
Case Report
*Address for Correspondence: Ahmad Nasrat Al-Juboori, Professor and Consultant Otorhinolaryngologist, Head and Neck Surgeon (F.I.C.M.S, EBE ORL-HNS), College of Medicine, Al-Iraqia University, Al-Adhamyia, Baghdad, Iraq, Tel: +9647902892674; E-mail: ahmednas2005@yahoo.com, aljubooriahmad@gmail.com
Citation: Citation: Al-Juboori AN. Safety of Cold Tonsillectomy Techniques: Comparison between Wired Snare and Inferior Tonsillar Pole Ligation Methods. 2016;3(1): 4.
Copyright © 2016 Al-Juboori AN, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolaryngology| ISSN: 2380-0569 | Volume: 3, Issue: 1
Submission: 14 March, 2016 | Accepted: 05 May, 2016 | Published: 09 May, 2016
Safety of Cold Tonsillectomy Techniques: Comparison between Wired Snare and Inferior Tonsillar Pole Ligation Methods
Ahmad Nasrat Al-Juboori*
- Professor and Consultant Otorhinolaryngologist, Head and Neck Surgeon (F.I.C.M.S, EBE ORL-HNS), College of Medicine, Al-Iraqia University, Al-Adhamyia, Baghdad, Iraq
*Address for Correspondence: Ahmad Nasrat Al-Juboori, Professor and Consultant Otorhinolaryngologist, Head and Neck Surgeon (F.I.C.M.S, EBE ORL-HNS), College of Medicine, Al-Iraqia University, Al-Adhamyia, Baghdad, Iraq, Tel: +9647902892674; E-mail: ahmednas2005@yahoo.com, aljubooriahmad@gmail.com
Citation: Citation: Al-Juboori AN. Safety of Cold Tonsillectomy Techniques: Comparison between Wired Snare and Inferior Tonsillar Pole Ligation Methods. 2016;3(1): 4.
Copyright © 2016 Al-Juboori AN, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolaryngology| ISSN: 2380-0569 | Volume: 3, Issue: 1
Submission: 14 March, 2016 | Accepted: 05 May, 2016 | Published: 09 May, 2016
Abstract
Objective: The aim of this study was to assess the safety of wired snare method compared with inferior tonsillar pole ligation method as techniques used in cold dissection tonsillectomy.Study design: Prospective, case series study with six months follow up.
Setting: Al-Fallujah Teaching Hospital, Al-Anbar, Iraq.
Subjects and methods: This was a hospital based prospective study performed in the Department of Ear, Nose and Throat, from July 2012 to June 2013, during this period 210 patients underwent tonsillectomy by same surgeon. Tonsillectomy done by cold dissection technique, one side the inferior tonsillar pole ligated by silk, the other side in the same patient, the inferior pole had been taken with cold wire snare, the selection done randomly. Bipolar diathermy forceps were used for tonsillar bed homeostasis adenoidectomy done by curettage if indicated. Follow up continued for the next six months.
Results: The indication for tonsillectomy was mainly due to recurrent acute or chronic tonsillitis (75.2%). Early complications as primary bleeding happened more with wired snare method (four times) as well as the reactionary hemorrhage, on the other hand the anesthetic complications (four times), trauma to base of tongue and tonsillar remnant happened more with inferior tonsillar pole ligation method. Late complications were very limited after both procedures.
Conclusion: From this study we concluded that wired snare method carried more risk of bleeding, while inferior tonsillar pole ligation method associated with more anesthetic, traumatic and tonsillar remnant complications.

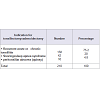
 The indication for tonsillectomy was mainly due to recurrent acute or chronic tonsillitis (75.2%), snoring with or without sleep apnea syndrome (20%) and peritonsillar abscess (quinsy) which happened in 4.8%, as shown in Table 2.
The indication for tonsillectomy was mainly due to recurrent acute or chronic tonsillitis (75.2%), snoring with or without sleep apnea syndrome (20%) and peritonsillar abscess (quinsy) which happened in 4.8%, as shown in Table 2.
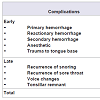
 Anesthetic complications occurred during surgical procedure manifested as depressed oxygen saturation, which was happened in three patients who underwent ITPL method and non in patients with WS method. Couple of patients developed trauma to base of tongue with ITPL method, as shown in Table 3.On the other hand, the late complications were very limited in form of recurrence of snoring happened three patients, recurrence of sore throat occurred in four patient and change of voice happened in three patient. Tonsillar remnant happened in three sides with ITPL method, as shown in Table 3.
Anesthetic complications occurred during surgical procedure manifested as depressed oxygen saturation, which was happened in three patients who underwent ITPL method and non in patients with WS method. Couple of patients developed trauma to base of tongue with ITPL method, as shown in Table 3.On the other hand, the late complications were very limited in form of recurrence of snoring happened three patients, recurrence of sore throat occurred in four patient and change of voice happened in three patient. Tonsillar remnant happened in three sides with ITPL method, as shown in Table 3.
Keywords
Tonsillectomy complications; Dissection method; Wired snare; Ligation inferior tonsillar poleIntroduction
Tonsillectomy (surgical removal of the tonsils) has been practiced since antiquity [1]. The first known removal of tonsils dates back to the first century AD, when Cornelius Celsius in Rome used his own finger to perform it [2]. Tonsillectomy is one of the commonest otolaryngological procedures performed, representing approximately 20%-40% of surgical procedures performed in this field [3,4]. Various surgical techniques are used to perform this operation, including blunt dissection, guillotine excision, electrocautery, cryosurgery, coblation, ultrasonic removal, laser removal, monopolar and bipolar dissection, thermal welding tonsillectomy, and ligature tonsillectomy [5]. There is no uniform technique of tonsillectomy throughout the world and the choice of the technique depends on the surgeon´s preference. Different tonsillectomy techniques have different impact on postoperative morbidity [6]. Generally tonsillectomy is considered simple procedure but, in comparison with other similar operations, it implies a common and sometimes serious complication [7]. There are several techniques for tonsillectomy and their relative effectiveness remains a matter of debate. Each has its advantages and disadvantages and the method chosen by the surgeon has often depended on their personal preference based on training and experience. Traditionally, tonsillectomy has been performed by means of ´cold´ dissection. The tonsil and its capsule are separated from the surrounding peritonsillar) tissues using metal instruments [8]. The upper pole of the tonsil is mobilized first and dissection continues to the base of the tongue. A cold wire snare is used to ensure that a flat ´tongue´ of lymphoid tissue beyond the lower pole of the tonsil is removed with the tonsil proper [9]. Alternatively ligation of inferior tonsillar pole may be performed to achieve hemostasis [10].The aim of this study was to assess the safety of wired snare (WS) method compared with Inferior Tonsillar Pole Ligation (ITPL) method as techniques used in cold dissection tonsillectomy.
Subjects and Methods
This was a hospital based prospective study performed in the Department of ear, nose and throat, Al-Fallujah Teaching Hospital from July 2012 to June 2013. This study was approved by ethics committee of the hospital and informed consent had been secured from each patient or their parents, during this period, 210 patients underwent tonsillectomy and they were admitted for different indications. Preoperative information was obtained and reviewed including the age at the time of surgery, gender, indication for surgery. Preoperative investigations included blood examinations (hemoglobin level, prothrombin time, partial thromboplastin time and platelet count), and radiography of soft tissue of the postnasal space may be done if indicated. No antibiotics were given before the operations except for those with upper respiratory tract infection. The indications for surgery were recurrent acute or chronic tonsillitis, snoring with or without sleep apnea syndrome, and peritonsillar abscess (quinsy). Tonsillectomy done under general anesthesia with endotracheal intubation, and the patient with standard tonsillectomy position, a Boyle Davis gag is in situ. A mucosal incision was made with scissors between the tonsil and anterior pillar in keeping with a cold dissection technique i.e. the procedure done by cold dissection method, one side the lower tonsillar pole taken by Negus artery forceps and ligated by 3/0 silk Figure 1a.The opposite tonsillar side in the same patient, the lower pole had been taken with cold wire snare randomly Figure 1b, this means that selection of right or left side were chosen randomly for each technique. Bipolar diathermy forceps were used for tonsillar bed hemostasis. Adenoidectomy underwent by curettage if indicated. The assessment of blood loss quantity is done by measuring the amount of blood loss and the number of swabs used in each side. Data was collected intra-operatively and during the first 24 hours post-operative, the follow up continued for the coming two weeks after the procedure as well as for the next six months either by visits or by phone. Bleeding during tonsillectomy, i.e. primary hemorrhage was very important complication, reactionary hemorrhage happened within the first 24 hours after tonsillectomy, while secondary hemorrhage occurred after the first postoperative day after the procedure as a result of infection.
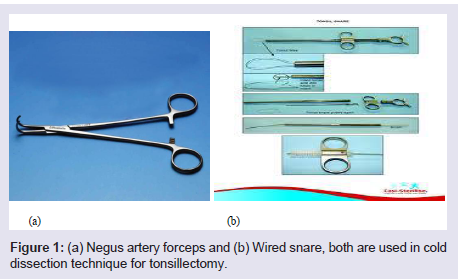
Figure 1: (a) Negus artery forceps and (b) Wired snare, both are used in colddissection technique for tonsillectomy.
Results
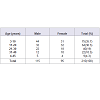
The total number of the patients who underwent tonsillectomy by cold dissection method was 210 patients; they ranged from 3-45 years. The mean age was 14.6 years with standard deviation ±2.1. They were 115 males and 95 females with female:male ratio 1:1.2 as shown in Table 1.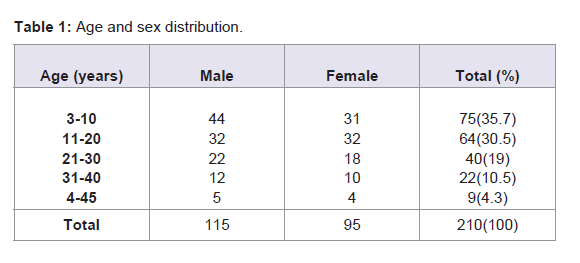
Table 1: Age and sex distribution.
Early complication of WS method compared with ITPL method as techniques used in cold dissection tonsillectomy means that complications happened during surgical procedure as a result of different technique used. Primary hemorrhage happened in four sides ith WS method and in one side with ITPL method. Reactionary hemorrhage occurred in two sides with WS method, while secondary hemorrhage developed in one side after each method, so that over all patients who developed primary hemorrhage were 5 sides (2.3%), reactionary hemorrhage were 2 sides (0.95%) and secondary hemorrhage were 2 sides (0.95%).
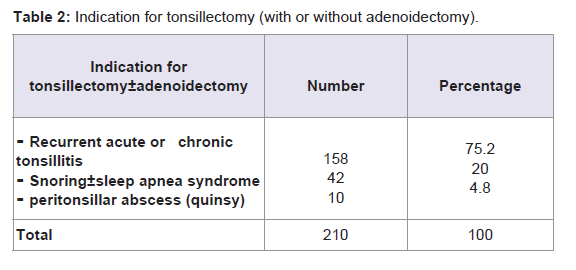
Table 2: Indication for tonsillectomy (with or without adenoidectomy).
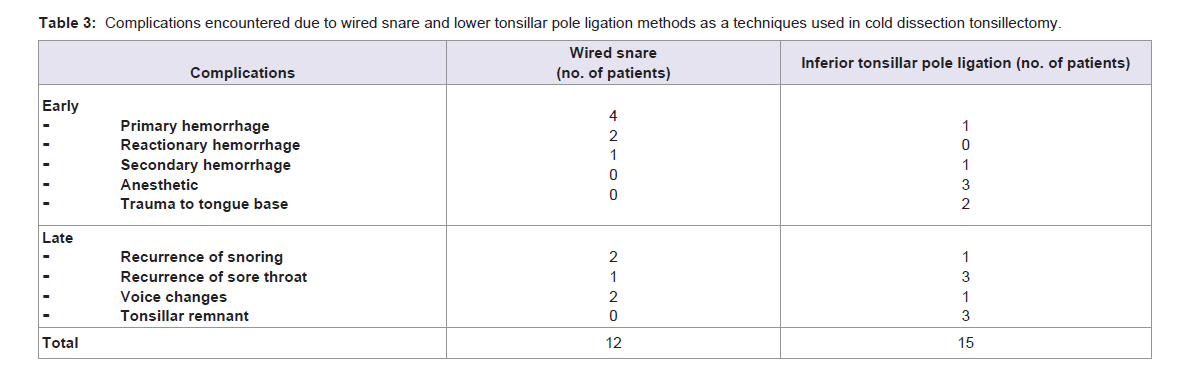
Table 3: Complications encountered due to wired snare and lower tonsillar pole ligation methods as a techniques used in cold dissection tonsillectomy.
Discussion
A tonsillectomy is one of the most common operations performed in the world. Various surgical procedures for tonsillectomy are performed with a wide array of opinions to support the pros and cons of each technique [11]. This article highlighted upon the comparison between WS method and ITPL method. Primary and reactionary bleeding are generally considered to be related to surgical technique whereas environmental factors that influence oropharyngeal healing contribute to delayed (secondary) hemorrhage [12,13]. Some researchers showed post-tonsillectomy bleeding (PTB) rates of 5.1 percent in adults and PTB rates of 6.75 percent in pediatric patients. In a literature based study by Blakley, he concluded that PTB rates of about 5 percent are typical [14]. In a recent study by D´Agostino et al. on 3306 patients undergoing elective adenotonsillectomy by five senior surgeons with different surgical techniques, they found late post-operative hemorrhage rate of 1.78% which started all at home [15]. Benson and Mitchell found that 16% of children had experienced some bleeding when contacted at 2 weeks postoperatively [16]. Raut found 16.9% secondary hemorrhage rate in 200 patients while assessing 15-17 days postoperatively [17]. Blogmren found that 32.8% of a mixed adult and pediatric population had experienced some secondary hemorrhage following tonsillectomy [18]. However, in a number of previous studies the secondary hemorrhage rate was much higher in comparison with our study.Bleeding is the major source of morbidity and mortality of tonsillectomy and most operative time is spent securing hemostasis [10,19]. The bleeding was less in ITPL method probably due to dealing with offending bleeders by competent and secured way of hemostasis which was the ligation, this phenomenon seen also by others. Sharp et al. showed that swab blood loss was significantly lower for surgeons who ligated the lower tonsillar pole, compared with surgeons who used a snare [10]. The variety of powered instrument such as coblator, ultrasound dissection and diathermy has greatly reduced the risk of primary and reactionary hemorrhage among the patients. Wired snare method seen superior to ITPL method regarding anesthetic complications in form of suppressed oxygen saturation, this issue may be due to manipulation of the endotracheal tube by Negus artery forceps during hemostasis especially when non fenestrated tongue blade used and the tube forced to be on either side and not in the mid line, or because of dislodgement of the tube after withdrawing after release of the artery forceps especially if non cuffed tube used in small children. Trauma to the tongue base also recorded with use of ITPL method after crushing the lower pole by artery forceps, this was not seen in WS method.
Patients operated with tonsillar surgery report a high degree of symptom relief six months after surgery [20,21], this was consistent with the results of this study, but there were limited number of patients developed recurrence of snoring and sore throat, and those were more with the ITPL group, the explanation probably because of a remnant of tonsillar tissue which later on causing recurrence of symptoms or even re-growth of tonsillar tissue in the bed of surgical field.
The use of ITPL is advisable as compared to WS technique to minimize the rate of PTB which is the main morbid problem posttonsillectomy, but we should but in our consideration the possibility of post-operative tonsillar remnant, and in order to avoid this complication, proper dissection and ligation as much as to tonsillolingual sulcus is indicated with the assistance of cuffed endotracheal intubation to get rid of anesthetic complication.
Conclusion
From this study we concluded that wired snare method carried more risk of bleeding, while inferior tonsillar pole ligation method associated with more anesthetic, traumatic and tonsillar remnant complications.References
- Younis RT, Lazar RH (2002) History and current practice of tonsillectomy. Laryngoscope 112 (8 Pt 2 Suppl 100): 3-5.
- Curtain JM (1987) The history of tonsil and adenoid surgery. Otolaryngol Clin North Am 20: 415-419.
- Ahsan F, Rashid H, Eng C, Bennett DM, Ah-See KW (2007) Is secondary hemorrhage after tonsillectomy in adults an infective condition? Objectivemeasures of infection in a prospective cohort. Clin Otolaryngol 32: 24-27.
- Evans AS, Khan AM, Young D, Adamson R (2003) Assessment of secondary hemorrhage rates following adult tonsillectomy--a telephone survey and literature review. Clin Otolaryngol Allied Sci 28: 489-491.
- Karatzanis A, Bourolias C, Prokopakis E, Panagiotaki I, Velegrakis G (2008) Thermal welding technology vs ligature tonsillectomy: a comparative study. Am J Otolaryngol 29: 238-241.
- Windfuhr JP, Wienke A, Chen YS (2009) Electrosurgery as a risk factor for secondary post-tonsillectomy hemorrhage. Eur Arch Otorhinolaryngol 266: 111-116.
- D´Agostino R, Tarantino V, Calevo MG (2009) Post-tonsillectomy late hemorrhage: is it a preferably night time event? Int J Pediatr Otorhinolaryngol 73: 713-716.
- Burton MJ, Doree C (2009) Coblation versus other surgical techniques for tonsillectomy (Review). The Cochrane Collaboration and published in The Cochrane Library.
- Ballantyne JC, Harrison DF (1986) Rob & Smith’s operative surgery: nose and throat, (4thedn). London, Butterworths.
- Sharp JF, Rogers MJ, Riad M, Kerr AI (1991) Combined study to assess the role of calcium alginate swabs and ligation of the inferior tonsillar pole in the control of intra-operative blood loss during tonsillectomy. J Laryngol Otol 105: 191-194.
- Young C, MacRae J (2001) Tonsillectomy. A comparative study of dissection/ snare vs suction-cautery. Can Oper Room Nurs J 19: 7-11.
- Windfuhr JP, Schloendorff G, Baburi D, Kremer B (2008) Life threatening posttonsillectomy hemorrhage. Laryngoscope 118: 1389 1394.
- Walker P, Gillies D (2007) Post tonsillectomy hemorrhage rates: are they technique-dependent? Otolaryngol Head Neck Surg 136(4 Suppl): S27 S31.
- Blakley BW (2009) Post tonsillectomy bleeding: how much is too much? Otolaryngol Head Neck Surg 140: 288 290.
- Boo D´Agostino R, Tarantino V, Calevo MG (2009) Post-tonsillectomy late hemorrhage: is it a preferably night-time event? Int J Pediatr Otorhinolaryngol 73: 713-716.
- Benson-Mitchell R, Maw AR (1993) Assessment of sequelae at homefollowing adenotonsillectomy. A basis for day-case management? Clin Otolaryngol Allied Sci 18: 282-284.
- Raut V, Bhat N, Kinsella J, Toner JG, Sinnathuray AR, et al. (2001) Bipolar scissors versus cold dissection tonsillectomy: a prospective, randomised, multi-unit study. Laryngoscope 111: 2178-2182.
- Blomgren K, Qvarnberg YH, Valtonen HJ (2001) A prospective study on pros and cons of electrodissection tonsillectomy. Laryngoscope 111: 478-482.
- Windfuhr JP, Chen YS (2003) Post-tonsillectomy and -adenoidectomyhemorrhage in nonselected patients. Ann Otol Rhinol Laryngol 112: 63-70.
- Stalfors J, Ericsson E, Hemlin C, Hultcrantz E, Månsson I, et al. (2012) Tonsil surgery efficiently relieves symptoms: analysis of 54 696 patients in the National Tonsil Surgery Register in Sweden. Acta Otolaryngol 132: 533-539.
- Clayburgh D, Milczuk H, Gorsek S, Sinden N, Bowman K, et al. (2011) Efficacy of tonsillectomy for pediatric patients with Dysphagia and tonsillar hypertrophy. Arch Otolaryngol Head Neck Surg 137: 1197-1202.