
Special Issue: Plastic and Reconstructive Surgery
Case Report
*Address for Correspondence: Ekkehard M. Kasper, MD, PhD, FAANS, Assistant Professor of Surgery, Division of Neurosurgery, Beth Israel Deaconess Medical Center, Harvard Medical School, 110 Francis street, Lowry Medical Office Building, Suite 3B, Boston, MA 02215, USA, Tel: 617 632 7246; Fax: 617 632 0949; E-mail: ekasper@bidmc.harvard.edu
Citation: Bayoumi AB, Ohla V, Lin SJ, Frankenthaler RA, Zimarowski MJ, et al. Single Stage Multidisciplinary Treatment of Recurrent Scalp Dermatofibrosarcoma Protuberans. J Surgery. 2014; S(1): 7.
Copyright © 2014 Bayoumi AB, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Special Issue: 1
Submission: 07 May 2014 | Accepted: 19 May 2014 | Published: 23 May 2014
Editor:Dr. Abdou Mohammed Abd Allah Darwish, Head of the Department of Plastic & Reconstructive Surgery Minia University, Egypt
 Operative details
Operative details
 The plastic surgeons started at the donor site with a curvilinear incision which was made at the level of the axilla in order to visualize thoracodorsal perforators and the serratus anterior muscle. Thoracodorsal perforator vessels were visualized and measures of the usual landmarks taken; however, it was noted that this rather large scalp defect was not amenable to thoracodorsal perforator flap. A serratus flap was therefore elevated in standard fashion from underneath the latissimus muscle. The inferior four slips were taken from the serratus muscle, preserving the upper slips of the muscle attached to the scapula. The vascular pedicle was preserved at all times and carried nearly to the subscapular system, and the thoracodorsal branches were divided. Meanwhile, the superficial temporal artery (STA) and vein (STV) were identified and dissected free in a separate surgical field in a standard fashion. These vessels were prepared for microsurgical anastomoses. Following the preparation of the STA and STV, the pedicle was divided inferiorly and the serratus muscle flap was transferred up to the head and neck region. The anastomosis was performed with 9-0 nylon sutures in an interrupted fashion and a 2.0 venous coupler was used for the vein. The flap was then inserted with horizontal mattress sutures with 3-0 Vicryl suture.
The plastic surgeons started at the donor site with a curvilinear incision which was made at the level of the axilla in order to visualize thoracodorsal perforators and the serratus anterior muscle. Thoracodorsal perforator vessels were visualized and measures of the usual landmarks taken; however, it was noted that this rather large scalp defect was not amenable to thoracodorsal perforator flap. A serratus flap was therefore elevated in standard fashion from underneath the latissimus muscle. The inferior four slips were taken from the serratus muscle, preserving the upper slips of the muscle attached to the scapula. The vascular pedicle was preserved at all times and carried nearly to the subscapular system, and the thoracodorsal branches were divided. Meanwhile, the superficial temporal artery (STA) and vein (STV) were identified and dissected free in a separate surgical field in a standard fashion. These vessels were prepared for microsurgical anastomoses. Following the preparation of the STA and STV, the pedicle was divided inferiorly and the serratus muscle flap was transferred up to the head and neck region. The anastomosis was performed with 9-0 nylon sutures in an interrupted fashion and a 2.0 venous coupler was used for the vein. The flap was then inserted with horizontal mattress sutures with 3-0 Vicryl suture.

 Some histopathological variants reported in the literature include fibrosarcomatous DFSP, myxoid variant, and Bednar tumor. Fibrosarcomatous types show less immunoreactivity to CD34 in the sarcomatous areas with higher risk of local recurrence [5]. The myxomatous variant shows little cytologic pleomorphism and low mitotic rate with pale basophilic stromal staining positive for alcian blue stain [4]. In Bednar tumor, there are melanin-containing dendritic cells scattered throughout the tumor representing the pigmented DFSP variant [3].
Some histopathological variants reported in the literature include fibrosarcomatous DFSP, myxoid variant, and Bednar tumor. Fibrosarcomatous types show less immunoreactivity to CD34 in the sarcomatous areas with higher risk of local recurrence [5]. The myxomatous variant shows little cytologic pleomorphism and low mitotic rate with pale basophilic stromal staining positive for alcian blue stain [4]. In Bednar tumor, there are melanin-containing dendritic cells scattered throughout the tumor representing the pigmented DFSP variant [3].
Case Report
Single Stage Multidisciplinary Treatment of Recurrent Scalp Dermatofibrosarcoma Protuberans
Ahmed B. Bayoumi1, Victoria Ohla5, Samuel J. Lin2,3, Robert A. Frankenthaler3, Mary Jane Zimarowski4 and Ekkehard M. Kasper1*
- 1Division of Neurosurgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA
- 2Division of Plastic Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA
- 3Division of Otolaryngology, Department of Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA,USA
- 4Department of Pathology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA
- 5Department of Neurosurgery, Freiburg, Germany
*Address for Correspondence: Ekkehard M. Kasper, MD, PhD, FAANS, Assistant Professor of Surgery, Division of Neurosurgery, Beth Israel Deaconess Medical Center, Harvard Medical School, 110 Francis street, Lowry Medical Office Building, Suite 3B, Boston, MA 02215, USA, Tel: 617 632 7246; Fax: 617 632 0949; E-mail: ekasper@bidmc.harvard.edu
Citation: Bayoumi AB, Ohla V, Lin SJ, Frankenthaler RA, Zimarowski MJ, et al. Single Stage Multidisciplinary Treatment of Recurrent Scalp Dermatofibrosarcoma Protuberans. J Surgery. 2014; S(1): 7.
Copyright © 2014 Bayoumi AB, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Special Issue: 1
Submission: 07 May 2014 | Accepted: 19 May 2014 | Published: 23 May 2014
Editor:Dr. Abdou Mohammed Abd Allah Darwish, Head of the Department of Plastic & Reconstructive Surgery Minia University, Egypt
Abstract
Background: Dermatofibrosarcoma protuberans (DFSP) is a rare soft tissue tumor that may affect the trunk, proximal extremities and less frequently the scalp.Methods: A 25-year-old Hispanic male presented with a large recurrent left sided scalp lesion. A wide margin soft tissue resection was done followed by craniectomy and allograft cranioplasty with deep margin resection and autologous duraplasty. Skull reconstruction was done. The scalp defect was closed by a serratus anterior myofascial free flap and a split thickness graft from the thigh.
Results: Over a 5-year follow up period, there was no evidence of local recurrence, distant spread, infections or neurological deficit. The only visible effect noted was alopecia at the surgical site.
Conclusions: A single-stage complex surgical excision and reconstruction may represent the safest and most effective option in the management of recurrent scalp DFSP with improved outcomes including minimal morbidity and prolonged recurrence free survival or cure.
Keywords
Dermatofibromasarcoma protuberans; Multidisciplinary; Single stage; Complex reconstruction; Skull tumorsIntroduction
Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, slowly growing mesenchymal tumor that arises primarily from the dermis, but frequently invades the underlying subcutaneous tissue [1]. Although it represents less than 0.1% of malignant tumors, it is considered the most common skin sarcoma [2,3]. In the United States, the annual incidence of DFSPs is about 4.5 cases per million individuals [3]. DFSP has no obvious sex predilection, but a slight male predominance was reported by some authors quoting a 3:2 male to female ratio [3,4]. It occurs typically in young and middle aged adults (20-50 years) [3-5]. African Americans are more affected than Caucasians, but familial predisposition or hereditary patterns have not been established [3]. DFSP typically occurs in the trunk and proximal extremities rather than the head and neck [1,3,4,6]. They account for 7% of head and neck sarcomas with less than 5% of all DFSPs occurring in the scalp region [3,4]. It can be classified as a low intermediate grade malignancy, which may invade the underlying tructures causing bony erosion, dural infiltration, and even brain nvasion, especially in the setting of recurrent tumors and certain brosarcomatous variants [3-6]. Distant spread is uncommon, but a few studies have reported metastases to bones, lungs, pancreas, or cervical lymph nodes [5-8].Difficulties in the management of scalp DFSP stem from the high propensity of its recurrence which is explained by tentacle like tentaclelike extensions of malignant cells that microscopically invade the surrounding dermis and subcutis horizontally and/or the underlying structures vertically, making it difficult to achieve clean surgical margins and to determine the tumor boundaries histopathologically [2,4]. Traditionally, wide local excision and/or Mohs micrographic surgery (MMS) have been used for the management of DFSP and are currently recommended by the National Comprehensive Cancer Network (NCCN) [2]. However, there are conflicting opinions regarding the safety and efficacy in terms of local recurrence, tissue preservation and subsequent reconstruction outcomes[2]. Numerous studies have demonstrated multi-staged surgical excision and reconstruction for the management of scalp DFSPs reporting unfavorable outcomes in terms of local recurrences and/or wound complications [4,6,7]. Despite this, surgical intervention remains the cornerstone of treatment for DFSPs, as both radiotherapy and chemotherapy are commonly only used for recurrent, unresectable, and metastasizing lesions [5,7,9].
In this technical note, we present the surgical management of a complex case of recurrent scalp DFSP, treated in a single stage multidisciplinary approach and with 5 years of follow up in order to report our advantageous experience and outcome with this scalp DFSP management. This study was approved by the institutional review board (IRB) of our hospital. An informed patient’s consent was obtained to publish this study.
Case Presentation
We report on a 25-year-old male Hispanic patient, who presented with a recurrent left sided fronto-parietal scalp lesion. His past medical history was significant for asthma and a positive family history of diabetes and hypertension. He was operated on 15 months prior to our intervention for a similar scalp lesion at another health care facility abroad.The patient was initially referred to the plastic surgery clinic by a dermatologist after the lesion had been biopsied and revealed a diagnosis of DFSP. On exam, the patient was found to have a large recurrent left sided fronto-parietal scalp lesion in the form of coalesced firm nodules, forming a fungating mass which arose from a raised painful scar of his previous surgical intervention. It was orange-yellow in color measuring about 4×3.5 cm with an adjacent solitary nodule medially measuring approximately 1.1 × 0.9 cm. CT revealed some bone erosions (Figure 1) and MRI did not show any evidence of brain invasion or parenchymal involvement. A wedge biopsy was performed by the plastic surgeon which confirmed the histopathological diagnosis of scalp DFSP with positive periosteal involvement. An elective, single-session, complex surgical procedure was therefore planned by a multidisciplinary team including neurosurgeons, head and neck, and plastic and reconstructive surgeons.
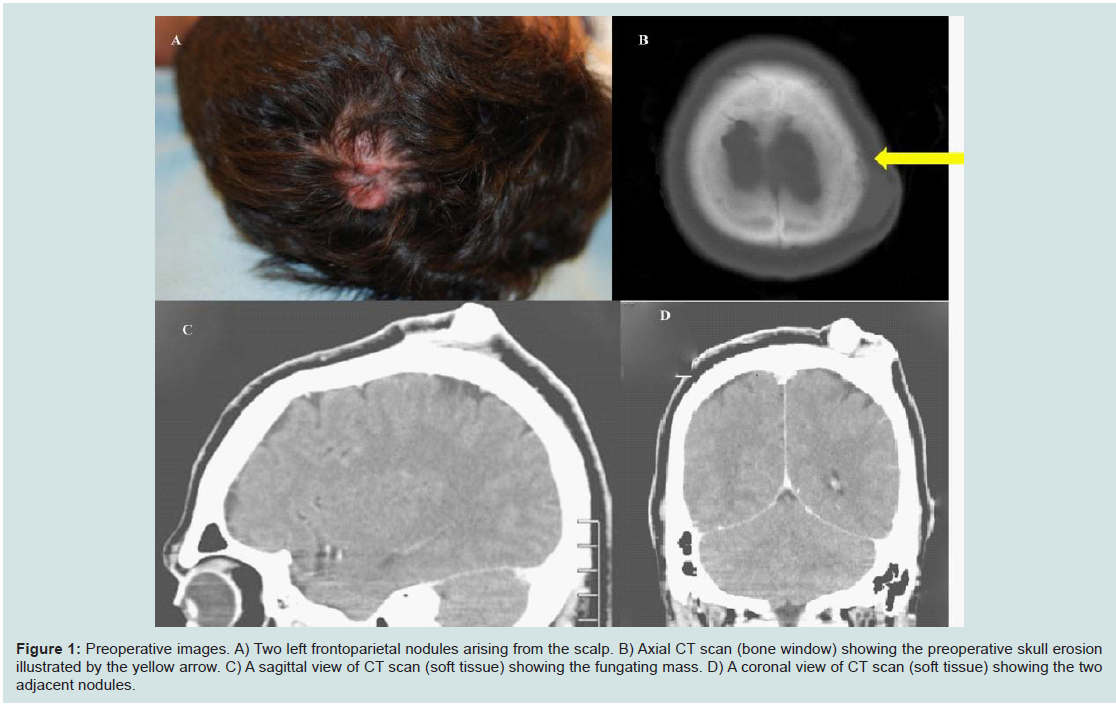
Figure 1: Preoperative images. A) Two left frontoparietal nodules arising from the scalp. B) Axial CT scan (bone window) showing the preoperative skull erosion illustrated by the yellow arrow. C) A sagittal view of CT scan (soft tissue) showing the fungating mass. D) A coronal view of CT scan (soft tissue) showing the two adjacent nodules.
The patient was placed in a lateral decubitus position. We carefully marked the anatomical landmarks including midline structures, superior sagittal sinus and infiltrative and safety margins of the tumor. Then we shaved, prepped and draped the patient in the usual sterile fashion. A wide-margin soft tissue component resection was first performed by the head and neck surgery team.
The neurosurgery team then placed multiple burr holes using a high-speed craniotome. Remnants of the inner table were removed using a straight cup curette. The dura was identified and a Penfield #3 was chosen to dissect the dura off the overlying bone. A side-cutting high-speed drill was chosen to perform a wide margin craniectomy including a rim of 2 cm of surrounding normal appearing bone. The specimen was removed en bloc and given to pathology for further analysis. Circumferential tenting stitches were applied using 4-0 Nurolon stitches. The dura was first excised and repaired with a dural allograft. We then carefully molded a titanium mesh according to the contour of the calvarium to close the cranial defect. It was secured with circumferential Synthes mini plate screws. Subsequent augmentation was performed by using methyl methacrylate forming a stable construct with the mesh during hardening which was copiously irrigated with bacitracin. This technique allowed a complete closure of the skull defect in a natural shape. We then covered the wound with bacitracin-soaked sponges until the plastics team was ready to proceed with a free flap closure of the skin defect that measured about 12 x 13 cm (Figure 2).

Figure 2: A) Intraoperative view of scalp and bone defect after titanium mesh implant and methacrylate allograft placement, prior to soft tissue coverage. B) Early postoperative view of graft recipient site.
In a final step, a split-thickness skin graft (at 0.015 inch) was harvested from the left lateral thigh. The skin graft was sewn in place with 4-0 chromic sutures. The skin graft was also tacked into place, and the preauricular incision for access to the STA and STV was closed with multiple 3-0 Vicryl sutures as well as a running 5-0 nylon suture. Penrose drains had been placed as well as a #15 Jackson Pratt. The donor site was closed with interrupted 3-0 Vicryl and 4-0 monocryl sutures.
Postoperative
Postoperatively, the patient was admitted to the ICU and remained initially intubated, sedated, and mechanically ventilated due to the length of the procedure (14 hours). The surgical site was monitored hourly by Doppler sonography at the venous and arterial anastomoses as well as with a continuous venous Doppler that was sutured around the vein. Parenteral IV antibiotics (Vancomycin/Ceftazidime) were administered for 8 days together with analgesics and Aspirin. Xeroform dressings were applied to the flap and skin graft donor sites. The patient was then discharged eight days following surgery after removal of the drains. Regular follow ups were done over a period of 5 years by both the neurosurgeons and the plastic surgeons with no evidence of erythema, subcutaneous collection, neurological deficit, meningeal signs, winging of the scapula, local recurrence, or distant spread (Figure 3).
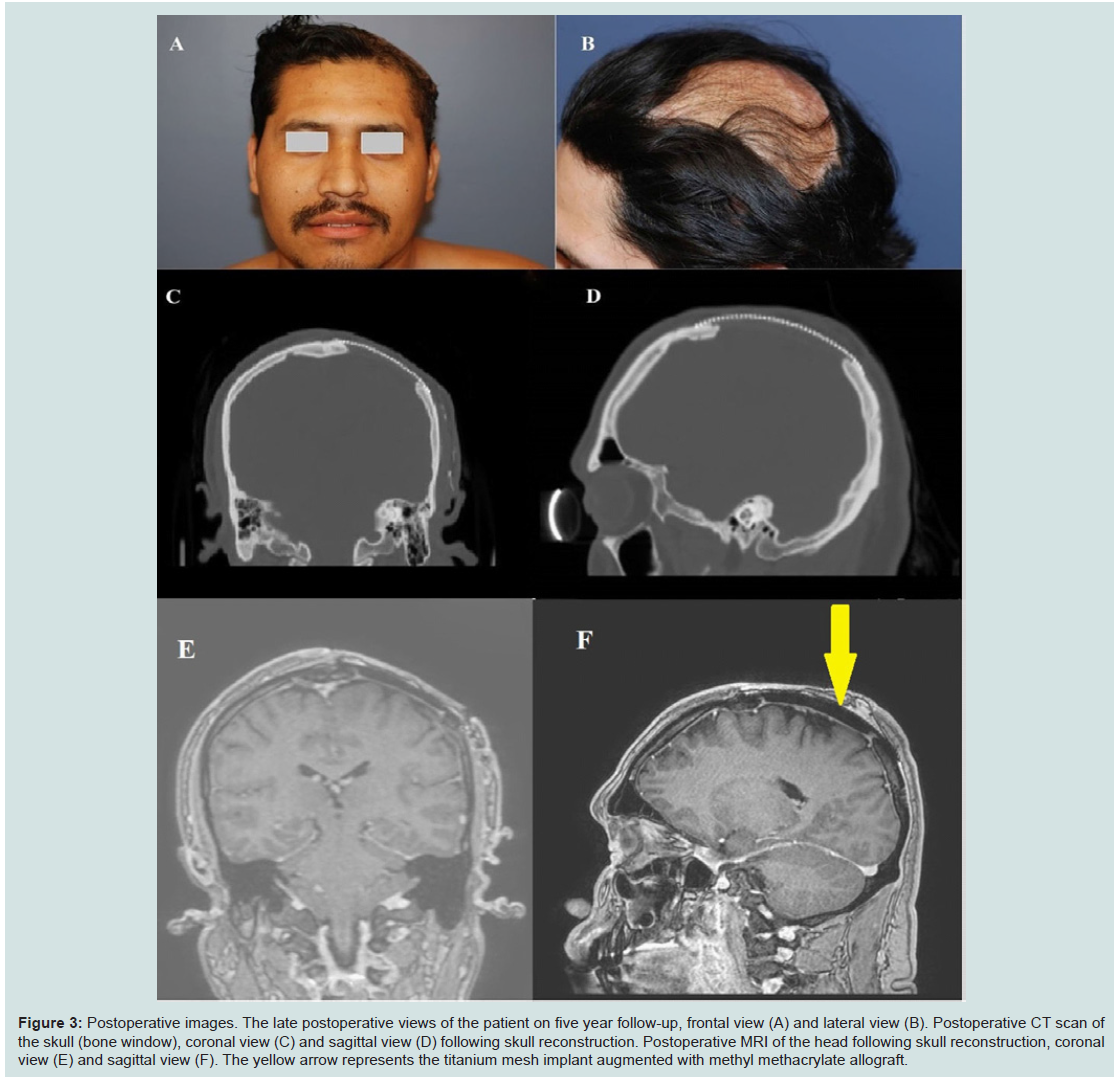
Figure 3: A) Postoperative images. The late postoperative views of the patient on five year follow-up, frontal view (A) and lateral view (B). Postoperative CT scan of the skull (bone window), coronal view (C) and sagittal view (D) following skull reconstruction. Postoperative MRI of the head following skull reconstruction, coronal view (E) and sagittal view (F). The yellow arrow represents the titanium mesh implant augmented with methyl methacrylate allograft.
Discussion
The clinical presentations of scalp DFSP are variable and can be deceiving for both patients and doctors [7]. It usually presents in the form of a solitary, painless, firm and slowly growing subcutaneous nodule or plaque with an irregular surface and hard indurated base [7,10]. Microscopic pathological examination is extremely important for proper diagnosis, as clinical findings alone are unreliable and may mimic other benign or malignant lesions [7].DFSP is characterized by the presence of monomorphic fibroblast like fibroblastlike spindle shaped cells embedded in collagen [7]. They are arranged in irregular interwoven fascicles forming a storiform pattern which gives a cartwheel appearance [3,7]. The presence of hemorrhagic foci may indicate higher metastatic potential [4].
Positive staining with CD34 is the most important immunohistochemical marker for DFSP diagnosis [5]. It is usedto differentiate DFSP from benign fibrous histiocytoma [5]. Furthermore, negative S-100 protein in DFSP excludes neurofibromas which react positively to it in 100% of cases [5,11]. S100 protein is also a reliable marker to excluded esmoplastic melanoma and spindle cell melanoma which react positively to it in 96.4% and 91.3% of cases, respectively [12,13]. Our histopathological specimen is represented in (Figure 4).
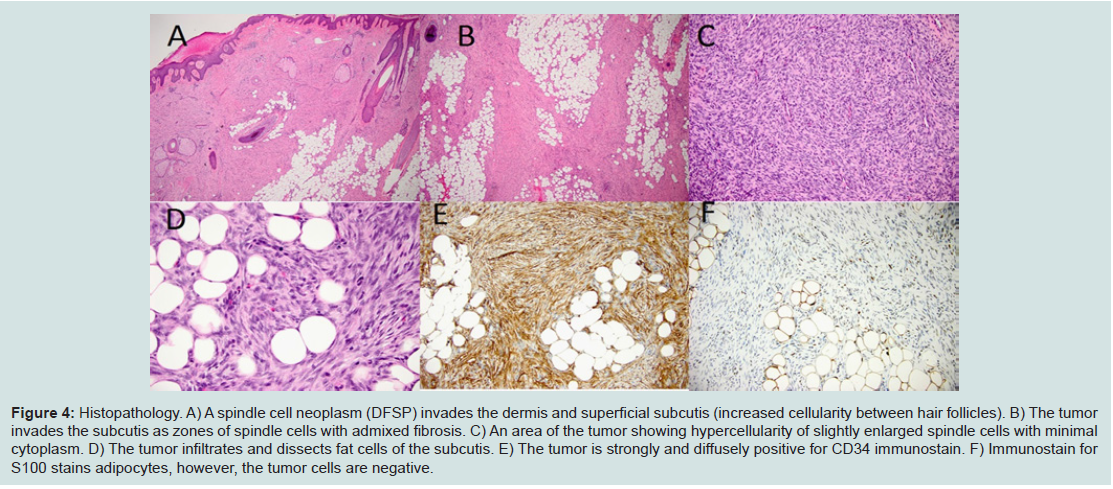
Figure 4: Histopathology. A) A spindle cell neoplasm (DFSP) invades the dermis and superficial subcutis (increased cellularity between hair follicles). B) The tumor invades the subcutis as zones of spindle cells with admixed fibrosis. C) An area of the tumor showing hypercellularity of slightly enlarged spindle cells with minimal cytoplasm. D) The tumor infiltrates and dissects fat cells of the subcutis. E) The tumor is strongly and diffusely positive for CD34 immunostain. F) Immunostain for S100 stains adipocytes, however, the tumor cells are negative.
Surgery remains the mainstay of management for DFSP. Wide local excision (WLE) and Mohs micrographic surgery (MMS) are the most commonly used procedures. MMS is preferred by many centers for DFSP treatment due to maximal conservation of surrounding normal tissue, and the fact that it allows frozensection histopathological examination - especially for the peripheral margins - during the procedure. It is recommended for large, recurrent, incompletely excised skin cancers or for tumors located in high-recurrence rate regions [7. However, MMS was criticized by many authors as being inaccurate, as it is difficult to distinguishDFSP malignant cells among scattered spindle cells of normal connective tissue debris [2]. Buck et al. approached 19 DFSP cases (3 of them located in head and neck) with a multidisciplinary team consisting of a Mohs micrographic surgeon, a surgical oncologist, a dermatopathologist, and a plastic surgeon. They used a multi-stage technique. In the first stage, mapping of peripheral margins wasdone using MMS. In the second stage, wide local excision (WLE) was performed together with dermatopathological examination. The stages were done several days apart. Then final surgical reconstruction was done immediately following the second stage. No recurrence was reported over a 17-month average follow up period. Seven postoperative complications were reported including partial suture dehiscence, seroma, cellulitis, skin graft loss, and one case of positive deep margin [2]. Rather than opting for staged management, our patient underwent a single-stage excision and reconstruction. This approach was found to be effective, safe and less time consuming providing the advantage of decreased hospital stay with no reported complications or evidence of local recurrence over a 5-year follow up period. The only noticed side effect was an area of alopecia at the site of surgery.
The reported 5 year survival rate for patients with DFSP is 99.2%. However, most patients with distant metastases die within 2 years of diagnosis. Fortunately, the incidence of metastases is low and varies from 1% to 4% [2]. A better prognosis is conferred by early and radical surgery [5]. An abundance of prognosticators are recorded in the literature including: fibrosarcomatous variant, positive microscopic margins, increased cellularity, high mitotic rate, patients aged above 50 years, multiple prior recurrences and extension of resection which is the most important factor [7,10,14]. Thieli and colleagues reported a case series of 7 patients with recurrent craniofacial DFSP who were treated by radical surgery with 1 cm safety margin in all directions. In the two cases where lesions were located in the scalp, recurrences were reported during follow up [1]. Some authors prefer wider safety margins measuring up to 2 to 3 cm [11]. Although it may prove difficult to obtain negative lateral margins by WLE techniques, negative deep margins are easily ascertained [2]. Roses and colleagues found that a margin of 3 cm or more results in a 20% recurrence rate compared to a 41% recurrence rate in patients with a safety margin of 2 cm or less [15]. This is contrary to our finding in which a 2 cm safety margin was excised including both skull bone and soft tissues and resulted in no evidence of relapse over a 5-year follow up period.
In our study, the serratus anterior myofascial free flap alone was successfully used for scalp reconstruction. Fibrinolytic agents were not used following the procedure. Split thickness skin graft was used from the thigh without any tissue expansion. Similarly, another study reported the use of the serratus anterior muscle flap but in combination with a latissimus dorsi flap in a case of massive malignant endothelioma involving the scalp with positive outcomes [16]. Trignano and colleagues also reported the usefulness of a combined latissimus dorsi/serratus anterior flap with superadded rib free flap as an alternative procedure of vascularized coverage of composite tissue defects following variable lesions involving scalp or extrimities [17]. Taniguchi and colleagues used a latissimus dorsi myocutaneous flap alone as skin coverage for a scalp defect following repeated surgical excisions of recurrent DFSP but with subsequent administration of Urokinase (which was not used in our case) [6]. Other reconstructive options include the use of rotational flaps and Acellular Dermal Matrix (ADM) in scalp DFSP cases [2].
There is a debate regarding the efficacy of radiotherapy in the management of DFSP. Some authors consider it beneficial as adjuvant therapy before or after surgery in terms of lowering recurrence rates [7,18,19]. DFSP lesions with positive margins following resection are considered to be radioresponsive at doses of 50-60 Gy [7,20]. Taniguchi and colleagues reported no effect on the blood supply of the myocutaneous flap used for scalp reconstruction at doses of 120 gray of gamma radiation [6]. In our case the patient did not receive pre or post-operative radiation and there was no evidence of local recurrence over a 5-year follow up period. This management of local disease without adjuvant radiation is corroborated by Vothand colleagues who found in an evidence-based review of literature that the theoretical effect of radiotherapy in preventing recurrence and metastasis is not supported by adequate data [21]. However, radiotherapy should be considered as an option in the management of unresectable DFSP lesions [3,22].
Historically, chemotherapy has proven to be unsuccessful in the management of patients with recurrent and/or metastatic DFSP [2]. Recently, understanding the molecular backgrounds of DFSP development has generated an interest in medical management using imatinib mesylate. Imatinib is a protein tyrosine kinase inhibitor that targets platelet-derived growth factor beta receptors which are upregulated secondary to a chromosomal translocation t(17:22) [2,23]. This chromosomal aberration exists in about 90% of DFSPs. NCCN recommends imatinib for adult patients with metastatic disease, recurrence in critical and functional cosmetic areas and cases with positive surgical margins after re-resection [23]. It may downstage the disease and facilitates residual tumor excision [2,23]. Imatinib can be the treatment of choice in patients with locally advanced irresectable lesions [7,24]. In our study, the patient did not receive any postoperative chemotherapeutic agent or molecular based medication with no evidence of distant spread on follow-up. This is supported by McArthur and colleagues who found that fibrosarcomatous variants of DFSP lacking t(17:22) may show no response to imatinib [24]. Furthermore, Uematsu and colleagues used methotrexate (50 mg/m2 body surface area) in a case with recurrent DFSP lesion based on a chemosensitivity test, but the lesion identified did not respond [5]. More specific targeted therapies are to be expected in the future. To the best of author’s knowledge, this is the first reported case of recurrent scalp DFSP treated successfully by conventional wide local excision and reconstruction without micrographic mapping technique or any adjuvant radiotherapy, chemotherapy or immunomodulation.
Conclusion
The rate of scalp DFSP recurrence varies with surgical technique and extent of resection [2,7]. Poor local control is documented when resection with conservative margins is applied [7,10]. DFSP should not be managed initially by simple surgical excision only in order to avoid recurrences which carry a high risk of deep invasions and distant spread which worsens the outcome and prognosis [6]. A single-stage complex surgical excision and reconstruction may represent a safe and an effective option in the management of recurrent DFSP scalp lesions with improved outcomes including minimal morbidity and prolonged recurrence free survival or cure.References
- Thiele OC, Seeberger R, Bacon C, Muhling J, Freier K, et al. (2009) Recurrent craniofacial dermatofibrosarcoma protuberans: long-term prognosis after close surgical removal. J Craniofac Surg 20: 844-846.
- Buck DW 2nd, Kim JY, Alam M, Rawlani V, Johnson S, et al. (2012) Multidisciplinary approach to the management of dermatofibrosarcoma protuberans. J Am Acad Dermatol 67: 861-866.
- Eguzo K, Camazine B, Milner D (2012) Giant dermatofibrosarcoma protuberans of the face and scalp: a case report. Int J Dermatol [Epub ahead of print].
- Loss L, Zeitouni NC (2005) Management of scalp dermatofibrosarcoma protuberans. Dermatol Surg 31: 1428-1433.
- Uematsu Y, Fukai J, Tamura M, Owai Y, Obayashi S, et al. (2003) Distant metastasis of dermatofibrosarcoma protuberans of the scalp--case report. Neurol Med Chir (Tokyo) 43: 493-496.
- Taniguchi Y, Tamaki T, Yoshida M, Uematsu Y (2002) Reconstruction of a scalp and skull defect with free latissimus dorsi myocutaneous flap following dermatofibrosarcoma protuberans. J Orthop Surg (Hong Kong) 10: 206-209.
- Kim SD, Park JY, Choi WS, Kim SH, Lim DJ, et al. (2007) Intracranial recurrence of the scalp dermatofibrosarcoma. Clin Neurol Neurosurg 109: 172-175.
- Lal P, Goel A, Mandal AK (2004) Dermatofibrosarcoma protuberans of scalp with cervical lymph node metastasis. Sarcoma 8: 43-45.
- Marks LB, Suit HD, Rosenberg AE, Wood WC (1989) Dermatofibrosarcoma protuberans treated with radiation therapy. Int J Radiat Oncol Biol Phys 17: 379-384.
- Stojadinovic A, Karpoff HM, Antonescu CR, Shah JP, Singh B, et al. (2000) Dermatofibrosarcoma protuberans of the head and neck. Ann Surg Oncol 7: 696-704.
- Hirabayashi S, Kajikawa A, Kanazawa K, Mimoto K (1989) Dermatofibrosarcoma protuberans with regional lymph node metastasis: a case report. Head Neck 11: 562-564.
- Ohsie SJ, Sarantopoulos GP, Cochran AJ, Binder SW (2008) Immunohistochemical characteristics of melanoma. J Cutan Pathol 35: 433-444.
- Weissinger SE, Keil P, Silvers DN, Klaus BM, Möller P et al. (2013) A diagnostic algorithm to distinguish desmoplastic from spindle cell melanoma. Mod Pathol 27: 524-534.
- Kimmel Z, Ratner D, Kim JY, Wayne JD, Rademaker AW, et al. (2007) Peripheral excision margins for dermatofibrosarcoma protuberans: a meta-analysis of spatial data. Ann Surg Oncol 14: 2113-2120.
- Roses DF, Valensi Q, LaTrenta G, Harris MN (1986) Surgical treatment of dermatofibrosarcoma protuberans. Surg Gynecol Obstet 162: 449-452.
- Tanaka Y, Miki K, Tajima S, Akamatsu J, Tsukazaki Y, et al. (1998) Reconstruction of an extensive scalp defect using the split latissimus dorsi flap in combination with the serratus anterior musculo-osseous flap. Br J Plast Surg 51: 250-254.
- Trignano E, Fallico N, Nitto A, Chen HC (2013) The treatment of composite defect of bone and soft tissues with a combined latissimus dorsi and serratus anterior and rib free flap. Microsurgery 33: 173-183.
- Sun LM, Wang CJ, Huang CC, Leung SW, Chen HC, et al. (2000) Dermatofibrosarcoma protuberans: treatment results of 35 cases. Radiother Oncol 57: 175-181.
- Abe T, Kamida T, Goda M, Inoue R, Fujiki M, et al. (2009) Intracranial infiltration by recurrent scalp dermatofibrosarcoma protuberans. J Clin Neurosci 16: 1358-1360.
- Ballo MT, Zagars GK, Pisters P, Pollack A (1998) The role of radiation therapy in the management of dermatofibrosarcoma protuberans. Int J Radiat Oncol Biol Phys 40: 823-827.
- Voth H, Landsberg J, Hinz T, Wenzel J, Bieber T, et al. (2011) Management of dermatofibrosarcoma protuberans with fibrosarcomatous transformation: an evidence-based review of the literature. J Eur Acad Dermatol Venereol 25: 1385-1391.
- Rutkowski P, Van Glabbeke M, Rankin CJ, Ruka W, Rubin BP, et al. (2010) Imatinib mesylate in advanced dermatofibrosarcoma protuberans: pooled analysis of two phase II clinical trials. J Clin Oncol 28: 1772-1779.
- McArthur GA (2007) Molecular targeting of dermatofibrosarcoma protuberans: a new approach to a surgical disease. J Natl Canc Netw 5: 557-562.
- McArthur GA, Demetri GD, van Oosterom A, Heinrich MC, Debiec-Rychter M, et al. (2005) Molecular and clinical analysis of locally advanced dermatofibrosarcoma protuberans treated with imatinib: Imatinib Target Exploration Consortium Study B2225. J Clin Oncol 23: 866-873.