oral and pharyngeal structures such as the tongue and the palate. Dentition can now be reliably restored with osseointegrated implants. No current single technique can restore sensation and lubrication, but a combination of flaps can now approach almost complete functional restoration.
Review Article
Mandible Reconstruction: A Review Article
Alessio Baccarani* and Giorgio De Santis
- Division of Plastic Surgery, Modena University Hospital, University of Modena and Reggio Emilia, Modena, Italy
*Address for Correspondence: Alessio Baccarani, MD FACS, Division of Plastic Surgery, Modena University Hospital, University of Modena and Reggio Emilia, Largo Pozzo 71, 41124 Modena, Italy, E-mail: alessio.baccarani@unimore.it
Citation: Baccarani A, De Santis G. Mandible Reconstruction: A Review Article. J Surgery. 2015; S(1): 7.
Copyright © 2015 Baccarani A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Special Issue: 1
Submission: 31 March 2015 | Accepted: 02 June 2015 | Published: 06 June 2014
Keywords
Computer-generated modeling; Free flaps; Mandible reconstruction; OsteonecrosisIntroduction
Segmental mandibular defects can result from trauma, infection, tumor resection or osteoradionecrosis. Reliable long-term restoration of mandibular continuity, necessary for the return of predictable form and function, demands that viable bone replace the segmental defect. Form and function restoration implies preservation of all oral functions including speech, and capability of processing food. Morphologically the mandible defines the contour of the lower third of the face. For the past 33 years, the technique that has produced the most efficient, most reliable and most cost effective method for replacing segmental mandibular defects has been free tissue transfer of osseous and osteocutaneous free flaps. Due to the mobile, contaminated and frequently radiated surgical bed, no other techniques have been as successful or timely.Established and Current Concepts – A Review of the Literature
Much has been written over the years about multistaged techniques employing pedicled and even free soft tissue flaps supporting a neomandibular scaffold. These flaps isolate the contaminated oral cavity and at second surgeries, often after hyperbaric oxygen regimens, are filled with cancellous bone grafts from the iliac crest with or without bone morphogenic proteins. Once new bone forms, osseointegrated implants are placed at a third surgery. This process involves multiple surgeries over months with repeated hospitalizations. The resulting neomandible can be an excellent replacement for the missing mandible segment, but the time is long and the costs are high in a patient population dominated by cancer and almost always radiation therapy.The alternative of a one-stage cancer removal, immediate reconstruction of the missing mandible with vascularized bone and placement of osseointegrated implants during a single anesthesia has proven to be more reliable and much more cost effective, despite potential obscuring residual disease and delay in its recognition. What has evolved is the choice of which free osseous or osteocutaneous flap to employ. Taylor et al. described the iliac crest microvascular free flap for just this reconstruction in 1979 [1]. The flap was reliable and the bone stock could be harvested to closely mimic the mandible in size and shape. The vascular pedicle was relatively short, the cutaneous paddle carried on a mesentery of abdominal muscles was often unwieldy for intraoral use and the donor morbidity was significant. Still, this was a game-changing technique as it was shown to be vastly superior to all other techniques previously employed. The bone stock is adequate to reliably accept osseointegrated implants.
The 1980s saw the introduction of the radial forearm flap incorporating a partial thickness segment of the radius [2] and the scapula osteocutaneous flap employing the lateral border of the scapula [3]. The amount of radius bone available was a poor match to any segmental mandibular defect, with insufficient bone stock to accept osseointegrated implants, and the potential donor morbidity was significant. The scapula composite flap provided 11–14 cm of bone with two large, thin and easily manipulated skin paddles. The bone stock is marginal for reliable placement of osseointegrated implants. Patient positioning is tedious for synchronous cancer ablation and flap harvest, but the donor morbidity for scapular flap is substantially less than seen with the iliac crest or the radius.
The fibula flap was also introduced by Taylor et al. in 1975 forlong bone reconstruction [4]. It was first described for oromandibular reconstruction by Hidalgo in 1989 [5]. This incredibly versatile osteocutaneous free flap can provide up to 25 cm of dense cortical bone and skin paddles as large as 10 × 20 cm. The bone stock is excellent for reliable placement of osseointegrated implants. Dr Barber described the placement of osseointegrated implants at the initial surgery in 1990 [6]. The thin and pliable skin paddle can also be harvested as a neurosensory flap and an additional vascularized nerve graft can be included with the flap [7]. Multiple skin paddles can be harvested with this flap, including those based on septocutaneous and also on musculocutaneous peroneal perforators [8]. This flap has been our primary choice for oromandibular reconstruction for 22 years, as it now is for almost all reconstructive surgeons. Of the fourosteocutaneous flaps, it has the lowest significant complication rate.
Early complaints about the fibula flap were largely about the limited height of the reconstructed mandible, which then required long abutments on the osseointegrated implants, increasing the risk of cantilever forces and subsequent implant failure. These authors had always placed the fibula bone at the basilar aspect of the mandible defect. Vertical distraction osteogenesis has been utilized to increase the height of the fibular segment, but is expensive, time consuming and technically challenging. We have employed simpler techniques to circumvent this problem in more than 270 fibula reconstructions. The fibula replacement can be located more superiorly in the mandible defect or can be double barreled [9,10]. Both of these techniques result in insignificant height discrepancies with the native mandible optimizing dental rehabilitation and maintaining aesthetic facial contours (Figures 1 and 2). He et al. reviewed a small series of seven patients reconstructed for segmental mandibular defects with the double-barrel fibular flap and dental rehabilitation in 2011 [11]. Prosthodontic treatment was completed in all patients. Four patients received secondary implant-supported dental reconstruction, and three patients who received radiation after graft surgery had conventional removable partial dentures. In this series, the fibula graft had a reconstructed height of 3–3.8 cm, which matched the native mandibular height, which the authors suggest may result in better aesthetics and function.
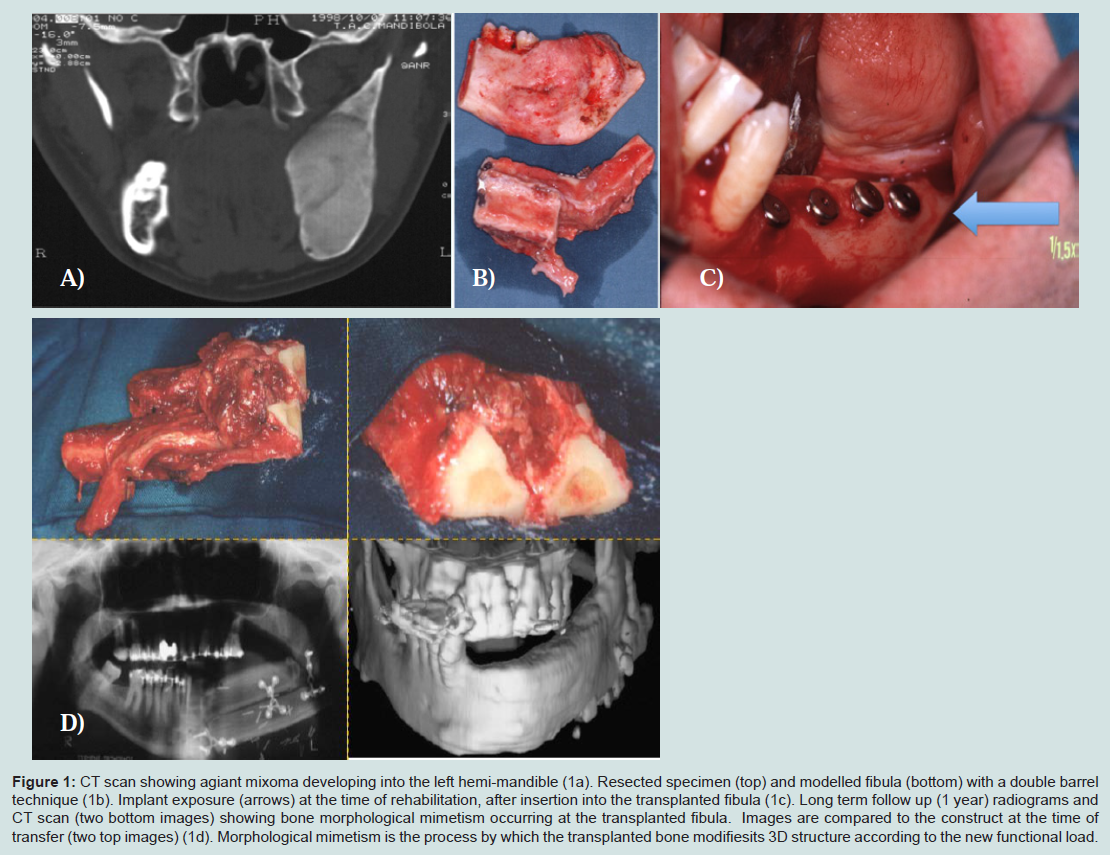
Figure 1: CT scan showing agiant mixoma developing into the left hemi-mandible (1a). Resected specimen (top) and modelled fibula (bottom) with a double barrel technique (1b). Implant exposure (arrows) at the time of rehabilitation, after insertion into the transplanted fibula (1c). Long term follow up (1 year) radiograms and CT scan (two bottom images) showing bone morphological mimetism occurring at the transplanted fibula. Images are compared to the construct at the time of transfer (two top images) (1d). Morphological mimetism is the process by which the transplanted bone modifiesits 3D structure according to the new functional load.
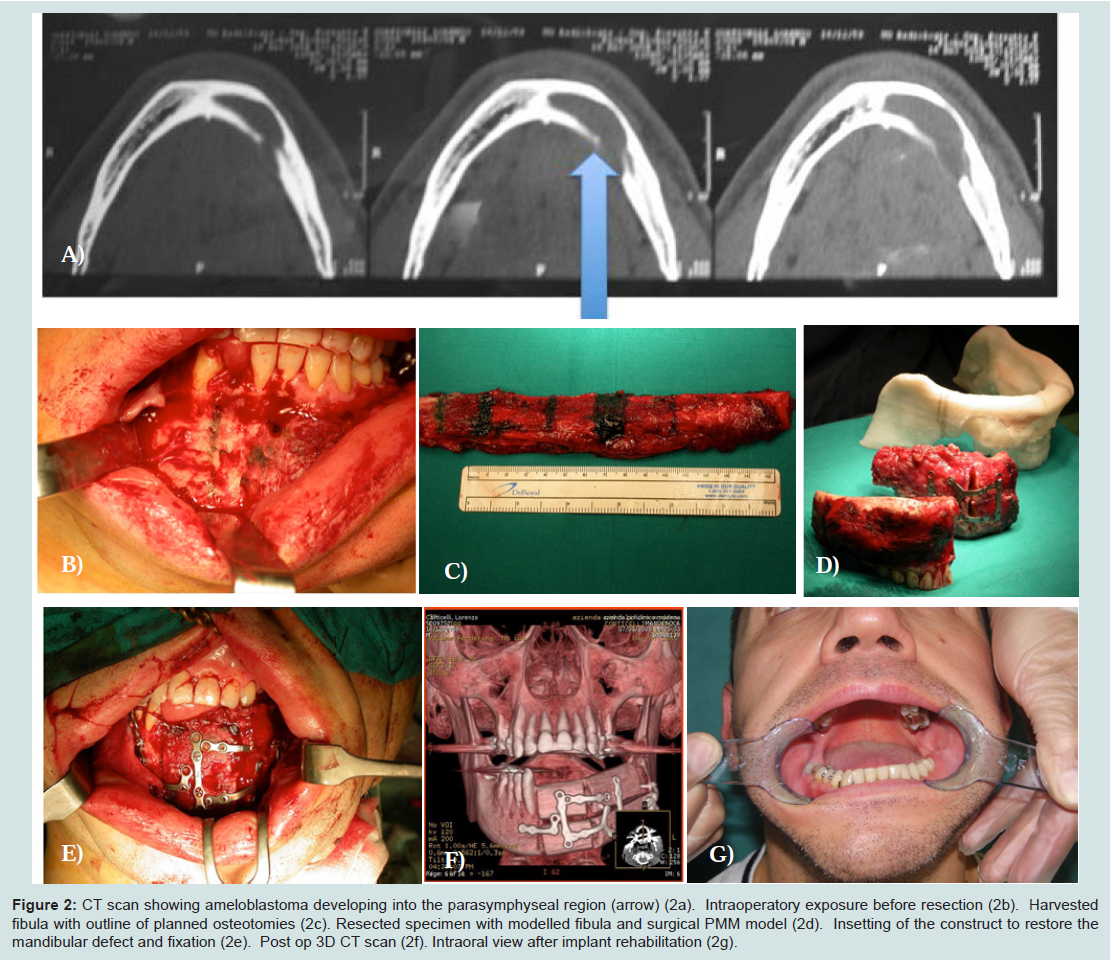
Figure 2: CT scan showing ameloblastoma developing into the parasymphyseal region (arrow) (2a). Intraoperatory exposure before resection (2b). Harvested fibula with outline of planned osteotomies (2c). Resected specimen with modelled fibula and surgical PMM model (2d). Insetting of the construct to restore the mandibular defect and fixation (2e). Post op 3D CT scan (2f). Intraoral view after implant rehabilitation (2g).
Remember that not all mandible surgery requires a segmental mandibulectomy even for cancer ablation. Marginal mandibulectomy is often sufficient oncologically and can save a patient additional reconstructive surgery. Also, very small segmental defects, especially of the body of the mandible, can often be reconstructed with nonvascularized bone grafts (NVBGs) as long as radiation therapy is not included. However, the focus of this review is on larger defects, most often after cancer ablation and radiation therapy. Osteocutaneous free flaps are the primary choices for the best functional and aesthetic outcome for these patients. If performed with the ablation, this reconstruction will provide the quickest and most successful rehabilitation with the shortest operative time. Large complex oromandibular defects deserve immediate reconstruction with vascularized osteocutaneous flaps and osseointegrated implants placed primarily in one surgery under one anesthesia. In the past 2 years, we found nearly 100 articles available through PubMed focusing on current and advancing concepts in mandibular reconstruction. These articles represent the integration of technology into medical practice and can be grouped into several broader categories as depicted in the following review.
Virtual Surgical Planning using Computer-Assisted Modeling
The first introduction of three-dimensional planning in craniofacial surgery was described by Cutting et al. [12]. In recent years, perhaps the most represented topic in the literature regarding segmental mandibular reconstruction is that of computer-assisted modeling. With this technique, stereolithographic models of the patient’s mandible and fibula are created based on three-dimensional computed tomography scans. Computer analysis then determines the optimal location for both the mandibular osteotomies and the fibular osteotomies, and templates are created to be used intraoperatively. The accuracy of bony alignment of the neomandible then no longer relies strictly on the surgeon’s intraoperative manual approximation, and the dimensions of the neomandible and degree of bone-on-bone contact are optimized healing and subsequent function.The fibula is a straight bone. Because a defect of the lateral body of the mandible is a straight defect, the defect is easily replaced with the fibula. However, an anterior mandibular defect is much more complicated because the curved defect must now be replaced by a straight bone. For an optimal aesthetic result, the external contour of the jaw should be maintained. But for optimal dental rehabilitation, alveolar alignment with the upper jaw is essential. It is critical to remember that the alveolar portion is mesial to the basilar portion of the lateral mandible and posterior to the mentum anteriorly. It is critical that the fibula bone segments and the segments of the remaining mandible be in precise apposition. This can be a very timeconsuming and arduous process. Moreover the symphyseal region is essential in preserving tongue movements, and the soft tissue reattachment to the fibula consequently critical.
Hirsch et al. provide a concise overview of computer-aided virtual surgical planning [13]. The creation of staged models, created based on three-dimensional imaging and used intraoperatively to make accurate extirpative cuts on the mandible, ostectomies in the fibulaand prebending of the reconstructive plate, is detailed clearly.
Roser et al. looked into the accuracy of computer-assisted planning by comparing the virtually planned with the actual reconstruction by superimposing three-dimensional scans [14]. For the 11 fibulas in the study, the mean percentage of volumes of the postoperative fibula compared with the virtually planned fibula was 90.93 ± 18.03%, the mean distance of the actual fibula osteotomy when compared with the virtual osteotomy was 1.30 ± 0.59 mm, and the mean percentage overlap of the reconstruction plate to the virtual plate was 58.73 ± 8.96%. Hence, the accuracy of the mandibular and fibular osteotomies was quite high; however, a limited ability to recreate the plate template by hand was noted.
Hou et al. describe seven patients in whom computer modeling was employed to create prefabricated titanium mesh used in conjunction with a fibula-free flap, arguing improved re-creation of the mandibular shape and improved operative time [15].
Another interesting article comes from Juergens et al., who introduce a novel method of flap harvest [16]. Using newly developed software and mathematical algorithms, the ideal donor site in the iliac crest is identified and subsequently transferred to the patient in the operative room via a developed three-dimensional real-time intraoperative navigation prototype system.
There have been numerous articles about the computer-assisted techniques and stereolithographic models and the benefits of the technology. However, few have described outcomes and none have compared these methods with results of other techniques used by experienced surgeons. Although exciting and sometimes time saving, this technology is costly and further research is needed before widespread use will follow.
New Flap Designs and Harvest
Vacher and Lkah described their experience with the pedicled osteomuscular dorsal scapular flap [17]. This flap is pedicled on the dorsal scapular vessels with the harvest of the medial border of the scapula and the lateral portion of the rhomboid musculature. It produces a pedicled osteomuscular flap with a thin (less than 4 mm thick) piece of medial scapula, which can be 11–12 cm long. The pedicle length is short at 6–7 cm, only allowing reconstruction of lateral mandible defects with this flap. This is a significant contribution to theflap armamentarium, similar to the lateral trapezius osteocutaneous pedicled flap in the late 1970’s. But with preservation of the spinal accessory nerve, this flap does not have the trapezius morbidity of loss of shoulder function. Be aware that, in patients with previous neck dissections, the dorsal scapular vessels may not be available.Another novel option has been introduced by Hanasono and Skoracki who present seven patients with peripheral vascular disease and anterior segmental defects, reconstructed with the scapular tip [18]. The flap is based on the angular branch of the thoracodorsal artery, can reliably supply 20 cm of bone from both the medial and lateral aspects of the scapula and a pedicle length of up to 17 cm if the subscapular vessels are included. In their technique, the flap is inset transversely in a tongue-in-groove fashion to the remaining native mandible and secured with titanium plates. Drawbacks include the patient positioning required for a two team approach, deficient vertical height of the neomandible and inadequate bone stock of the scapula tip for osseointegrated implants.
Although first introduced by Green et al. in 1981, the pectoralis major pedicled flap with vascularized sternum has been essentially lost in the era of free tissue transfer [19]. It has been reintroduced recently by Selber and Ghali as another viable option in patients who are poor candidates for free tissue transfer [20]. With this technique, the medial anterior table of the ipsilateral lower third of the sternum is incorporated into the pectoralis major flap. This represents a fallback technique for the compromised patient.
Regarding flap harvest, Chang et al. looked in to the effect of ischemia time on the outcome of free fibula flaps [21]. In this study, 114 patients with similar risk factors for flap failure (age, BMI, smoking, ETOH, radiation history, diabetes) underwent 116 freefibula flaps. Outcomes among different ischemia time groups were evaluated. The overall complication rate was 57%, whereas in the subcohort with ischemia time over 5 h, this increased to 82% along with a statistically significant higher rate of partial flap loss relative to the other groups. Although this subcohort had a smaller ratio of mean number of perforators to mean skin paddle size, it was suggested that a critical ischemia time of 5 h be implemented based on a lack of increased complications with ischemia times less than 5 h.
Articles are still being published promoting the use of NVBGs instead of vascularized bone transfer. Gadre et al. in 2011 present a long-term retrospective study of 166 patients who had undergone mandibular ablation, of which 101 were reconstructed with NVBGs, 27 with vascularized bone grafts and 38 with functional plate reconstruction [22]. Eighty-seven of 101 patients with NVBGs who had a minimum period of f/u of 1 year were included. The overall success rate was 77 (88.5%) of 87. Ilium was used in 68 cases (78.16%), fibula in 16 cases (18.39%) and rib in three cases (3.44%). Ten cases (11%) showed complete failure due infection (seven cases) and resorption (three cases). The authors conclude that NVBG can be used judiciously for reconstruction of selected mandibular defects without significant soft tissue loss, or where two-layer watertight closure can be achieved intraorally and extraorally. The authors review the difficulties of performing vascularized bone grafts in developing countries such as India due to economic reasons, shortage of trained manpower and limited hospital resources and suggest that NVBG is still an accepted method of reconstruction in the developing world. The short follow-up and the relatively low representation of radiation therapy make it hard to predict a comparable long-term success rate to the high 90% seen almost universally with vascularized bone transfer.
Matsuo et al. in 2011 present a study of the bone quality of mandibles reconstructed with particulate cellular bone and marrow (PCBM) and platelet-rich plasma (PRP) evaluated at the time of dental implant placement [23]. Bone mineral density and microstructure of PCBM-reconstructed and PRP-reconstructed bone were compared to normal bone. Eleven samples were taken from five patients who had undergone mandibular reconstruction with PCBM and PRP. Biopsies were performed using a standardized bone biopsy technique with trephine bur. As controls, 16 biopsies were obtained from normal mandibular bone. Microcomputed tomogrpahy scanning and bone mineral density were measured, and histology performed. Results revealed that the compact bone in the PCBM group was extremely thin, and that the trabecular structure of the cancellous bone in both groups (PCBM/PRP and normal bone) was similar.
Kokemueller et al. present a research article using a sheep model for prefabrication of vascularized bioartificial bone grafts in vivo [24]. Two cylindrical beta-TCP (beta-tricalcium phosphate) scaffolds were intraoperatively filled with autogenous bone marrow from the iliac crest and implanted into the latissimus dorsi muscle, one with a surgically supplied central vascular bundle to assess the effect of axial perfusion. At 3 months, sheep were sacrificed and histomorphometric analysis revealed considerable ectopic bone growth in all scaffolds with bone growth, ceramic resorption and angiogenesis increased significantly with axial perfusion. Clinical application was presented of a man with loss of a left hemimandible. The procedure was performed with three iliac crest bone biopsies harvested and morselized with an electric bone mill and four blood-soaked cylinders supplied with central vascular bundle from dissection of the latissimus dorsi thoracodorsal trunk. Six months later, bone grafts were explanted and shaped using piezosurgery according to a virtual template preoperatively created using computer software. A titanium mesh was used to create a bowl that was filled with the bone grafts and stabilized to the mandible. Twelve months after surgery there were no signs of infection or rejection. This is an interesting research article, but the single clinical case presented is another example of a very prolonged multistaged surgical option, which ultimately transfers a NVBG.
Distraction Osteogenesis
The use of distraction osteogenesis for segmental mandibular defects is limited at this time. In cancer cases, there is usually resection of soft tissue and periosteum and often adjuvant radiation therapy. These are both relative contraindications for distraction osteogenesis. Sacco and Chepeha compiled an excellent review on this topic in 2007 [25]. Since then, there have been a number of small series describing success with transport-disk distraction osteogenesis.In 2010, Chen et al. used a two-step transport-disk distraction technique with internal distracters to reconstruct body or ramus defects in both horizontal and vertical dimensions [26]. These patients all had benign odontogenic tumors, which allowed preservation of periosteum and no required radiation. Also, the distraction requires 14–18 months of treatment.
Seitz et al. reported in 2010 on a series of seven patients with segmental defects after composite resections for oral cavity squamous cell carcinoma [27]. The initial reconstruction used soft tissue flaps and reconstructive bridging plates. At an average 20 months later, transport disk distraction osteogenesis was performed with an external fixator. One patient received radiotherapy and had insufficient callus formation. The other six patients had successful bony reconstruction.
Although distraction osteogenesis has been successful in the reconstruction of large segmental defects, its application is limited by a requirement for intact soft tissue and periosteum, an incompatibility with adjuvant radiotherapy and the need for a long period of treatment.
Osteoradionecrosis
Osteoradionecrosis, as a consequence of radiation therapy, presents a difficult reconstructive challenge. The significant damage to the microvasculature of all of the tissues in the radiation field leads to greater failure and complication rates of reconstruction. Recently, two large series have been published that further our understanding of the issues in the treatment of this serious complication.In 2009, Alam et al. reported a 9% rate of recurrent radionecrosis in a series of 33 patients, undergoing microsurgical reconstruction [28]. They had a high surgical complication rate (39%) but still cured 94% of patients.
Suh et al. reported in 2010 that 25% of 40 patients with osteoradionecrosis developed residual or recurrent osteonecrosis, after microsurgical flap reconstruction [29]. The majority of these were in the adjacent condyle. They reason that the dense cortical nature of the condyle makes assessment of bleeding more difficult. They believe that the condyle should be resected if it has received the same dose of radiation as the necrotic segment even if it appears to be clinically and radiographically healthy.
Mandibular reconstruction for bisphosphonate-related osteonecrosis of the jaw is a controversial subject. The patients who receive high dose intravenous bisphosphonates are usually those with bony metastases or multiple myeloma. With greater systemic disease and unknown effects of the bisphosphonates on donor bones and recipient mandible, these patients present a greater challenge for mandible reconstruction, requiring more extensive surgical resection and reconstruction [30,31]. Nocini et al. describe a series of seven patients who received subtotal mandibulectomies (average 18.5 cm) and fibular flap reconstructions [30]. With a mean follow-up of 23 months, only one patient had a recurrence of osteonecrosis.
Conclusion
Successful reconstruction of the segmental mandibular defect depends on the restoration of vascularized bone and the surrounding soft tissues. To date, the most reliable reconstruction is achieved with vascularized free flaps, with the fibula flap being the most popular. The more than 20-year experience developed at our institution with microsurgical reconstruction has led us to consider the fibula the procedure of choice. Techniques continue to evolve to improve both form and function.References
- Taylor GI, Townsend P, Corlett R (1979) Superiority of the deep circumflex iliac vessels as the supply for free groin flaps. Plast Reconstr Surg 64: 595-604.
- Soutar DS, Scheker LR, Tanner NS, McGregor IA (1983) The radial forearm flap: a versatile method for intra-oral reconstruction. Br J Plast Surg 36: 1-8.
- Swartz WM, Banis JC, Newton ED, Ramasastry SS, Jones NF, et al. (1986) The osteocutaneous scapular flap for mandibular and maxillary reconstruction. Plast Reconstr Surg 77: 530-545.
- Taylor GI, Miller DH, Ham FJ (1975) The free vascularized bone graft: A clinical extension of microvascular techniques. Plast Reconstr Surg 55: 533-544.
- Hidalgo DA (1989) Fibula free flap: a new method of mandible reconstruction. Plast Reconstr Surg 84: 71-79.
- Barber HD, Seckinger RJ, Hayden RE, Weinstein GS (1995) Evaluation of osseointegration of endosseous implants in radiated, vascularized fibula flaps to the mandible: a pilot study. J Oral Maxillofac Surg 53: 640-644.
- O’Leary MJ, Martin PJ, Hayden RE (1994) The neurocutaneous free fibula flap in mandibular reconstruction. Otolaryngol Clin North Am 27: 1081-1096.
- Daya M (2008) Peroneal artery perforator chimeric flap: changing the perspective in free fibula flap use in complex oromandibular reconstruction. J Reconstr Microsurg 24: 413-418.
- Chang YM, Tsai CY, Wei FC (2008) One-stage, double-barrel fibula osteoseptocutaneous flap and immediate dental implants for functional and aesthetic reconstruction of segmental mandibular defects. Plast Reconstr Surg 122: 143-145.
- Bahr W, Stoll P, Wachter R (1998) Use of the “double barrel” free vascularized fibula in mandibular reconstruction. J Oral Maxillofac Surg 56: 38-44.
- He Y, Zhang Z, Zhu H, Wu YQ, Fu HH (2011) Double-barrel fibular vascularized free flap with dental rehabilitation for mandibular reconstruction. J Oral Maxillofac Surg 69: 2663-2669.
- Cutting C, Bookstein FL, Grayson B, Fellingham L, McCarthy JG (1986) Three-dimensional computer-assisted design of craniofacial surgical procedures: optimization and interaction with cephalometric and CT-based models. Plast Reconstr Surg 77: 877-887.
- Hirsch DL, Garfein ES, Christensen AM, Weimer KA, Saddeh PB, et al. (2009) Use of computer-aided design and computer-aided manufacturing to produce orthognathically ideal surgical outcomes: a paradigm shift in head and neck reconstruction. J Oral Maxillofac Surg 67: 2115-2122.
- Roser SM, Ramachandra S, Blair H, Grist W, Carlson GW, et al. (2010) The accuracy of virtual surgical planning in free fibula mandibular reconstruction: comparison of planned and final results. J Oral Maxillofac Surg 68: 2824-2832.
- Hou JS, Chen M, Pan CP, Tao Q, Wang JG, et al. (2011) Immediate reconstruction of bilateral mandible defects: management based on computer-aided design/computer-aided manufacturing rapid prototyping technology in combination with vascularized fibular osteomyocutaneous flap. J Oral Maxillofac Surg 69: 1792-1797.
- Juergens P, Klug C, Krol Z, Beinemann J, Kim H, et al. (2011) Navigation-guided harvesting of autologous iliac crest graft for mandibular reconstruction. J Oral Maxillofac Surg 69: 2915-2923.
- Vacher C, Lkah C (2010) The osteomuscular dorsal scapular (OMDS) flap: an alternative technique of mandibular reconstruction. J Plast Reconstr Aesthet Surg 63: 198-204.
- Hanasono MM, Skoracki RJ (2010) The scapular tip osseous free flap as an alternative for anterior mandibular reconstruction. Plast Reconstr Surg 125: 164e-165e.
- Green MF, Gibson JR, Bryson JR, Thomson E (1981) A one-stage correction of mandibular defects using a split sternum pectoralis major osteo-musculocutaneous transfer. Br J Plast Surg 34: 11-16.
- Selber JC, Ghali S (2012) Pectoralis major flap with sternum: achieving vascularized osseous reconstruction of the mandible without a free flap. Plast Reconstr Surg 129: 389e-391e.
- Chang SY, Huang JJ, Tsao CK, Nguyen A, Mittakanti K, et al. (2010) Does ischemia time affect the outcome of free fibula flaps for head and neck reconstruction? A review of 116 cases. Plast Reconstr Surg 126: 1988-1995.
- Gadre PK, Ramanojam S, Pantakar A, Gadre KS (2011) Nonvascularized bone grafting for mandibular reconstruction: myth or reality? J Craniofac Surg 22: 1727-1735.
- Matsuo A, Chiba H, Takahashi H, Toyoda J, Hasegawa O, et al. (2011) Bone quality of mandibles reconstructed with particulate cellular bone and marrow, and platelet-rich plasma. J Craniomaxillofac Surg 39: 628-632.
- Kokemueller H, Spalthoff S, Nolff M, Tavassol F, Essig H, et al. (2010) Prefabrication of vascularized bioartificial bone grafts in vivo for segmental mandibular reconstruction: experimental pilot study in sheep and first clinical application. Int J Oral Maxillofacial Surg 39: 379-387.
- Sacco AG, Chepeha DB (2007) Current status of transport-disc-distraction osteogenesis for mandibular reconstruction. Lancet Oncol 8: 323-330.
- Chen J, Liu Y, Ping F, Zhao S, Xu X, et al. (2010) Two-step transport-disk distraction osteogenesis in reconstruction of mandibular defect involving body and ramus. Int J Oral Maxillofacial Surg 39: 573-579.
- Seitz O, Harth M, Ghanaati S, Lehnert T, Vogl TJ, et al. (2010) Secondary mandibular reconstruction after oral squamous cell carcinoma resection: clinical reevaluation of transport disk distraction osteogenesis. J Craniofac Surg 21: 59-63.
- Alam DS, Nuara M, Christian J (2009) Analysis of outcomes of vascularized flap reconstruction in patients with advanced mandibular osteoradionecrosis. Otolaryngol Head Neck Surg 141: 196-201.
- Suh JD, Blackwell KE, Sercarz JA, Cohen M, Liu JH, et al. (2010) Disease relapse after segmental resection and free flap reconstruction for mandibular osteoradionecrosis. Otolaryngol Head Neck Surg 142: 586-591.
- Nocini PF, Saia G, Bettini G, Ragazzo M, Blandamura S, et al. (2009) Vascularized fibula flap reconstruction of the mandible in bisphosphonate-related osteonecrosis. Eur J Surg Oncol 35: 373-379.
- Baccarani A, Follmar KE, Erdmann D, Levin LS (2013) Face transplantation surgical options and open problems in cadaveric models: a review article. Microsurgery 33: 239-246.