
Case Report
*Address for Correspondence: Fransiska Hutahaean, MD, Department of Otorhinolaryngology-Head & Neck Surgery, Universitas Airlangga/Dr. Soetomo Hospital, Mayjend. Prof. Dr. Moestopo 6-8, Surabaya, Indonesia, Tel: +62 8785269 5838; E-mail: siskafk94@yahoo.com
Citation: Romdhoni AC, Hutahaean F. Giant Retropharyngeal Lipoma. Inter J Otorhinolaryngology. 2015;2(2): 4.
Copyright © 2015 Hutahaean et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolarygology | ISSN: 2380-0569 | Volume: 2, Issue: 2
Submission: 11 August 2015 | Accepted: 19 September 2015 | Published: 22 September 2015
 Tracheotomy and transcervical resection (U-shaped incision) were performed. Tumor mass was released from surrounding tissue, such as the carotid artery, bilateral jugular vein, esophagus, and trachea and was removed intoto. Its weighted 850 grams with a size of 19 cm x 14 cm x 7 cm. Pathologic examinations confirmed a benign noninfiltrating lipoma, consists of mature fat cell proliferation, monotonous with fibrous connective tissue of which referredto fibrolipoma appearance ( Figure 2).
Tracheotomy and transcervical resection (U-shaped incision) were performed. Tumor mass was released from surrounding tissue, such as the carotid artery, bilateral jugular vein, esophagus, and trachea and was removed intoto. Its weighted 850 grams with a size of 19 cm x 14 cm x 7 cm. Pathologic examinations confirmed a benign noninfiltrating lipoma, consists of mature fat cell proliferation, monotonous with fibrous connective tissue of which referredto fibrolipoma appearance ( Figure 2).
 After surgery, all symptoms disappeared and the tracheotomy could be closed. The postoperative course has been good so far.
After surgery, all symptoms disappeared and the tracheotomy could be closed. The postoperative course has been good so far.
From all cases that were found during 1887-2013, lipoma size varies however shows a pattern of the same size over the period 1912-2001 with range between 150-250 cm3 and tend to fluctuate since this time. Moreover, the biggest size continues to increase, especially in 2006, 2007, 20011, 2013 and 2014. The increasing of the size occurred two to four times, about 250 cm3 in early 1900, increased to 400 cm3 in a hundred years later (2006) and continues to increase within shorter time cycles (five years) to about 800 cm3 and finally increased to about 1800 cm3 in 2014. From ( Figure 3) below clearly shows that the size of the retropharyngeal lipoma operated at Hospital Dr. Soetomo, it is the largest single lipoma in history (giant lipoma). Retropharyngeal is a wide space, from the base of the skull to the superior of mediastinum. Lipoma in this space will give various symptoms, depending on the affected part of aero digestive tract, such as nasal obstruction, tightness, hoarseness, snoring, and a sense of prop when swallowing food, depend on the location and size of the tumor [3,6,10-11]. The patient had early symptoms of nasal obstruction during sleeping on right side and prop sense when swallowing, followed by longer process of swallowing, snoring, hoarseness, and dyspnea while sleeping.
Retropharyngeal is a wide space, from the base of the skull to the superior of mediastinum. Lipoma in this space will give various symptoms, depending on the affected part of aero digestive tract, such as nasal obstruction, tightness, hoarseness, snoring, and a sense of prop when swallowing food, depend on the location and size of the tumor [3,6,10-11]. The patient had early symptoms of nasal obstruction during sleeping on right side and prop sense when swallowing, followed by longer process of swallowing, snoring, hoarseness, and dyspnea while sleeping.
Giant Retropharyngeal Lipoma
Achmad C. Romdhoni, Fransiska Hutahaean*, Chippy Ahwil and Ibnu Haris Fadillah
- Department of Otorhinolaryngology-Head & Neck Surgery, Universitas Airlangga, Indonesia
*Address for Correspondence: Fransiska Hutahaean, MD, Department of Otorhinolaryngology-Head & Neck Surgery, Universitas Airlangga/Dr. Soetomo Hospital, Mayjend. Prof. Dr. Moestopo 6-8, Surabaya, Indonesia, Tel: +62 8785269 5838; E-mail: siskafk94@yahoo.com
Citation: Romdhoni AC, Hutahaean F. Giant Retropharyngeal Lipoma. Inter J Otorhinolaryngology. 2015;2(2): 4.
Copyright © 2015 Hutahaean et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolarygology | ISSN: 2380-0569 | Volume: 2, Issue: 2
Submission: 11 August 2015 | Accepted: 19 September 2015 | Published: 22 September 2015
Introduction
Lipoma in the head and neck is relatively rare and retropharyngeal lipoma is even rarer in this area. Not more than 45 cases of lipoma retropharyngeal have been found in the literature since 1877 to 2014. It is a benign tumor that consists of adipose tissue cells, which appears as a soft mass without any severe symptoms unless it reaches large size [1]. Literature reported that the tumor was discovered accidentally when a computed tomography (CT) scan of the head and neck for other diseases was performed [2,3]. Retropharyngeal lipoma usually occurs in adults over the age of 35 years [4], although in children aged 11 and 12 years have also been reported in the literature [5,6]. Therapy will be a transoral or transcervical approach of excision. Low prevalence rates in the world makes a discussion about this disease to be interesting; especially case that occured in Dr. Soetomo Hospital is a retropharyngeal lipoma with a relatively large size.Case Report
A 44-year-old man, presented with a 2-year history of abnormal sensation in the throat and progressive dysphagia. He was admitted to our hospital in January 2014 due to dyspnea, dysphagia, speech disturbance, and obstruction in the nose. Physical and endoscopic examinations revealed a neck swelling and bulging of the posterior pharyngeal wall. X-ray films of the neck showed a large soft-tissue mass pushing the trachea forward. CT scan result was fat dominant lesion in retropharyngeal space as high as corpus VC 2 - VC 6, with a size of 10 cm x 5 cm x 10 cm. The lesion was pressing the posterior wall of the oropharynx and hypopharynx to the anterior and narrowing both structures. The lesion extended to the right and left region colli ( Figure 1). Fine needle aspiration biopsy was also failed because of oedema of the tissue and gave unrepresentative specimen.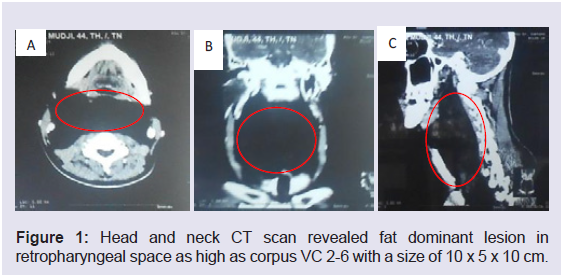
Figure 1: Head and neck CT scan revealed fat dominant lesion in retropharyngeal space as high as corpus VC 2-6 with a size of 10 x 5 x 10 cm.
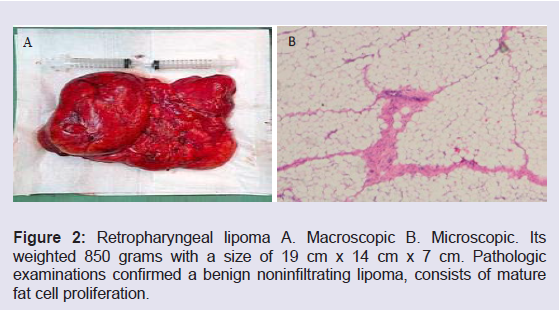
Figure 2: Retropharyngeal lipoma A. Macroscopic B. Microscopic. Its weighted 850 grams with a size of 19 cm x 14 cm x 7 cm. Pathologic examinations confirmed a benign noninfiltrating lipoma, consists of mature fat cell proliferation.
Discussion
Lipoma is a benign tumor that derived from fat cells and coated by capsule [7]. It is relatively rare occurrence in the head and neck, with the most frequent manifestation in this area is in posterior trigonum of the neck. Lipoma rarely found in the anterior colli, infratemporal fossa, oral cavity, larynx, nasopharynx or parapharyngeal space, and extremely rarely found in the retropharyngeal space [8,9]. Retropharyngeal lipoma case is not clearly described in the literature study, as shown in ( Table 1) that since 1877 until now, not more than 46 cases are reported, including this case.From all cases that were found during 1887-2013, lipoma size varies however shows a pattern of the same size over the period 1912-2001 with range between 150-250 cm3 and tend to fluctuate since this time. Moreover, the biggest size continues to increase, especially in 2006, 2007, 20011, 2013 and 2014. The increasing of the size occurred two to four times, about 250 cm3 in early 1900, increased to 400 cm3 in a hundred years later (2006) and continues to increase within shorter time cycles (five years) to about 800 cm3 and finally increased to about 1800 cm3 in 2014. From ( Figure 3) below clearly shows that the size of the retropharyngeal lipoma operated at Hospital Dr. Soetomo, it is the largest single lipoma in history (giant lipoma).
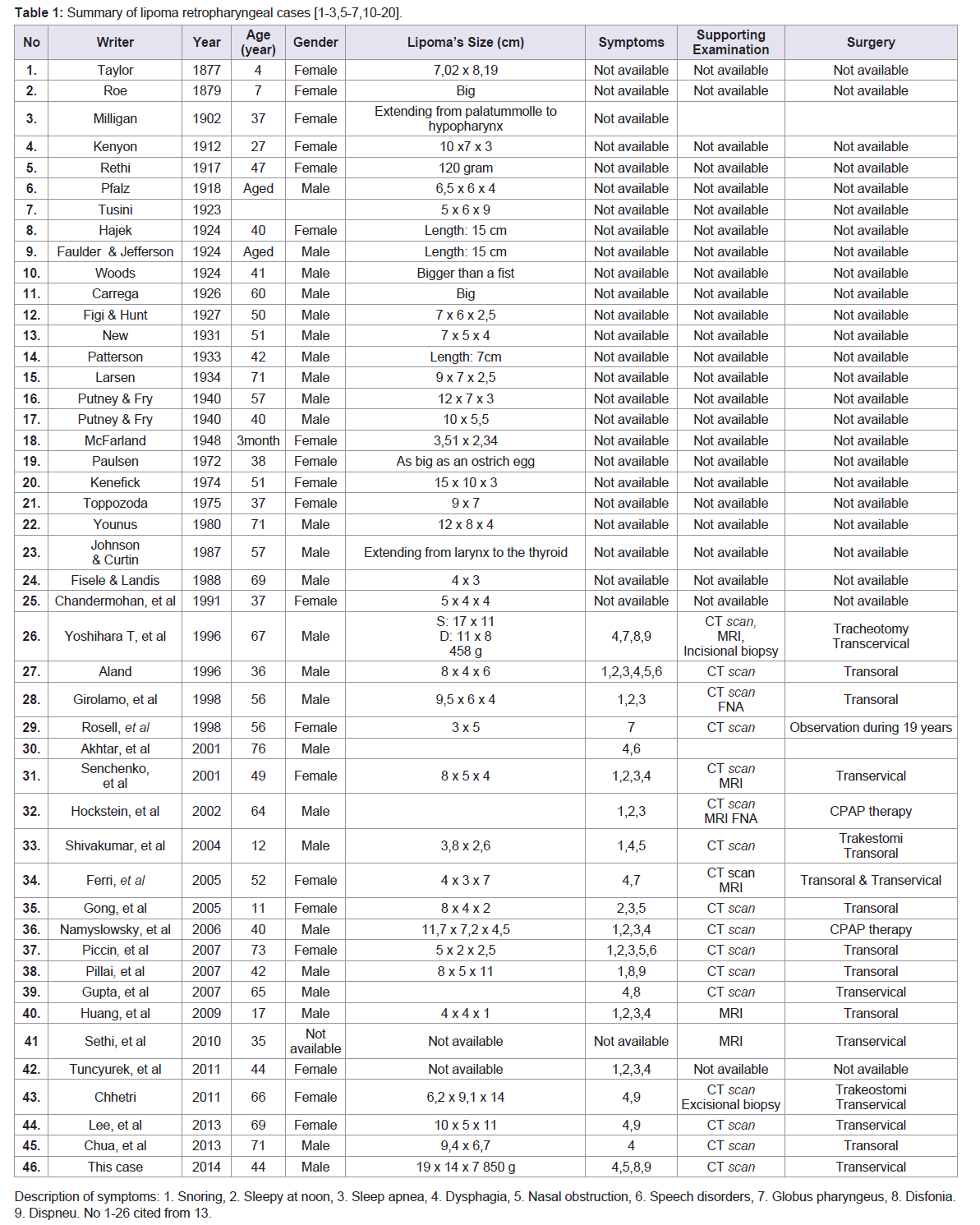
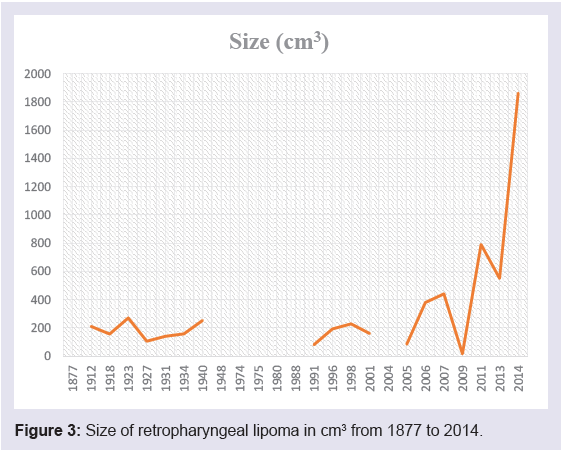
Figure 3: Size of retropharyngeal lipoma in cm3 from 1877 to 2014.
CT scan is helpful in diagnosing this disease preoperatively. Radiographic characteristics of lipoma retropharyngeal like typical lipoma in other parts of the body. Lipoma appears as a homogeneous period with low attenuation without a clear capsule that resembles the fat with -50 to -150 Hounse field Units (HU) [14]. CT scan or MRI will differentiate lipoma from liposarcoma retropharynx because both diseases are very different in terms of therapy. Surgery will not be enough for liposarcoma, but should be followed by chemoradiation [7].
Liposarcoma on MRI is shown as hyperintense lesions on T1 without using contrast, thickening septa, unrelated adipose mass, prominent foci with increasing T2 signal and protrusion of enhancement area. MRI has better contrast resolution, allowing the anatomical structure and boundaries of the tumor that looks better than CT scan. MRI also shows the spatial relationship of tumor and blood vessels more clearly [15]. In this case, specifically MRI couldn’t be performed due to the patient felt dyspnea in supine position. Large retropharyngeal lipoma will give pressure to aero digestivus tract causing difficulty in breathing and swallowing food, therefore it must be excisied.
Retropharyngeal lipoma surgery options can be trans-oral excision or transcervical. Each approach has its advantages and disadvantages. Transoral approach has the advantage of lower postsurgery morbidity, shorter hospitalization time, and no scar tissue on the neck. The disadvantage is not able to see the large blood vessels properly. This action is usually chose when the size of lipoma is not too large, though it isn’t impossible to do transoral approach in large lipoma as reported in Singapore, retropharyngeal lipoma which already extends into space of parapharynx successfully removed intoto with transoral approach. The procedure chosen by the consideration that lipoma has a capsule and can yield [16].
Transcervical approach is an option for a large lipoma because this approach gives a better surgical area, easier access so lipoma removal can be done by intoto. The disadvantage of this approach is the postsurgery morbidity is greater than transoral approach and there is a possibility damaging cranialis nerve and carotid artery [16]. In this case, transcervical excision was selected because very large tumor mass size 19 cm x 14 cm x 7 cm. Tracheotomy was performed first with the consideration of a difficult intubation. Literature reported airway management in a large lipoma retropharynx using glidescope for intubation in order to avoid tracheotomy before perfoming transcervical excision [17].
Macroscopically, lipoma may be single or lobulated, soft or sometimes felt cystic. Microscopically, lipoma is seen as aggregation of mature adipose cells which is coated by a thin capsule. Lipoma may be divided into several subclasses based on histology, that are classic lipoma (either solitary or multiple), fibrolipoma [18], angiolipoma, infiltrating lipomas, intramuscular lipoma, hibernoma, pleimorphic lipoma, lipoblastomastosis, and diffuse lipoblastomatosis [19]. Post-surgery, tissue was sent for pathological examination anatomy revealed macroscopic and microscopic pattern suitable for retropharyngeal fibrolipoma [20,21].
Generally, lipoma is rarely relapsing. In this patient, evaluation was undertaken in a month and seven months post-surgery respectively. It was concluded that no tumor recurrence was found on physical examination, fiber optic laryngoscopy, and CT scan.
Conclusion
Have reported a male patient, 44 years old, with giant retropharyngeal lipoma that has a size of 19 cm x 14 cm x 7 cm who has already been done tracheotomy and removal of the tumor through the transcervical approach. Evaluation seven months after surgery showed no recurrence obtained.References
- Radhakrishna Pillai OS, Vijayalakshmi S, Adarsha TV, Thahir M, Gupinathan UK, et al. (2007) Retropharyngeal lipoma - a case report. Indian J Otolaryngol Head Neck Surg 59: 360-362.
- Ferri E, Ianniello F, Armato E, Cavaleri S, Razavi IS, et al. (2005) Retro-parapharyngeal lipoma causing dysphagia: radiological findings and surgical management. Internet J Otorhinolaryngol 5.
- Hockstein NG, Anderson TA, Moonis G, Gustafson KS, Mirza N (2002) Retropharyngeal lipoma causing obstructive sleep apnea: case report including five-year follow-up. Laryngoscope 112: 1603-1605.
- Day TA, Joe JK (2005) Primary neoplasm of the neck. In: Cummings CW, Flent PW, Harker LA, Haughey BA, Richardson MA, et al. (eds.) Cummings: otolaryngology head and neck surgery. (4th edn), Elsevier, Philadelphia.
- Shivakumar AM, Naik AS, Shetty DK, Yogesh BS (2004) Lipoma of the retropharyngeal space. Indian J Pediatr 71: 271-272.
- Gong W, Wang E, Zhang B, Da J (2006) A retropharyngeal lipoma causing obstructive sleep apnea in a child. J Clin Sleep Med 2: 328-329.
- Chhetri DK (2011) Benign and malignant lipogenic tumors of the retropharyngeal space. Nepalese J ENT Head Neck Surg 2: 22-24.
- Anniko M (2010) Cyst and benign tumours of the neck. In: Anniko M, Bernal-Sprekelsen M, Bronkowsky V, Bradley P, Lurato S, (eds.) Otorhinolaryngology, head and neck surgery (1st edn), Springer, Leipzig.
- Mandpe AH (2012) Neck neoplasms and neck dissection. In: Lalwani AK, (ed.) Current diagnosis and treatment otolaryngology head and neck surgery. (3rd edn), The Mcgraw Hill Companies, New York.
- Yoshihara T, Kawano K, Mita N (1998) Retropharyngal lipoma causing severe dysphagia and dyspnea. J Otolaryngol 27: 363-366.
- Piccin O, Sorrenti G (2007) Adult obstructive sleep apnea related to nasopharyngeal obstruction: a case of retropharyngeal lipoma and pathogenetic considerations. Sleep Breath 11: 305-307.
- Namyslowski G, Scierski W, Misiolek M, Urbaniec N, Lange D (2006) Huge retropharyngeal lipoma causing obstructive sleep apnea: a case report. Eur Arch Otorhinolaryngol 263: 738-740.
- Akhtar J, Shaykhon M, Crocker J, D’Souza AR (2001) Retropharyngeal lipoma causing dysphagia. Eur Arch Otorhinolaryngol 258: 458-459.
- Lee HK, Hwang SB, Chung GH, Hong KH, Jang KY (2013) Retropharyngeal spindle cell/pleiomorphic lipoma. Korean J Radiol 14: 493-496.
- Chua DY, Lim MY, Teo DT, Hwang SY (2013) Retropharyngeal lipoma with parapharyngeal extension: is transoral excision possible? Singapore Med J 54: e176-e178.
- Gupta P, Deo RP, Udupa KV, Ravi HR, Pai SA (2007) A case of retropharyngeal lipoma. Indian J Surg 70: 40-41.
- Rosell A, Garcia-Arranz G, Llavero MT, Martinez-San-Millan J (1998) Imaging case study of the month. Lipoma of the retropharyngeal space. Ann Otol Rhinol Laryngol 107: 726-728.
- Huang HC, Li HY (2009) Retropharyngeal fibrolipoma: A counterchanging obstructive pattern in sleep apnea. Int J Pediatr Otorhinolaryngol 4: 45-48.
- Cappabianca S, Colella G, Pezzullo MG, Russo A, Iaselli F, et al. (2008) Lipomatous lesions of the head and neck region: imaging findings in comparison with histological type. Radiol Med 113: 758-770.
- Sethi S, Arora V (2010) Use of glidescope and external manipulation in airway management of an unusual retropharyngeal lipoma. J Anesthesiol Clin Pharmacol 26: 557-558.
- Tuncyurek O, Eyigor H, Ozkul A (2011) What is the importance of radiology in obstructive sleep apnea. J Craniofac Surg 22: 1971-1973.