
Case Report
A Thorough Genital Examination is the Key
Marianne Abdo Alam1*, Smart Najib Zeidan1, David Raja Breiche2 and Nabil Adel Diab1
- 1Department of Pediatric Surgery, University of Balamand, Lebanon
- 2Department of Pediatrics, Bekaa Hospital, Lebanon
*Address for Correspondence: Marianne Alam, University of Balamand, Faculty of Medicine & Medical sciences, Beirut, 00961 70 234 782, Lebanon; E-mail: marianne.alam@gmail.com
Citation: Alam MA, Zeidan SN, Breiche DR, Diab NA. A Thorough Genital Examination is the Key. J Pediatr Child Care. 2018;4(1): 01.
Copyright: © 2018 Alam MA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 4, Issue: 1
Submission: 03 May, 2018 | Accepted: 18 May, 2018 | Published: 28 May, 2018
Keywords
Incontinence; Female hypospadias; Imperforate hymen; Genital examination
Abstract
We report a case of lifelong urine incontinence in a 9-year-old girl who underwent numerous diagnostic modalities and treatment without success. A thorough genital examination revealed a mild female hypospadias with imperforate hymen and unlocked the mystery behind her refractory state for treatment. This association led to urine accumulation within the vagina with subsequent continuous dribbling. Her condition was treated by hymenectomy.
Introduction
Urinary incontinence is commonly managed by healthy dietary habits, constipation treatment and micturition calendars. Refractory incontinence should raise the possibility of anatomic abnormalities and warrants referral to a pediatric urologist [1]. Diagnosis can be made by a simple physical exam and obviate the need for unnecessary radiological investigations.
Case Report
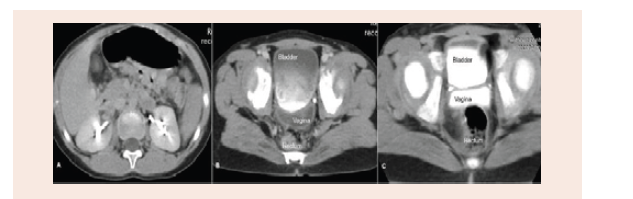
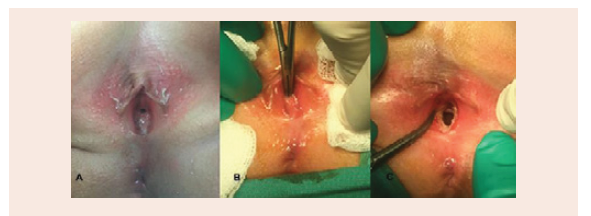
A 9-year-old girl was referred for daytime wetting and nocturnal enuresis. She voids 6 times per day with good quantities but continuous dribbling was noted. There was no urgency, frequency or previous surgeries. Four years ago, urodynamic studies in another institution showed no detrusor overactivity at the filling phase, a capacity of 160 ml, low detrusor pressure and no post-void residue. CT urogram revealed normal kidneys and ureters with Urine filling the vagina (Figure 1). Her pediatric urologist taught her the correct voiding posture with opening thighs without improvement. Current examination of the external genitalia revealed a normal appearing vulva, one orifice leaking urine and an imperforate hymen (Figure 2A). Under general anesthesia, hymenectomy was performed and a hypospadic urethra was noted (Figure 2B-2C). Cystovaginoscopy was within normal limits. Postoperatively, patient became continent. One year later, she is still doing well.
Discussion
Urinary incontinence is a common condition in pediatrics. Establishing healthy dietary habits, treating constipation and maintaining regular voiding pattern constitute the mainstay of therapy [1]. Anatomic abnormalities are the main contributors to refractory incontinence and the need for referral to a specialist. To our knowledge, this is the first reported case of urinary incontinence in girls secondary to the association of female hypospadias with imperforate hymen. This association led to urine accumulation within the vagina with subsequent continuous dribbling [2]. History and urogenital examination are enough to establish the diagnosis for timely treatment and minimizing unnecessary radiological investigations. However, when physical exam is non-revealing, further diagnostic modalities should be done to exclude an ectopic ureter associated with a double collecting system or a congenital vesicovaginal fistula in girls with dribbling [3-5].
References
- Haid B, Tekgul S (2017) Primary and secondary enuresis: pathophysiology, diagnosis, and treatment. Eur Urol Focus 3: 198-206.
- Su CC, Chang SJ, Yang SS (2014) Postvoiding urine accumulation in the vestibule in a girl complaining of postvoiding urine incontinence. Low Urin Tract Symptoms 6: 185-186.
- Carrico C, Lebowitz RL (1998) Incontinence due to an infrasphincteric ectopic ureter: why the delay in diagnosis and what the radiologist can do about it. Pediatr Radiol 28: 942-949.
- Jain KA (2007) Ectopic vaginal insertion of an obstructed duplicated ureter in an adult female: demonstration by magnetic resonance imaging. Clin Imaging 31: 54-56
- Martínez Escoriza JC, Palacios Marques AM, Lopez Fernandez JA, Feliu Rey E, Martín Medina P, et al. (2014) Congenital vesicovaginal fistula with or without menouria: a literature review. Eur J Obstet Gynecol Reprod Biol 175: 38-48.