
Case Report
*Address for Correspondence: Gollapalli V, Department of surgery, Bronx-Lebanon hospital, Bronx, NYC (Affiliated to Mt Sinai School of medicine), Attending Surgeon, 1650 Selwyn Ave Suite 4A, Bronx, New York, USA, Tel: 718 960 1216; Fax: 718 960 1370; E-mail: vgollapa@bronxleb.org
Citation: Gollapalli V, Bibi S, Shah AK, Gilchrist B. DCIS Breast Arising in a Fibroadenoma - Case Report of an Uncommon Condition. J Surgery. 2017;5(1): 4.
Copyright © 2017 Gollapalli V, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 5, Issue: 1
Submission: 28 November, 2016 | Accepted: 16 January, 2017 | Published: 24 January, 2017


DCIS Breast Arising in a Fibroadenoma - Case Report of an Uncommon Condition
Gollapalli V*, Bibi S, Shah AK and Gilchrist B
- Department of Surgery, Bronx Lebanon Hospital, Bronx, USA
*Address for Correspondence: Gollapalli V, Department of surgery, Bronx-Lebanon hospital, Bronx, NYC (Affiliated to Mt Sinai School of medicine), Attending Surgeon, 1650 Selwyn Ave Suite 4A, Bronx, New York, USA, Tel: 718 960 1216; Fax: 718 960 1370; E-mail: vgollapa@bronxleb.org
Citation: Gollapalli V, Bibi S, Shah AK, Gilchrist B. DCIS Breast Arising in a Fibroadenoma - Case Report of an Uncommon Condition. J Surgery. 2017;5(1): 4.
Copyright © 2017 Gollapalli V, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 5, Issue: 1
Submission: 28 November, 2016 | Accepted: 16 January, 2017 | Published: 24 January, 2017
Abstract
Introduction: Fibroadenoma (FA) is a type of benign tumor that occur in young women below the age of 35 years old. The incidence of carcinoma arising with FA is rare with range of 0.002-0.1% Most cases are detected at an early stage; cases of locally advanced carcinoma with distant metastasis have been published.Case presentation: We present a case of Ductal Carcinoma in situ (DCIS) with microinvasion arising within Fibroadenoma which was being followed for 9 years.
Discussion: Fibroadenoma is typically considered to be a type of benign lesion and requires careful observation. However, data regarding whether FA is a risk factor for carcinoma is inconsistent. The present case showed that FAs containing foci of carcinoma in situ can be indistinguishable from benign lesions with imaging, therefore, despite the incidence of carcinoma within FA is estimated at 0.002– 0.1%, it should be considered a long-term risk factor for invasive breast cancer. Complex FA has a higher risk. High degree of suspicion is needed, as there are limitations in screening, which adds to the problem of delayed diagnosis.
Conclusions: The present case was reported to increase awareness that Fibroadenoma in the middle and older age group can harbor cancer; early intervention in this age group is suggested.
Keywords
Case report; Breast cancer; FibroadenomaCase Report
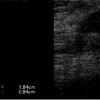
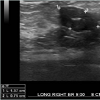
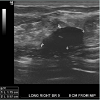
This is a 43 year female who was being followed for an image detected lesion (fibroadenoma) in the right breast upper outer quadrant, since age 34 (9 years ago). She had no family history of breast cancer. Initial imaging 9 years ago with Diagnostic mammogram and ultrasound showed a macrolobulated 1.8 cm hypoechoic lesion with a central of calcification in a very dense glandular breast tissue on right side consistent with fibroadenoma BI RADS 3 (Figure 1), interval follow up of 6 months was recommended. Serial imaging with Ultrasound & Mammogram at 6 months showed a hypoechoic 1.5 cm lesion at 9 ‘0’clock position with a calcification consistent with fibroadenoma (Figure 2-5). She was seen again in a year’s time with similar findings and was given BI RADS 2, annual follow up was recommended. She had a very glandular and dense breast, making the interpretation difficult and was BI RADS 2 or BI RADS 3 at times. The patient did not follow up consistently on a regular basis in between for 2 years and had imaging at outside center. She was seen again and Ultrasound/Diagnostic mammogram showed macro lobulated lesion with central calcification.. After 9 years of follow up, surveillance mammogram showed no change in the size of the mass, but increased number of faint polymorphic micro calcifications BIRADS 0 warranting biopsy (Figure 6-9). Ultrasound guided biopsy showed ductal carcinoma in situ, with areas of micro invasion. She underwent needle localized partial mastectomy and Sentinel lymph node biopsy. The size was 0.5 cm (pT1mic) and lymph node negative (pN0) (Figure 10). Tumor was estrogen and progesterone receptor positive and Her2 neu receptor negative. All margins were negative. She is currently undergoing radiation therapy followed by hormonal therapy. The patient was followed up every 3 months, and at the last follow-up examination in October 2016, the patient exhibited no signs of recurrence.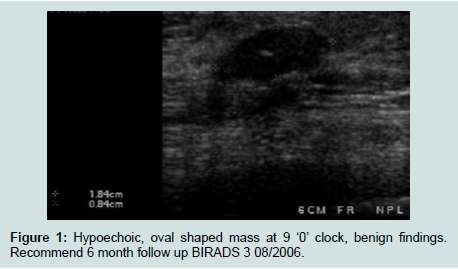
Figure 1: Hypoechoic, oval shaped mass at 9 ‘0’ clock, benign findings.Recommend 6 month follow up BIRADS 3 08/2006.
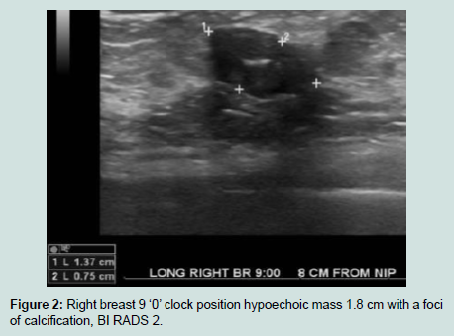
Figure 2: Right breast 9 ‘0’ clock position hypoechoic mass 1.8 cm with a foci of calcification, BI RADS 2.
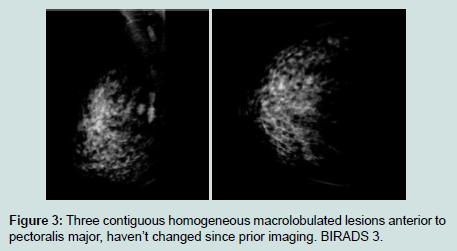
Figure 3: Three contiguous homogeneous macrolobulated lesions anterior topectoralis major, haven’t changed since prior imaging. BIRADS 3.
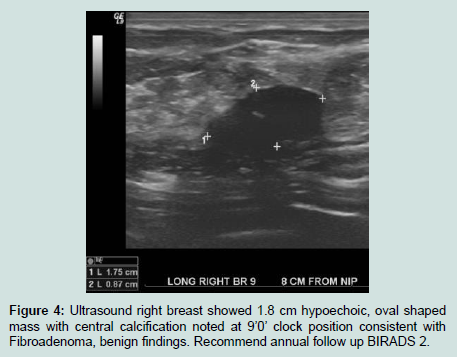
Figure 4: Ultrasound right breast showed 1.8 cm hypoechoic, oval shapedmass with central calcification noted at 9’0’ clock position consistent with Fibroadenoma, benign findings. Recommend annual follow up BIRADS 2.
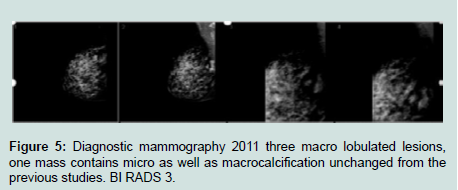
Figure 5: Diagnostic mammography 2011 three macro lobulated lesions,one mass contains micro as well as macrocalcification unchanged from the previous studies. BI RADS 3.
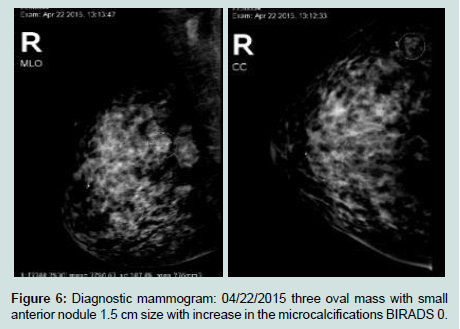
Figure 6: Diagnostic mammogram: 04/22/2015 three oval mass with smallanterior nodule 1.5 cm size with increase in the microcalcifications BIRADS 0.
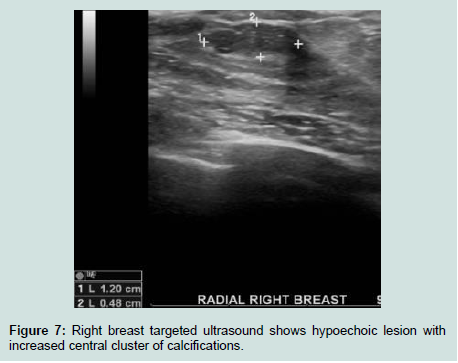
Figure 7: Right breast targeted ultrasound shows hypoechoic lesion withincreased central cluster of calcifications.
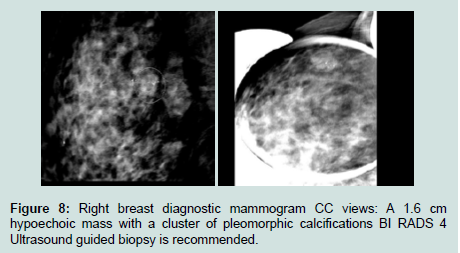
Figure 8: Right breast diagnostic mammogram CC views: A 1.6 cmhypoechoic mass with a cluster of pleomorphic calcifications BI RADS 4 Ultrasound guided biopsy is recommended.
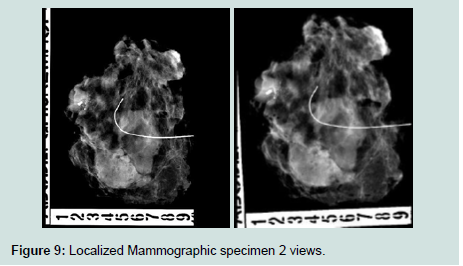
Figure 9: Localized Mammographic specimen 2 views.
Discussion
Fibroadenomas (FA) are a common type of benign tumor that occurs in younger women below the age of 35 years old, with a reported incidence rate of 7-13% in female individuals. It may occur at any age; however, the peak age of incidence is in the second and third decade of life. The FA can be stimulated by estrogen, progesterone, pregnancy and lactation, and may undergo atrophy during menopause [1,2]. Furthermore, FA is a biphasic tumor composed of stromal and epithelial components, and can be effectively treated by local excision [3]. Most cases are detected at an early stage, cases of locally advanced carcinoma with distant metastasis have been published [2-6].They occur asymptomatically in 25% of all patients. The majority FAs are clinically identifiable; however, 25% of cases are non-palpable and, thus, require mammography and/or Ultrasonography (US) for diagnosis [4,7,8]. The incidence of carcinoma arising with FA is rare with range of 0.002 to 0.125% [4-6]. Previous studies have reported that fibroadenomas can evolve into different types of malignancy, such as lobular intraepithelial neoplasia, lobular carcinoma in situ, malignant phyllodes tumors and microinvasive lobular carcinoma [7-11].
According to its clinicopathological presentation, FA can be divided into simple and complex FA. Complex FA is characterized by cysts, sclerosing adenosis, epithelial calcification or papillary apocrine change [1,12,13]. Carcinoma arising within a fibroadenoma is a rare with an incidence rate of 0.1-0.3% in a screened population [14] and unique subtype of mammary cancer, which was reported by Buzanowski-Konakry et al. in 1975 [9]. To date, 15-18].
Therefore, histological diagnosis is typically unexpected [1,10,11,19,20]. The mean age of patients with carcinoma in FA has been reported as 42-44 years, ~20 years subsequent to the peak age of occurrence of FA [15,21]. Our patient was in this 40’s age group. Two-thirds of carcinomas within FA are lobular, and one-third are ductal or mixed ductal and lobular, with the frequency of LCIS and ductal carcinoma in situ almost equal [2,15]. Carcinoma is diagnosed as arising within FA if: 1) The carcinoma is entirely encased within the FA; or 2) if the carcinoma is only focally involved with the adjacent breast tissue [3]. The case presented in the present study met the first criterion.
FA is typically considered to be a type of benign lesion and requires careful observation. However, data regarding whether FA is a risk factor for carcinoma is inconsistent [22]. A number of studies have provided evidence of the association between the excised FA and carcinoma. The relative risk of developing breast cancer following surgically excised FA appears to depend on the histological characteristics of FA and the state of the breast parenchyma [4,23].
The present case showed that FAs containing foci of carcinoma in situ can be indistinguishable from benign lesions following imaging, therefore, despite the incidence of carcinoma within FA is estimated at 0.002-0.125%, it should be considered a long-term risk factor for invasive breast cancer. The present describes a case of DCIS arising within an FA and conducts a review of the relevant literature.
FA is considered to be an aberration of normal breast development [24] and the majority that occur in younger females may resolve or reduce in size without intervention [8,25]. Although malignancy in FA is rare it may be difficult to predict malignant transformation in a FA, as the clinical and radiological signs may be masked [6]. There is a general consensus that the management of FA depends on the age of the patient, the nature of the lesion, the family history of breast or ovary carcinoma, or any data of proliferative changes in the breasts from previous biopsies [8,26]. For example, previous studies have proposed a conservative therapeutic strategy for FA in patients younger than a certain age. However, the threshold ages proposed or conservative treatment is inconsistent, and have been reported as 25, 35 and 45 years [27-30]).
If the lesion increases in size regardless of age, excision is immediately performed. However, if the lesion is regressive, follow up should be continued until the regression is complete. If the lesion does not completely regress, or stabilizes by the age of 35 years, a lumpectomy is suggested. For females aged >35 years, greater than 2.5 cm, surgery should be recommended if increases in size after a 6- to 12-month follow-up period or any stable FA with complex features on imaging. For patients with a family history of breast and/or ovarian cancer, surgery is more actively advised. Currently, the therapeutic methods used for breast cancer include surgery, chemotherapy, radiotherapy, endocrine therapy and targeted therapy [3]. The treatment for DCIS arising within fibroadenoma is not clearly defined. DCIS is treated by surgical excision, followed by radiotherapy as part of breast conserving treatment, and/or endocrine therapy.
The aggressiveness, morbidity and mortality is not clear. Presence of carcinoma could also be a sign of the deficiency related to the screening system. The use of mammograms in young females has widely been documented to be of limited value due to increased breast density [31]. As most of the patients with FA are young and have dense breast that might preclude detection of these lesions. Ultrasound is operator dependent close follow up may not be as accurate as possible. Hence suggest early MRI of breast as an option. High degree of suspicion is needed, as there are limitations in screening, which adds to the problem of delayed diagnosis.
Conclusion
The present case was reported to increase awareness that FA in the middle and older age group with complex characteristics on imaging can harbor cancer. We suggest early intervention in this age group.Acknowledgements
Author contributions: Dr. Gollapalli V had full access to all data in the study and takes responsibility for the integrity and accuracy of the data.Drafting of case report: Dr. Gollapalli V, Dr. Bibi S Critical revision of the manuscript for important intellectual content: Dr. Gollapalli V, MD, Dr. Bibi S, MD, Dr. Shah AK and Gilchrist B.
References
- Kuijper A, Mommers EC, van der Wall E, van Diest PJ (2001) Histopathology of the fibroadenoma of the breast. Am J Clin Pathol 115:736-742.
- Kuijper A, Preisler-Adams SS, Rahusen FD, Gille JJ, van der Wall E, et al. (2002) Multiple fibroadenomas harboring carcinoma in situ in a woman with a family history of breast/ovarian cancer. J Clin Pathol 55: 795-797.
- Azzopardi JG, Ahmed A, Mills RR (1979) Problems in breast pathology. Major Probl Pathol 11: 1-466.
- Dupont WD, Page DL, Parl FF, Vnencak-Jones CL, Plummer WD Jr, et al. (1994) Long-term risk of breast cancer in women with fibroadenoma. N Engl J Med 331: 10-15.
- El-Wakeel H, Umpleby HC (2003) Systematic review of fibroadenoma as a risk factor for breast cancer. Breast 12: 302-307.
- Wu YT, Chen ST, Chen CJ, Kuo YL, Tseng LM, et al. (2014) Breast cancer arising within fibroadenoma: collective analysis of case reports in the literature and hints on treatment policy. World J Surg Oncol 12: 335.
- Greenberg R, Skornick Y, Kaplan O (1998) Management of breast fibroadenomas. J Gen Intern Med 13: 640-645.
- Drukker BH (1997) Breast disease: a primer on diagnosis and management. Int J Fertil Womens Med 42: 278-287.
- Buzanowski-Konakry K, Harrison EG Jr, Payne WS (1975) Lobular carcinoma arising in fibroadenomas of the breast. Cancer 35: 450-456.
- De Iyengar KR, Peh SC, Yip CH, Vijayananthan A (2009) Infiltrating duct carcinoma within a fibroadenoma. Indian J Cancer 46: 244-246.
- Abe H, Hanasawa K, Naitoh H, Endo Y, Tani T, et al. (2004) Invasive ductal carcinoma within a fibroadenoma of the breast. Int J Clin Oncol 9: 334-338.
- Dixon JM, Mansel RE (1994) ABC of breast diseases. Congenital problems and aberrations of normal breast development and involution. BMJ 309: 797-800.
- Tissier F, De Roquancourt A, Astier B, Espie M, Clot P, et al. (2000) Carcinoma arising within mammary fibroadenomas. A study of six patients. Ann Pathol 20: 110-114.
- Lakhani SR, Ellis LO, Schnitt SJ, Tan PH, van de Vijver MJ (2012) WHO classification of tumours of the breast. In: Lakhani SR, Schnitt SJ, Malley FO, van de Vijver MJ, Simpson PT, et al. (Eds). Lobular neoplasia. IARC Press; Lyon, pp. 77-80.
- Diaz NM, Palmer JO, McDivitt RW (1991) Carcinoma arising within fibroadenomas of the breast. A clinicopathologic study of 105 patients. Am J Clin Pathol 95: 614-622.
- Fukuda M, Nagao K, Nishimura R, Matsuda M, Baba K, et al. (1989) Carcinoma arising in fibroadenoma of the breast--a case report and review of the literature. Jpn J Surg 19: 593-596.
- Yoshida Y, Takaoka M, Fukumoto M (1985) Carcinoma arising in fibroadenoma: case report and review of the world literature. J Surg Oncol 29: 132-140.
- Tanaka A, Hirano M, Sakai Y, Ichikawa T, Nitta N, et al. (1983) Fibroadenoma, mastopathy, intraductal papilloma: relationship to carcinoma--a case report of carcinoma of the breast arising in fibroadenoma. Nihon Geka Hokan 52: 232-243.
- Sklair-Levy M, Sella T, Alweiss T, Craciun I, Libson E, et al. (2008) Incidence and management of complex fibroadenomas. AJR Am J Roentgenol 190: 214-218.
- Netto D, Satchidanand SK, Gaeta JF (1980) Carcinomas arising in fibroadenomas: a report of two cases and a review of literature. J Surg Oncol 13: 367-372.
- Pick PW, Iossifides IA (1984) Occurrence of breast carcinoma within a fibroadenoma. A review. Arch Pathol Lab Med 108: 590-594.
- Dent DM, Cant PJ (1989) Fibroadenoma. World J Surg 13: 706-710.
- McDivitt RW, Stevens JA, Lee NC, Wingo PA, Rubin GL, et al. (1992) Histologic types of benign breast disease and the risk for breast cancer. The Cancer and Steroid Hormone Study Group. Cancer 69: 1408-1414.
- Hughes LE, Mansel RE, Webster DJ (1987) Aberrations of normal development and involution (ANDI): a new perspective on pathogenesis and nomenclature of benign breast disorders. Lancet 2: 1316-1319.
- Carty NJ, Carter C, Rubin C, Ravichandran D, Royle GT, et al. (1995) Management of fibroadenoma of the breast. Ann R Coll Surg Engl 77: 127-130.
- Goldman RL, Friedman NB (1969) Carcinoma of the breast arising in fibroadenomas, with emphasis on lobular carcinoma. A clinicopathologic study. Cancer 23: 544-550.
- Cant PJ, Madden MV, Close PM, Learmonth GM, Hacking EA, et al. (1987) Case for conservative management of selected fibroadenomas of the breast. Br J Surg 74: 857-859.
- Sainsbury JR, Nicholson S, Needham GK, Wadehra V, Farndon JR (1988) Natural history of the benign breast lump. Br J Surg 75: 1080-1082.
- Wilkinson S, Anderson TJ, Rifkind E, Chetty U, Forrest AP (1989) Fibroadenoma of the breast: a follow-up of conservative management. Br J Surg 76: 390-391.
- Dixon JM, Dobie V, Lamb J, Walsh JS, Chetty U (1996) Assessment of the acceptability of conservative management of fibroadenoma of the breast. Br J Surg 83: 264-265.
- Templeman C, Hertweck SP (2000) Breast disorders in the pediatric and adolescent patient. Obstet Gynecol Clin North Am 27: 19-34.