
Case Report
*Address for Correspondence: Ashraf M Aly, Department of Pediatrics, Division of Pediatric Cardiology University of Texas Medical Branch, Texas, 301 University Blvd, Galveston, TX, 77555, USA, Tel: (409) 772-22341; Fax: (409) 772-3680; E-mail: amaly@utmb.edu
Citation: Asrani P, Sahni M, Aly AM, Jain S. Chylous Pericardial Effusion and Tamponade Due to Catheter Induced Superior Vena Caval Obstruction in a Premature Infant. J Pediatrics Child Care. 2015;1(1): 3.
Copyright © 2015 Aly et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 1, Issue: 1
Submission: 13 April 2015 | Accepted: 30 April 2015 | Published: 07 May 2015
Reviewed & Approved by: Dr. Bryan Burnette, Associate Professor of Clinical Pediatrics, Vanderbilt University School of Medicine, USA



Chylous Pericardial Effusion and Tamponade Due to Catheter Induced Superior Vena Caval Obstruction in a Premature Infant
Priyanka Asrani, Mitali Sahni, Ashraf M Aly* and Sunil Jain
- Department of Pediatrics, University of Texas Medical Branch, 301 University Blvd, Galveston, TX, 77555, USA
*Address for Correspondence: Ashraf M Aly, Department of Pediatrics, Division of Pediatric Cardiology University of Texas Medical Branch, Texas, 301 University Blvd, Galveston, TX, 77555, USA, Tel: (409) 772-22341; Fax: (409) 772-3680; E-mail: amaly@utmb.edu
Citation: Asrani P, Sahni M, Aly AM, Jain S. Chylous Pericardial Effusion and Tamponade Due to Catheter Induced Superior Vena Caval Obstruction in a Premature Infant. J Pediatrics Child Care. 2015;1(1): 3.
Copyright © 2015 Aly et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 1, Issue: 1
Submission: 13 April 2015 | Accepted: 30 April 2015 | Published: 07 May 2015
Reviewed & Approved by: Dr. Bryan Burnette, Associate Professor of Clinical Pediatrics, Vanderbilt University School of Medicine, USA
Abstract
Chylous pericardial effusion and tamponade in children are rare complications of thoracic duct injury during cardiothoracic surgeries or as a result of superior vena cava (SVC) obstruction. We report a rare case of chylous tamponade in a premature infant as a complication of long standing central venous catheterization resulting in SVC obstruction. Urgent pericardiocentesis and then surgical creation of a pericardial window resulted in complete resolution of the effusion and recovery of the patient.Keywords
Chylopericardium; Pericardial effusion; Pericardial tamponadeIntroduction
Central venous catheters (CVCs) are more frequently used in the neonatal intensive care units as the birth rate and survival of premature infants increase. They provide long-standing central venous access for the administration of fluids, medications and nutrition. The most common complications of CVC placement are mechanical dislodgment, perforation, thrombosis, catheter obstruction and sepsis [1]. Other reported complications include arrhythmias, systemic and pulmonary embolization, pericardial and pleural effusions, pulmonary infarction and pulmonary hemorrhage [2]. Although rare pericardial effusion with cardiac tamponade in the neonate is one of the potentially serious complications of central venous catheters with a prevalence of 1-3%, and a high mortality rate of 30-50% [2].Case Report
A thirty-six week gestation premature female infant was born via cesarean section. The pregnancy was complicated with a congenital diaphragmatic hernia and cardiac dextroposition. Postnatal 2-D echocardiogram showed normal cardiac anatomy and function and severe pulmonary hypertension. She required ECMO for the first 8 days of life. Surgical repair of the diaphragmatic hernia was performed at 2 weeks of age. A central venous catheter was needed for the administration of medications and for hyper-alimentation. The CVC was inserted in the SVC via the right internal jugular vein. At 3 months of age, she developed respiratory distress and edema of the upper chest, head and neck. A CXR showed an enlarged cardiac silhouette (Figure 1). An echocardiogram showed a massive pericardial effusion causing diastolic collapse of the right atrial posterior wall consistent with cardiac tamponade (Figure 2). Urgent pericardiocentesis was performed with aspiration of 50 cc of milky fluid that had triglycerides 413 mg/dl, protein 4.2 g/dl and WBC 2232/ dl with 89% lymphocytes. These values were suggestive of the chylous nature of the pericardial effusion. A pigtail catheter was placed for continuous drainage of the fluid. A magnetic resonance venogram (MRV) showed no clear flow related enhancement in both internal jugular vein and SVC. There were small collateral veins visualized in the neck (Figure 3). This indicated complete obstruction of both veins. The patient continued to accumulate significant amount of fluid despite being on octreotide. A surgical pericardial window was created and the CVC was subsequently removed with gradual clinical improvement. There was complete resolution of the swelling by 4 months of age. The patient continued to thrive well without any recurrence of the pericardial effusion as shown by echocardiography at one year of age.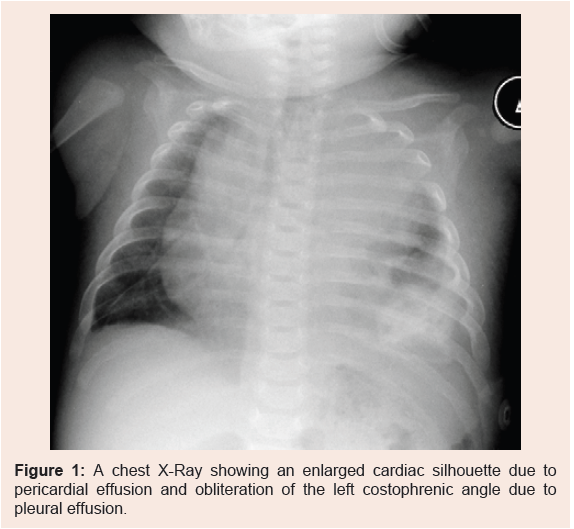
Figure 1: A chest X-Ray showing an enlarged cardiac silhouette due topericardial effusion and obliteration of the left costophrenic angle due to pleural effusion.
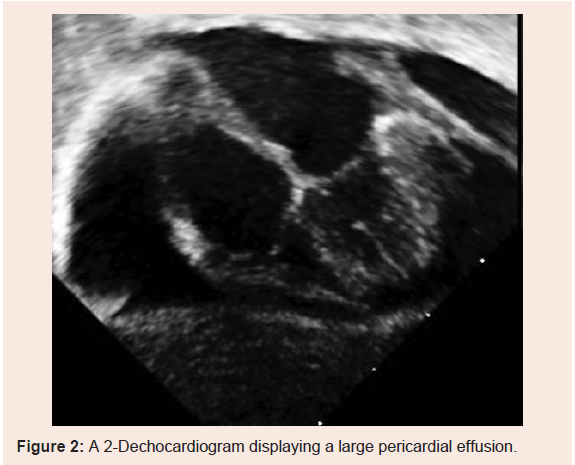
Figure 2: A 2-Dechocardiogram displaying a large pericardial effusion.
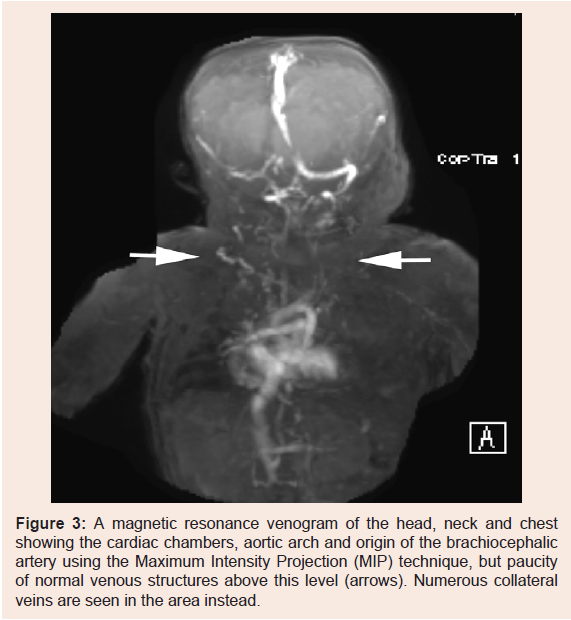
Figure 3: A magnetic resonance venogram of the head, neck and chest showing the cardiac chambers, aortic arch and origin of the brachiocephalic artery using the Maximum Intensity Projection (MIP) technique, but paucity of normal venous structures above this level (arrows). Numerous collateral veins are seen in the area instead.
Discussion
Chylous pericardial effusion may occur after cardiothoracic surgery, or in association with congenital lymphangiomatosis, chest trauma, mediastinal radiation and malignancy. It may also be due to thrombosis of the subclavian vein and superior vena cava [3]. There are very few reported cases of chylopericardium in association with superior vena cava and/or subclavian vein thrombosis [3]. SVC stenosis was described in an adult hemodialys is patient due to a long standing CVC leading to chylothorax and chylouspericardial tamponade [4]. Another case of chylopericaridum and bilateral chylothorax was described in a 16-year-old girl with Li Fraumeni syndrome after stem cell transplant. This was attributed to obstruction of the lymphatic flow due to thrombosis and stenosis of the SVC after prolonged use of multiple CVCs [5]. Idiopathic chylopericardium has also been described, most commonly in older children and young adults [3].In neonates, chylous pericardial effusion is commonly seen after cardiac and thoracic surgeries [6-8]. Central venous catheterization is a rare cause of chylous pericardial effusion in neonates and is commonly attributed to myocardial damage and perforation of the right atrium by the CVC tip [2]. In 2002, the U.S. Food and Drug Administration (FDA) recommended that the catheter tip should be maintained outside the right atrium, and that the neonate’s movements should be minimized in order to keep the catheter from migrating into the right atrium [9]. However, in one reported autopsy case of a premature infant, chylous pericardial effusion was presumed to have occurred due to permeation of hyper osmotic TPN contents into the pericardial sac. This occurred despite of appropriate position of the catheter tip proximal to the right atrium and there was no gross or microscopic myocardial damage [2]. Recently, a lethal case of chylous pericardial effusion and tamponade due to a catheter-induced thrombosis of intra thoracic veins (internal jugular vein, innominate, subclavian and axillary) was reported in a newborn infant [10].
Based on histological changes in the human venous wall adjacent to indwelling CVCs, 2 distinct microscopic patterns were observed in short-term catheters (<14 days) as compared to long-term catheters (> 90 days). The short-term catheters displayed foci of local intimalinjury with endothelial denudation and a layer of adherent thrombus. The second pattern, seen in the long-term catheters, consisted of smooth muscle cell proliferation leading to thickening of the venous wall. Three types of catheter-induced thrombus have been described: a) a mesh like thrombus, b) a non-organized form of thrombus and c) a mural thrombus [11].
We report a rare case of a SVC obstruction in a premature infant causing massive chylous pericardial effusion without a documented surgical injury of the thoracic duct. This obstruction was likely caused by either a thrombus formation or smooth muscle proliferation in the vessel wall causing stenosis. This resulted in increased central venous pressure and subsequently an increase in the thoracic duct luminal pressure with leakage of chylous fluid from the lymphatics into the pericardial and pleural sacs. Since no thrombi were identified by the MRV in any of the major intra thoracic veins, it is less likely to be the cause of obstruction. It is also unlikely that permeation of TPN contents into the pericardial sac would have presented with chylous pericardial effusion 2.5 months after catheter insertion. In previous literature, this was described to occur between 0-37 days with a median of 3 days between catheter placement and occurrence of symptoms [2]. It is therefore likely in this case that the obstruction was caused by smooth muscle proliferation in the venous structures.
Small and moderate size chylous pericardial effusions usually resolve with time and may benefit from octreotide supplementation. Pericardiocentesis and drainage are usually needed for large and symptomatic effusions. The central venous catheters are foreign bodies and have many potential complications; they need to be removed as soon as the clinical situation permits. Removal of the CVC in our patient, in addition to drainage of the effusion was associated with complete resolution of the symptoms.
Conclusion
We describe a rare case of chylous pericardial effusion and tamponade secondary to SVC obstruction in a premature infant. Pericardiocentesis and drainage of the effusion in addition to removal of the CVC may be necessary and could be life saving measures.References
- Goutail-Flaud MF, Sfez M, Berg A, Laguenie G, Couturier C, et al. (1991) Central venous catheter-related complications in newborns and infants - a 587-case survey. J Pediatr Surg 26: 645-650.
- Warren M, Thompson KS, Popek EJ, Vogel H, Hicks J (2013) Pericardial effusion and cardiac tamponade in neonates: sudden unexpected death associated with total parenteral nutrition via central venous catheterization. Ann Clin Lab Sci 43: 163-171.
- Lee N, Coco M (2006) Chylous pericardial tamponade in a haemodialysis patient with catheter-associated thrombosis of internal jugular and subclavian veins. Nephrol Dial Transplant 21: 2650-2653.
- Adekile A, Adegoroye A, Tedla F, Levin D, Salifu MO (2009) Chylothorax and chylopericardial tamponade in a hemodialysis patient with catheter-induced superior vena cava stenosis. Semin Dial 22: 576-579.
- Alkayed K, Plautz G, Gowans K, Rosenthal G, Soldes O, et al. (2013) Chylopericardium and chylothorax: Unusual mechanical complications of central venous catheters. Pediatr Int 55: e4-e6.
- Sykes JA, Verma R, Peshkovsky C, O'Connor B, Malik F, et al. (2012) Early repair of large infant ventricular septal defect despite respiratory syncytial virus-induced respiratory failure with postrepair chylous pericardial effusion requiring pleuropericardial window a case report and review of the literature. Pediatr Emerg Care 28: 1072-1077.
- Tchervenkov CI, Dobell AR (1985) Chylopericardium following cardiac-surgery. Can J Surg 28: 542-543.
- Papaioannou Y, Vomvoyannis A, Andritsakis G (1984) Combined chylopericardium and chylothorax after total correction of fallot's tetralogy. Thorac Cardiovasc Surg 32: 115-116.
- Yoder D (2001) Cardiac perforation and tamponade: the deadly duo of central venous catheters. Int J Trauma Nurs 7: 108-112.
- Rajpal MN, Buechler LS, Rao R (2013) Chylous cardiac tamponade due to catheter-associated thrombosis of intrathoracic veins in a newborn infant. J Pediatr Surg Case Rep 1: 180-182.
- Forauer AR, Theoharis C (2003) Histologic changes in the human vein wall adjacent to indwelling central venous catheters. J Vasc Interv Radiol 4: 1163-1168.