
Case Report
Topical Phytotherapy: Management of Deranged Anatomical and Abnormal Biochemical Risk Factors during Failed Total Knee Arthroplasty: A Unique Case Study
Apurba Ganguly* and Devika Ganguly
- Department of Research and Development, OPTM Research Institute, Kolkata, India
*Address for Correspondence: Apurba Ganguly, Founder and Chief Scientific Officer, Department of Research and Development, OPTM Research Institute, 145 Rashbehari Avenue, Kolkata - 700029, India, Tel: +919830389616; E-mail: apurbaganguly15@gmail.com
Citation:Ganguly A, Ganguly D. Topical Phytotherapy: Management of Deranged Anatomical and Abnormal Biochemical Risk Factors during Failed Total KneeArthroplasty: A Unique Case Study. J Orthopedics Rheumatol. 2018; 5(1): 6.
Copyright: 2018 Ganguly A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Orthopedics & Rheumatology | ISSN: 2334-2846 | Volume: 5, Issue: 1
Submission: 30 May, 2018 | Accepted: 03 July, 2018 | Published: 12 July, 2018
Keywords
Total knee arthroplasty; Anatomical; Biochemical and imaging markers; Topical phytotherapy; Biochemical risk factors management
Abstract
Total knee arthroplasty (TKA) is the ultimate answer to treat knee osteoarthritis (KOA) worldwide. The main purpose of TKA is to relief pain and to improve the day to day functional activities. But during failed TKA, various abnormal anatomical features and other biochemical risk factors develop in the serum of the patients along with pain and disability of performing daily activities persist.
The present case study was aimed to normalize the deranged anatomical features and elevated levels of biochemical parameters, to relief pain syndromes and to improve daily physical functional abilities without revision of failed TKA correlated with radiological images with the help of topical phytotherapeutic treatment protocol.
Five Indian patients were advice to undergo revision of TKA. They refused to do the further surgery and treated in OPTM Health Care (P) Ltd for 13 weeks. Anatomical measurements included the gap at the knee between the short head of the biceps femoris and the level of the bed, diameter of muscles at the thigh, the calf and, straight leg raising and knee flexions and extensions in different postural positions for both the legs, and biochemical parameters such as serum C-reactive protein (CRP), creatine kinase-muscle (CK-MM) and aldolase A (Aldo A) were measured pre- and post-treatment of 13 weeks using appropriate instruments.
The results indicate the percentage of improvements for all abnormal anatomical and biochemical features were highly statistically significant (p<0.0001), pain under VAS (p<0.0001), pain, stiffness and physical functions under WOMAC Index all are highly significant (p<0.0001) and parameters under KOOS (p<0.0001) and BMI (p<0.0001) with improved radiological images after 13-week of post-treatment. In conclusion, the deranged anatomical and elevated levels of biochemical risk factors, impaired acute pain syndromes, and day to day functional activities including quality of life with abnormal increased body weight developed during failed total knee arthroplasty can be normalized with the help of topical phytotherapeutic treatment protocol within 13 weeks.
Abbreviations
KOA: Knee Osteoarthritis; KGB: Gap at the Knee between the Short Head of the Biceps Femoris Muscle in the Lateral Part of The Knee-Joint and at the Level of the Bed in the Supine Position; DTM: Diameter of the Group of Thigh Muscles; DCM: Diameter of the Group of Calf Muscles; SLR: Straight Leg Rasing; KFS: Knee Flexion in the Supine Position; KFP: Knee Flexion in the Prone Position; KFSt: Knee Flexion in the Standing Position; KES: Knee Extension in the Supine Position; KEP: Knee Extension in the Prone Position; KESt: Knee Extension in the Standing Position; OA: Osteoarthritis; SD: Standard Deviation; AP: Anterior-Posterior; BMI: Body Mass Index; CI: Confidence Interval; MD: Mean Difference
Introduction
Total knee arthroplasty (TKA) is a common treatment method to relief pain and proper knee movement in knee osteoarthritis (KOA) worldwide [1,2]. However, it has been observed that revision of TKA requires in most patients due to infection, obesity, physical activity, loosening, osteolysis etc. [3-6]. The author had already established earlier that abnormal muscle morphology and musculo-postural-features of the legs and abnormal biochemical features and imaging markers are suitable diagnostic protocol for the detection of early progression and risk of KOA [7-10].
Moreover, during failed TKA, various abnormal anatomical features were further increased such as obesity, muscular wasting, unable to rise the legs while lying on bed or walking, unable to fold the knee joints and such other complications. Besides these, other biochemical risk factors develop in the serum of patients such as elevated levels of C-reactive protein (CRP) due to inflammation, creatine kinase-muscle (CK-MM) due to muscle degeneration and aldolase A (Aldo A) due to bone erosion and skeletal muscle damage along with pain and severe disability of performing daily activities also persist.
The present case study was aimed to normalize the deranged anatomical features such as bilateral gap of knees between the point of short head of the biceps femoris at the lateral knee joint and the surface of the bed while supine (KGB), bilateral diameters of the thigh muscles (DTM) and calf muscles (DCM), bilateral straight leg raising (SLR), bilateral angles of flexion in supine, prone and standing positions (KFS, KFP and KFSt respectively) and bilateral angles of extension in supine, prone and standing positions (KES, KEP and KESt respectively), which become asymmetrical between the legs due to damage of various connective muscles and tissues during KOA and normalize the elevated levels of biochemical parameters such as C-reactive protein (CRP) levels increase due to inflammation, creatine kinase-muscle (CK-MM) levels elevated due to muscular dystrophy, connective tissue damage, etc. and Aldolase A (Aldo A) levels increase due to skeletal muscle damages and bone erosion, to relief pain syndromes and to improve daily physical functional abilities without revision of failed TKA correlated with radiological images such as the Kellgren-Lawrence (KL) grading systems with the help of topical phytotherapeutic treatment protocol for 13 weeks.
Case Study
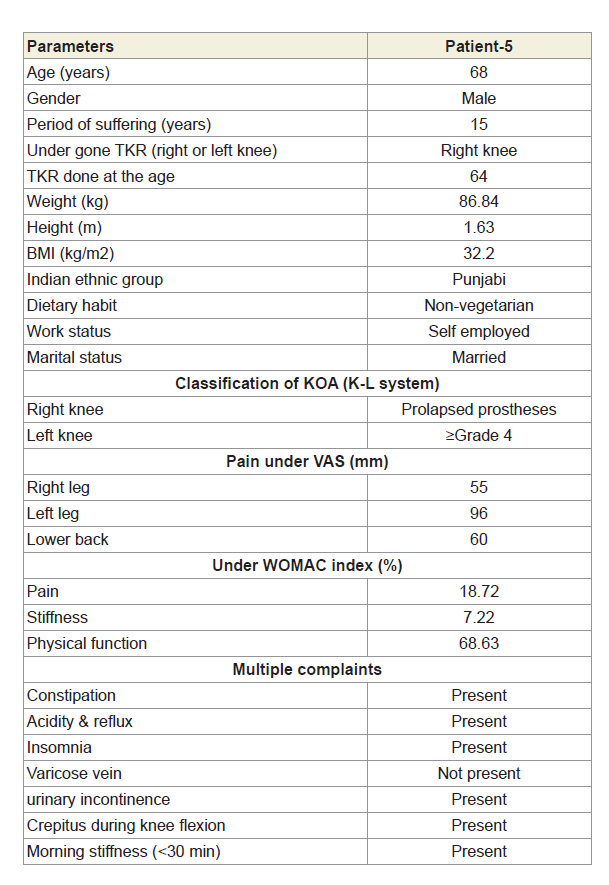
Five patients (4 females and a male) aged between 55-73 years old were suffering with severe pain, inflammation and stiffness on both the knee joints, massive muscular wasting in the thigh and calf regions, unable to raise their legs while supine, prone and standing positions, impaired function, and limitations of daily activities after TKA had undergone 2.5 to 4 years back. Two of them were walking with the help of cane and walker and rest three of them were in wheel chairs. They were advised to further revision of unilateral TKA. But they were refused to undergo further surgery and came to OPTM Health Care (P) Ltd, India, for treatment during the period January 2016 to August 2016. The study protocol was evaluated and approved by the OPTM Research Institute Ethics Committee. An institutional review board-approved consent form for physical examinations, blood sample collections and bilateral knee-joint images (X-rays) required for the study was signed by all five patients. Baseline demographic characteristics of four patients were shown in the previous study by Ganguly A and that of the 5th patient is shown in [Table 1 [11]. The physical examinations were made at the baseline and at the end of 13 weeks of post-treatment including anatomical measurements such as KGB, DTM, DCM, SLR, KFS, KFP, KFSt, KES, KEP and KESt respectively and shown in Table 2.
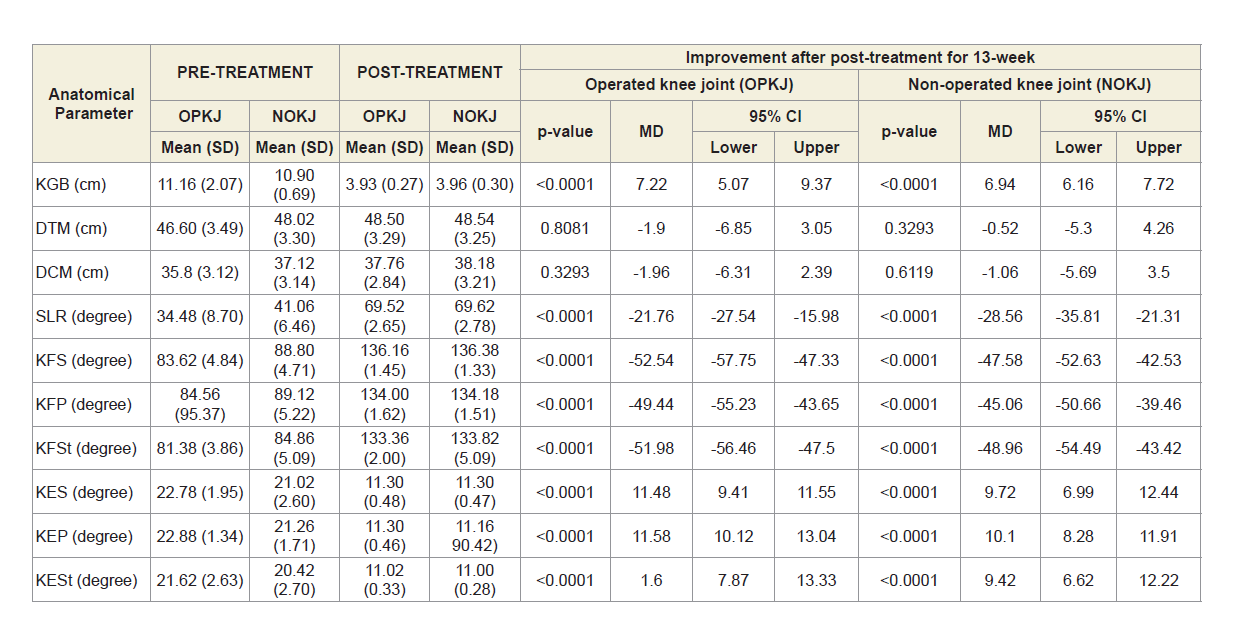
A meter scale was used to measure KGB, DTM and DCM measurements were performed using a meter tape and a goniometer was used for straight leg raising, flexion and extension measurements in accordance with the American Academy of Orthopedic Surgeons (AAOS) [12]. The methods of anatomical measurements had already elaborated in the earlier studies [7-10].
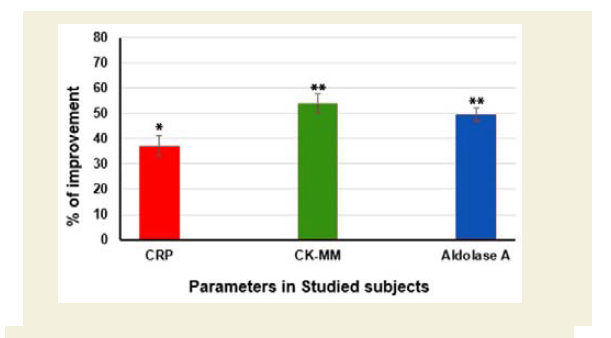
Evaluation of risk factors such as inflammation, muscle degeneration, bone erosion, and skeletal muscle diseases were recorded through the estimation of biomarkers, CRP, CK-MM, and Aldo A levels at the pre-treatment stage and at the end of post-treatment of 13-week using appropriate kits [13-16].
The author had already elaborated in details the treatment protocol based on the aims, principles and theories, accessories and mode of stimuli used in the therapy, effects of chemical, mechanical, thermal and electrical stimuli used in the treatment protocol, the specific programmed postural positions for the regimentation of neuromuscular strength required in the therapy and period of treatment for 13 weeks in the house with necessary documentation in the previous studies [7-11,19].
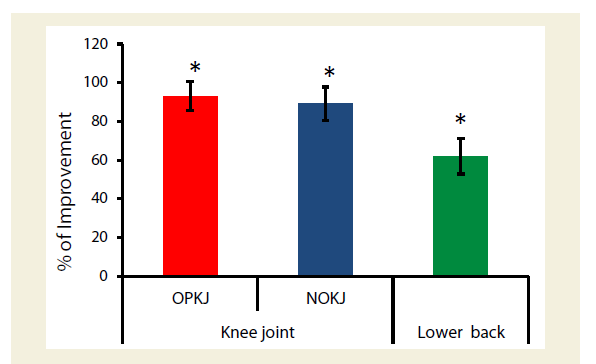
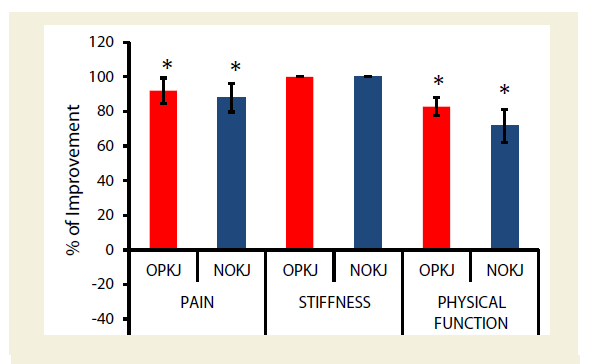
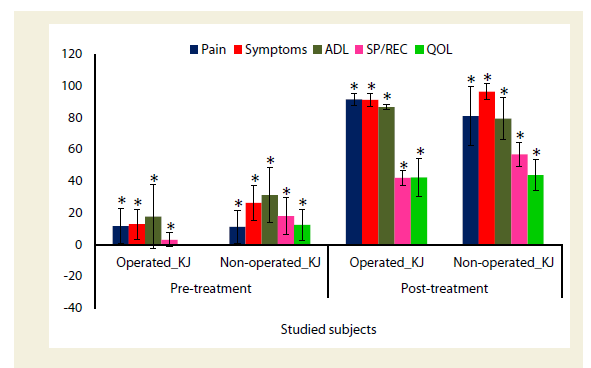
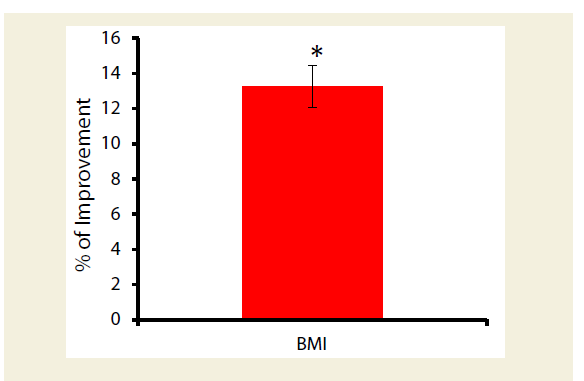
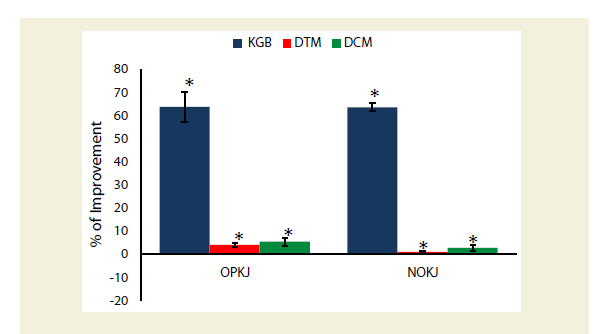
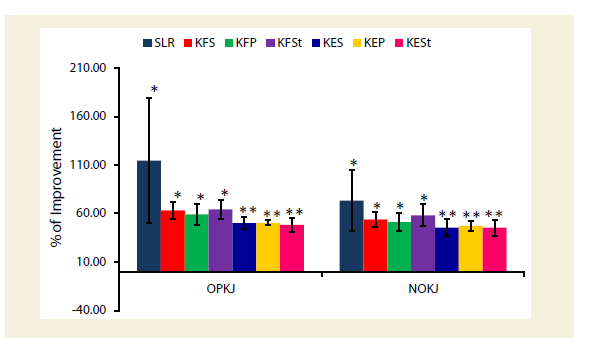
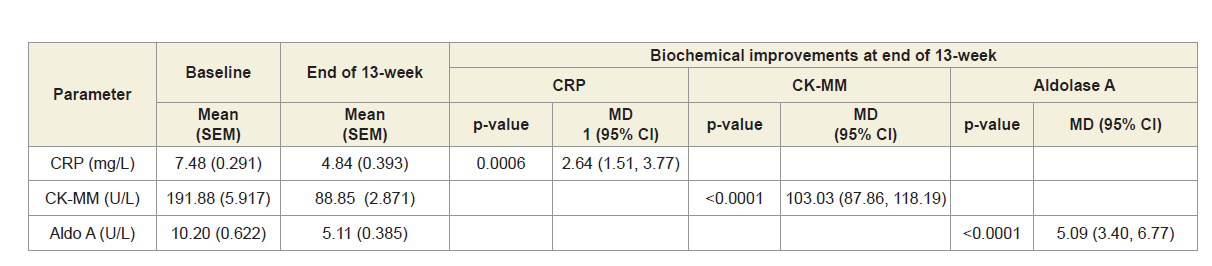
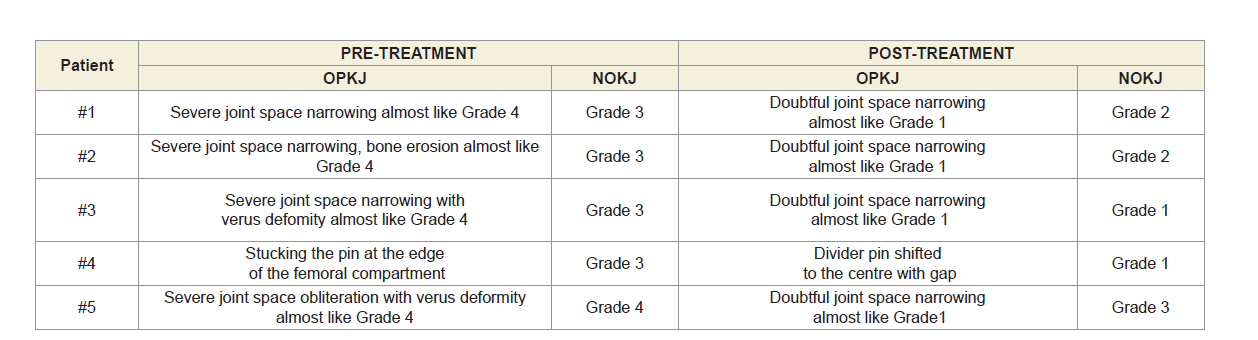
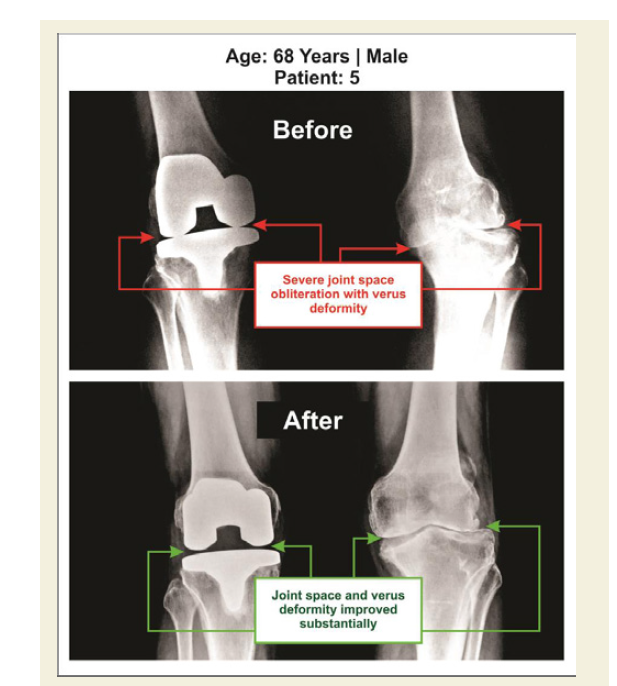
The graphical representations of percentage of improvements on pain, stiffness, physical function and quality of life under VAS, WOMAC Index and KOOS, reduction of body weight as assessed by BMI for five patients are depicted in Figures 1-4. The percentage of improvements at the end of topical phytotherapy treatment of 13 weeks of anatomical features for five patients such as KGB, DTM and DCM is exhibited in Figure 5A, SLR, KFS, KFP, KFSt, KES, KEP and KESt is depicted in Figures 5B. The mean, SD, mean differences (MDs) and 95% confidence intervals of biochemical markers such as CRP, CK-MM and Aldolase A at the pre-treatment stage and at the end of post-treatment and their improvements were shown in Table 3. The overall improvements of pain under visual analogue scale (VAS), pain, stiffness and physical function under WOMAC index and pain, other symptoms, activities of daily living, function on sports and recreation activities and quality of life under KOOS, reduction of body weight as assessed by body mass index (BMI), were also evaluated for five patients at pre-treatment and at the end of post-treatment of 13 weeks of phytotherapy (Figures 1-4). All the five patients were not being treated by oral medications; injections; massage with any type of herbal gels; and any type of alternative treatments such as homeopathic, ayurvedic, herbal or such others for diminishing pain or inflammation, for muscle relaxation, or to improve the skeletal muscles one day prior to post-treatment of 13 weeks. The Kellgren-Lawrance grading system of radiographic KOA of five patients at the pre-treatment stage and at the end of post-treatment were evaluated for bone erosion, reduction of the gap between the femoral and tibial compartments, varus deformities for both operated and non-operated knee joints (Table 4). The radiological images of four of them were shown in the previous study and that of the 5th patient was evaluated at pre- and post-treatment in the present study (Figure 7) [11].
Discussion
Several researchers had already reported the medical effects (specially on pain, inflammation and stiffness of muscles) on human body of the phytochemicals contained in Cissus quadrangularis, Rosemarinus officinals, Calotropis gigantea, Zingiber officinalis, Boswellia serrata, Curcuma longa, Withania somnifera and Sesamum indicum and their mechanism of actions [11,17,18].
It has attempted earlier that the topical application of phytoconstituents from the extracts of seven Indian medicinal plants namely Cissus quadrangularis (whole plant), Calotropis gigantea (root and leaves), Zingiber officinalis (rhizome), Rosmarinus officinalis (leaves and flowers), Boswellia serratia (resin), Curcuma longa (rhizome) and Withania somnifera (root) mixed with virgin sesame oil (extracted from seeds at room temperature) and beehives wax to make viscous phyto-based oil without using any preservatives or chemicals in order to preserve the phytochemical properties of plants intact is extremely useful for the treatment of osteoarthritis [11,17,18]. According to Ganguly A, this is a novel technique and observed first time with the help of aqueous phytoextraction as remedial measures [7]. An established research work when phytochemicals applied topically, phytoconstiuents help in normalization of anatomical derangement in knee-joints supported by radiological images but no one has not been reported before that biochemical markers such as CRP, CK-MM and Aldo A can be in a normal range after the topical application of phytoconstiuents from medicinal plants along with normalization of anatomical derangement, pain, stiffness and functional activities in knee-joints after TKA supported by radiographic changes as assessed by K-L grading scale [7-11,19].
It is interesting to note that the measurements of bilateral KGB, KES, KEP and KESt were widely and asymmetrically increased, and the bilateral DTM, DCM, SLR, KFS, KFP and KFSt were widely and asymmetrically decreased at the baseline because of cumulative effects of muscle wasting, and diminished strength of various connective muscles and tissues during KOA and they were almost symmetrical after the treatment of 13-week (Table 2) [7-10].
The present case report indicates that the normalization of deranged anatomical features and elevated levels of biochemical markers along with improvement of pain, optimization of joint and limb functions and improvement of quality of life with highly statistically significant (p<00001) in all the cases correlated with radiological images as assessed by K-L grading scale are absolutely possible with the help of specialized topical application of phytochemicals within 13 weeks in case of failed TKA (TTables 2-4) (Figures 1-7). Moreover, in the recent studies, the author had already shown no need of revision of TKR and normalization of elevated levels of biomarkers such as CRP, CK-MM and Aldo A developed during osteoarthitic changes in patients with the help of topical phytotherapy treatment [11,19].
Conclusion
The main purpose of TKA is to reduce the pain, increase the functional ability through the improvement of knee flexion [1,2]. This phytotherapeutic treatment may have synergistic effect of the phytochemicals used in the therapy. But, TKA is failed due to infection, obesity, physical activity, loosening, osteolysis, etc.
From the results and discursion, it is firmly concluded that deranged anatomical features and elevated levels of biochemical risk factors, impaired acute pain syndromes, and day to day functional activities including quality of life with abnormal increased body weight as assessed by VAS, WOMAC Index and KOOS and BMI and imaging markers developed during failed total knee arthroplasty can be normalized with the help of topical phytotherapeutic treatment protocol within 13 weeks (Tables 2-4) (Figures 1-7) [11,19].
References
- Hepinstall MS, Ranawat AS, Ranawat CS (2010) High-flexion total knee replacement: functional outcome at one year. HSS J 6: 138-144.
- Lee SM, Seong SC, Lee S, Choi WC, Lee MC (2012) Outcomes of the different types of total knee arthroplasty with the identical femoral geometry. Knee Surg Relat Res 24: 214-220.
- Julin J, Jämsen E, Puolakka T, Konttinen YT, Moilanen T (2010) Younger age increases the risk of early prosthesis failure following primary total knee replacement for osteoarthritis. A follow-up study of 32,019 total knee replacements in the Finnish Arthroplasty Register. Acta Orthop 81: 413-419.
- Kim TK, Chang CB, Kang YG, Kim SJ, Seong SC (2009) Causes and predictors of patient’s dissatisfaction after uncomplicated total knee arthroplasty. J Arthroplasty 24: 263-271.
- Kim KT, Lee S, Ko DO, Seo BS, Jung WS, et al. (2014) Causes of failure after total knee arthroplasty in osteoarthritis patients 55 years of age or younger. Knee Surg Relat Res 26: 13-19.
- Leta TH, Lygre SH, Skredderstuen A, Hallan G, Gjertsen JE, et al. (2016) Outcomes of unicompartmental knee arthroplasty after aseptic revision to total knee arthroplasty: a comparative study of 768 TKAs and 578 UKAs revised to TKAs from the Norwegian Arthroplasty Register (1994 to 2011). J Bone Joint Surg Am 98: 431-440.
- Ganguly A (2014) Tropical phytotherapeutic treatment for achieving knee symmetry in osteoarthritis-a sustainable approach. Int J Phytomed 6: 489-509.
- Ganguly A (2016) Normalization of varus/valgus deformities in osteoarthritis by external application of phytoconstituents: confirmed with anatomical observations and biochemical profiles and radiological images. Ant Physiol Curr Res 6: 224.
- Ganguly A (2018) Diagnosis of knee osteoarthritis risk through abnormal musculo-postural features. Int Arch BioMed Cin Res 4: 39-46.
- Ganguly A (2017) Diagnosis, prevention & phytotherapy for osteoarthritic disorders. Scholars Press Book, USA, pp. 13,14,46-48.
- Ganguly A (2018) Topical phytotherapy is the nobel approach for revision of total knee replacement: a unique case study. J Orthop Rheumatol 5: 1-5.
- American Academy of Orthopaedic Surgeons (1965) Joint motion: method of measuring and recording (4thedn). E & S livingstone Publishers, UK.
- Burtis CA, Ashwood ER, Burns DE (2012) Tietz Textbook of clinical chemistry and molecular diagnosis (5thedn). Elsevier Saunders, USA, pp. 572-557.
- Zeigenhagen G, Drahovshy D, Klinishe Bedeutung des (1983) C-reactive n protein. Med Klin 78: 45-50.
- Cabaniss CD (1990) Creatine kinase (Chapter 32). In: Walker HK, Hall WD, Hurst JW (Eds) Clinical methods: the history, physical, and laboratory examinations (3rdedn). Butterworth Publishers, Boston, USA.
- Feissli S (1966) Quantitative determination of Aldolase. Klin Wschr 44: 390.
- Dragos D, Gilca M, Gaman L, Vlad A, Iosif L, et al. (2017) Phytomedicine in joint disorders. Nutrients 9: 70.
- Belcaro G, Dugall M, Luzzi R, Hosoi M, Ledda A, et al. (2017) Phytoproflex®: supplementary management of osteoarthritis: a pilot, open, supplement registry. Minerva Med 109: 88-94.
- Ganguly A, Ganguly D, Banerjee SK (2018) Topical phytotherapeutic treatment: management of normalization of elevated levels of biochemical parameter during osteoarthritic disorders: a prospective study. J Orthop Rheumatol 5: 1-14.