
Case Report
*Address for Correspondence: Aye Aye Myint, Department of Pediatrics, Mandalay Children Hospital, University of Medicine, Mandalay, 30th Street, 73-74 Block, Mandalay, Myanmar, Tel: (095) 01681517; E-mail: aye441@gmail.com
Citation: Myo K, Maw SY, Myint AA. A Boy with Disseminated Tuberculosis. J Pediatr Child Care. 2016;2(1): 03.
Copyright © 2016 Myint, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 2, Issue: 1
Submission: 06 February, 2016 | Accepted: 09 March, 2016 | Published: 14 March, 2016
Reviewed & Approved by: Dr. Bryan Burnette, Clinical Pediatrics, Vanderbilt University School of Medicine, USA
 The child’s condition did not improve over the following days, and he required non-invasive respiratory support by nasal continuous positive airway pressure. Three days later, he had a brief generalised seizure which was controlled by a single dose of rectal diazepam. Blood pressure was found to be 130/90 mmHg, pulse rate was 60/minute, and random blood sugar level was 5.5 mmol/L. After the seizure, he remained semiconscious (GCS: 9/15) and was no longer able to move his right upper and lower limbs, together with ptosis, convergent strabismus, pupillary dilatation, and papilloedema in the right eye.
The child’s condition did not improve over the following days, and he required non-invasive respiratory support by nasal continuous positive airway pressure. Three days later, he had a brief generalised seizure which was controlled by a single dose of rectal diazepam. Blood pressure was found to be 130/90 mmHg, pulse rate was 60/minute, and random blood sugar level was 5.5 mmol/L. After the seizure, he remained semiconscious (GCS: 9/15) and was no longer able to move his right upper and lower limbs, together with ptosis, convergent strabismus, pupillary dilatation, and papilloedema in the right eye.


 The child was treated with a combination of isoniazid, rifampicin, pyrazinamide, ethambutol, and streptomycin together with prednisolone according to the national guideline. He made a gradual recovery with satisfactory weight gain over the next two months. Unfortunately, right hemiparesis, ptosis and convergent strabismus persisted. He will need multidisciplinary care for possible long term complications of post-meningoencephalitic cerebral palsy. Currently, he is in the continuation phase of anti-tuberculosis treatment with isoniazid and rifampicin and receiving rehabilitation therapy from physical medicine department.
The child was treated with a combination of isoniazid, rifampicin, pyrazinamide, ethambutol, and streptomycin together with prednisolone according to the national guideline. He made a gradual recovery with satisfactory weight gain over the next two months. Unfortunately, right hemiparesis, ptosis and convergent strabismus persisted. He will need multidisciplinary care for possible long term complications of post-meningoencephalitic cerebral palsy. Currently, he is in the continuation phase of anti-tuberculosis treatment with isoniazid and rifampicin and receiving rehabilitation therapy from physical medicine department.
A Boy with Disseminated Tuberculosis
Kyaw Myo, San Yu Maw and Aye Aye Myint*
- Department of Pediatrics, Mandalay Children Hospital, Myanmar
*Address for Correspondence: Aye Aye Myint, Department of Pediatrics, Mandalay Children Hospital, University of Medicine, Mandalay, 30th Street, 73-74 Block, Mandalay, Myanmar, Tel: (095) 01681517; E-mail: aye441@gmail.com
Citation: Myo K, Maw SY, Myint AA. A Boy with Disseminated Tuberculosis. J Pediatr Child Care. 2016;2(1): 03.
Copyright © 2016 Myint, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 2, Issue: 1
Submission: 06 February, 2016 | Accepted: 09 March, 2016 | Published: 14 March, 2016
Reviewed & Approved by: Dr. Bryan Burnette, Clinical Pediatrics, Vanderbilt University School of Medicine, USA
Abstract
Tuberculosis is a common infectious disease in developing countries. In the paediatric population, the disease can be manifested as pulmonary as well as extrapulmonary tuberculosis affecting multiple organs and systems at the same time. Delay in diagnosis and treatment can result in rapid progression of the disease with debilitating consequences in infants and young children because of weak immune defence mechanisms. We have described a case of disseminated tuberculosis involving the lungs, abdomen, lymphoreticular and central nervous systems.Keywords
Disseminated; Tuberculosis; ChildrenIntroduction
Tuberculosis (TB) is an important global health problem, with the highest burden falling on the middle and low income countries of Asia and Africa. According to “Global Tuberculosis Report 2014” by World Health Organization (WHO), TB incidence among children was estimated at 550000, equivalent to about 6% of the total number of 9 million new cases in 2013 [1].In the paediatric population, tuberculosis can present with various manifestations; pulmonary as well as extrapulmonary affecting multiple organs and systems at the same time. Diagnosis of childhood tuberculosis can be delayed or missed because in many developing countries, it mainly relies upon clinical, radiological and tuberculin skin test findings which are all non-specific [2-4] and subject to interobservervariability [5]. Microbiological confirmation is also not always available because of the difficulty in obtaining a good sputum specimen for examination and the paucibacillary nature of childhood tuberculosis.
Consequently, recent tuberculosis research has focused on development of molecular diagnostic technologies such as XPERT MTB/RIF assay and alternative specimens such as gastric lavage or aspirate for diagnosis of childhood tuberculosis [6,7].
Case Report
A 10 month old boy was admitted for fever with cough and dyspnoea for three days. The boy had a similar illness three months ago, and was diagnosed and treated as pneumonia. There was mild persistent cough between the two episodes. He was the only son of a healthy couple and his immunisations were all up to date for his age.Moderate respiratory distress was present. Proptosis was seen in both eyes. Weight, height and head circumference were between 3rd and 50th centile. Blood pressure was 120/80 mmHg, at 95th centile for his age. Vesicular breath sounds were heard in both lungs with diffuse crepitations. Abdomen was distended with massive hepatosplenomegaly. No significant abnormality was detected on neurological examination.
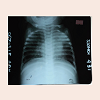
Basic investigations showed hypochromic anaemia, neutrophilic leucocytosis, increased CRP, and hyponatraemia. Lobar consolidation was seen in the left lung and nodular opacities were detected in the right lung (Figure 1). The child was treated with intravenous antibiotics according to WHO guideline for pneumonia, intravenous fluids and oxygen via a nasal cannula.
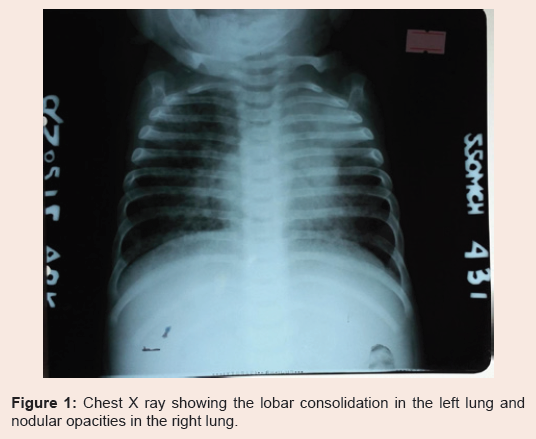
Figure 1: Chest X ray showing the lobar consolidation in the left lung and nodular opacities in the right lung.
Gastric lavage aspirate was examined for Mycobacterium tuberculosis. Smear microscopy was negative for acid fast bacilli. Xpert MTB/RIF assay detected Mycobacterium tuberculosis, but no rifampicin resistance. Solid culture on Lowenstein Jansen media also had abundant growth six weeks later, and Mycobacterium tuberculosis was confirmed by SD TB Ag MPT 64 Rapid test.
Contrast enhanced CT scan of the brain revealed multifocal hypodense areas in both basal ganglia and dilatation of lateral and third ventricles (Figures 2A and 2B). CT scan of the abdomen also revealed matted bowels, mesenteric lymphadenopathy, ascites and small renal stones in the right kidney (Figure 3). Both were typical radiological findings of tuberculosis infection. Cerebrospinal fluid and bone marrow examinations were not performed because lumbar puncture was deemed unsafe in a child with features of increased intracranial pressure and the results were also unlikely to have changed the management decisions.
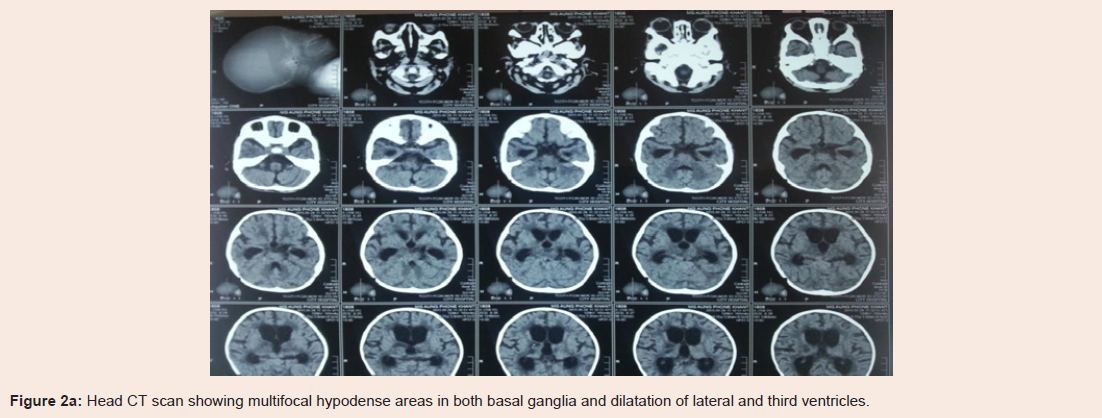
Figure 2a: Head CT scan showing multifocal hypodense areas in both basal ganglia and dilatation of lateral and third ventricles.
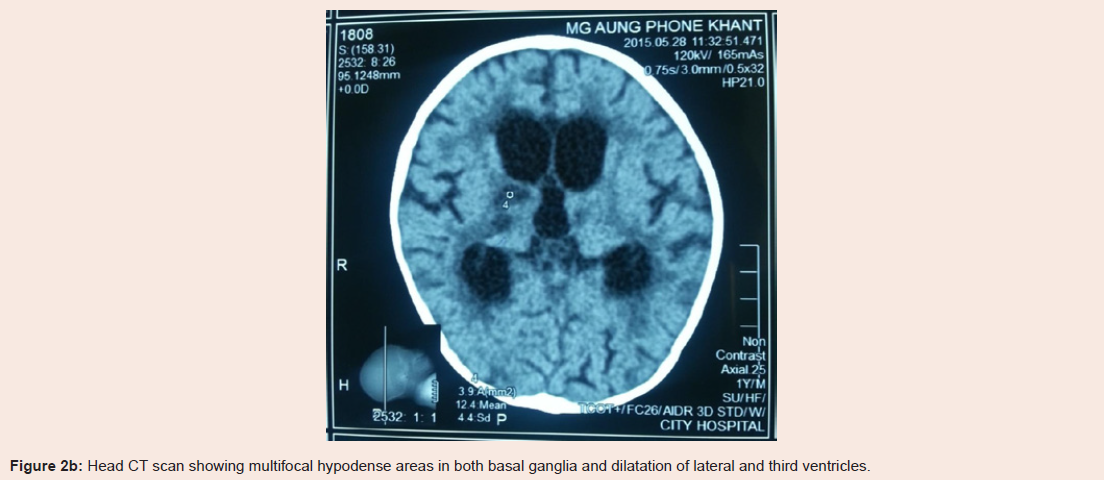
Figure 2b: Head CT scan showing multifocal hypodense areas in both basal ganglia and dilatation of lateral and third ventricles.
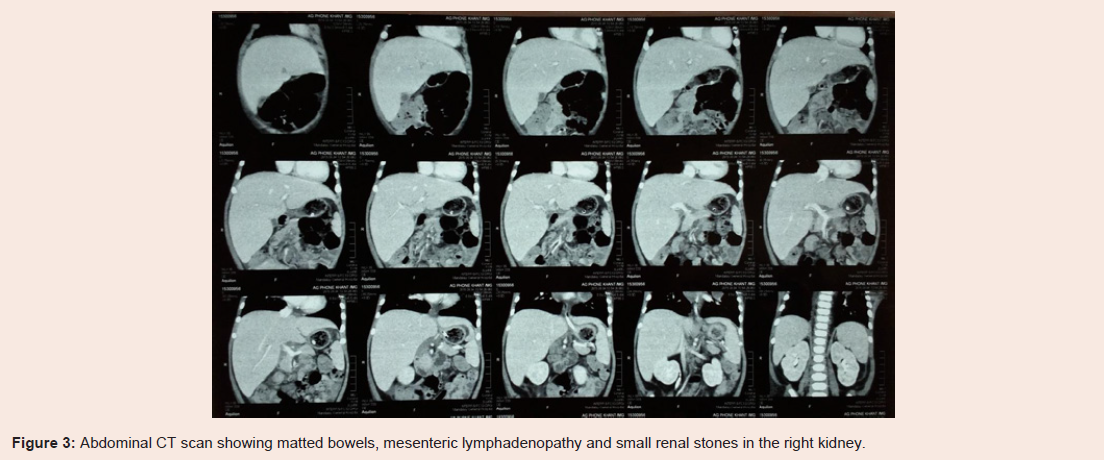
Figure 3: Abdominal CT scan showing matted bowels, mesenteric lymphadenopathy and small renal stones in the right kidney.
Discussion
The incidence of disseminated tuberculosis ranges from 1-3% of all tuberculosis cases [8,9]. It can involve pulmonary as well as extrapulmonary sites mainly affecting the organs and systems such as lungs, abdomen, and central nervous system. New molecular diagnostic tests and non-sputum specimens have been recommended for accurate and rapid diagnosis of childhood tuberculosis because delay in the diagnosis and treatment can result in rapid progression of the disease with debilitating consequences in infants and young children [6,7].The patient that we have reported was affected by Mycobacterium tuberculosis infection involving the lungs, kidneys, intestines, mesenteric lymph nodes and central nervous system. The case history also indicates the usefulness of gastric aspirate in children for microbiological confirmation of pulmonary tuberculosis and the superiority of XPERT MTB/RIF assay to conventional smear microscopy in terms of accuracy and to solid culture in terms of time required for diagnostic results (hours vs weeks). Unfortunately, the child survived with serious disabilities, including hemiparesis, ptosis, strabismus and possible long term consequences of cerebral palsy.
Conclusion
Disseminated tuberculosis can present with various manifestations affecting multiple organs and systems at the same time. Molecular diagnostic tests and gastric lavage aspirate are useful for fast and accurate diagnosis of the condition in children. Delay in diagnosis and treatment can result in rapid progression of the disease with debilitating consequences in infants and young children because of weak immune defence mechanisms.References
- WHO (2014) Global tuberculosis report 2014. World Health Organization. Geneva, Switzerland, pp. 1-171.
- Zar HJ, Connell TG, Nicol M (2010) Diagnosis of pulmonary tuberculosis in children: new advances. Expert Rev Anti Infect Ther 8: 277-288.
- Hatherill M, Hanslo M, Hawkridge T, Little F, Workman L, et al. (2010) Structured approaches for the screening and diagnosis of childhood tuberculosis in a high prevalence region of South Africa. Bull World Health Organ 88: 312-320.
- Hesseling AC, Schaaf HS, Gie RP, Starke JR, Beyers N (2002) A critical review of diagnostic approaches used in the diagnosis of childhood tuberculosis. Int J Tuberc Lung Dis 6: 1038-1045.
- Du-Toit G, Swingler G, Iloni K (2002) Observer variation in detecting lymphadenopathy on chest radiography. Int J Tuberc Lung Dis 6: 814-817.
- Bates M, O'Grady J, Maeurer M, Tembo J, Chilukutu L, et al. (2013) Assessment of the Xpert MTB/RIF assay for diagnosis of tuberculosis with gastric lavage aspirates in children in sub-Saharan Africa: A prospective descriptive study. Lancet Infect Dis 13: 36-42.
- Owens S, Abdel-Rahman IE, Balyejusa S, Musoke P, Cooke RP, et al. (2007) Nasopharyngeal aspiration for diagnosis of pulmonary tuberculosis. Arch Dis Child 92: 693-696.
- Domínguez Fenolle P, Cenarro Guerrero T, Rivas Chamorro A, Rituerto Gómez B, Franco López Y, et al. (1991) Tuberculosis: epidemiologic and clinical study of 268 paediatric patients. An Esp Pediatr 35: 26-30.
- Ibe M, Mori M, Mitsuda T, Aihara Y, Yokota S (1997) Analysis of children with tuberculosis in the past 20 years. Kansenshogaku Zasshi 71: 513-521.