
Case Report
*Address for Correspondence: Grazyna Sobal, Division of Nuclear Medicine, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Austria, E-mail: grazyna.sobal@meduniwien.ac.at
Citation: Sobal G, Velusamy K, Menzel J, Hacker M. Radiolabeled Chondroitin Sulfate (99mTcCS): Uptake and Binding Studies in Human Articular Chondrocytes and Cartilage in Osteoarthritis.. J Orthopedics Rheumatol. 2015; 2(1): 8.
Copyright © 2015 Sobal G, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Orthopedics & Rheumatology | ISSN: 2334-2846 | Volume: 2, Issue: 1
Submission: 27 May 2015 | Accepted: 25 June 2015 | Published: 30 June 2015
Reviewed & Approved by: Dr. Guangju Zhai, Associate Professor, Department of Genetics, Memorial University of Newfoundland, Canada
Keywords: Cartilage; Chondroitin sulfate; Chondrocytes;Osteoarthritis imaging; Autoradiography
Radiolabeled Chondroitin Sulfate (99mTcCS): Uptake and Binding Studies in Human Articular Chondrocytes and Cartilage in Osteoarthritis
Grazyna Sobal1*, Kavitha Velusamy1, JohannesMenzel2 and Marcus Hacker1
- 1Division of Nuclear Medicine, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Austria
- 22Institute of Immunology, Medical University of Vienna, Austria
*Address for Correspondence: Grazyna Sobal, Division of Nuclear Medicine, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Austria, E-mail: grazyna.sobal@meduniwien.ac.at
Citation: Sobal G, Velusamy K, Menzel J, Hacker M. Radiolabeled Chondroitin Sulfate (99mTcCS): Uptake and Binding Studies in Human Articular Chondrocytes and Cartilage in Osteoarthritis.. J Orthopedics Rheumatol. 2015; 2(1): 8.
Copyright © 2015 Sobal G, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Orthopedics & Rheumatology | ISSN: 2334-2846 | Volume: 2, Issue: 1
Submission: 27 May 2015 | Accepted: 25 June 2015 | Published: 30 June 2015
Reviewed & Approved by: Dr. Guangju Zhai, Associate Professor, Department of Genetics, Memorial University of Newfoundland, Canada
Abstract
Background: Chondroitin sulfate (CS), as Condrosulf (IBSA, Lugano, Switzerland) is used for treatment in patient with osteoarthritis (OA). A suitable and specific radiotracer for imaging of OA is not established yet. For this reason we radiolabeled CS and evaluated its action in OA. The aim of this study was to compare chondrocyte binding of 99mTcCS with cartilage uptake in tissues from patients with OA of different stage and severity.Methods: Radiolabeling of CS was performed using 99mTc (150-180 MBq)/stannous chloride method. Uptake of 99mTcCS (185kBq) was studied in human cartilage tissue samples from patients undergoing knee arthroplasty (n=4, 63-82a). Human articular chondrocytes were isolated from these tissue samples for uptake (37 °C) and binding studies (4 °C) using cell suspension (one million cells/tube) as well as monolayer cultures (15,000 cells/well).
Results: Labelling efficiency ranged 82.3-93.3%, specific activity of 99mTcCS was 4.5-4.9 mCi/μMol. We observed prolonged uptake of the tracer in tissue pieces up to 48 h amounting to a maximum of 49.2±2.2% of the total dose in heavily (grade III) versus 29.7±3.1% in mildly degenerated area (grade II). By autoradiography the uptake was also increasing with time in both areas of degeneration reaching saturation between 24-48 h. The maximum uptake was much higher in grade III tissues as compared to grade II tissues and amounted to 55.3±3.2% vs. 30.1±1.5%. The tracer uptake of chondrocytes in suspension culture after 24 h amounted to 16.9±1.3% from heavy degenerate and 10.8±2.1% from mild degenerate cartilage samples. Binding studies performed in monolayer cultures showed that both specific and non-specific binding from heavy and mild degenerate cartilage chondrocytes at 75 nmol/well reached the maximum binding after 2 h at this CS concentration. 62.4 % vs. 48.8% were bound by these cell populations originated from grade III and II OA cartilage.
Conclusions: These findings demonstrate high specificity (chondrotropism) of 99mTcCS for OA cartilage and significant interaction with chondrocytes and extracellular matrix depending on OA stage, supporting the clinical application of 99mTcCS as a promising diagnostic tool in OA imaging.
Keywords: Cartilage; Chondroitin sulfate; Chondrocytes;Osteoarthritis imaging; Autoradiography
Introduction
Our understanding of OA and our ability to establish early diagnosis of cartilage lesions is limited. Currently, there are neither specifically evaluated in vivo radiotracers for imaging of cartilage damage in OA nor treatments available for markedly altering its progression.Cartilage tissue consists of chondrocytes anchoring in an extracellular matrix which is mainly constituted of proteoglycans (PGs) [1] and type II collagen. The loss of PGs, mainly aggrecan, from the cartilage matrix is one of the hallmarks of OA pathogenesis. In response to this matrix breakdown accelerated by mechanical stress [2], chondrocytes progressively proliferate and produce increasing amounts of PG molecules. The repair process thus initiated is, however, ineffective, since hypertrophic differentiation of chondrocytes in OA [3], besides enhancing synthetic activities of chondrocytes, engenders an altered pattern of proteases favouring degenerative changes. Signalling factors involved in chondrocyte proliferation and differentiation during endochondral ossification might play a similar role in OA cartilage degeneration [4], e.g. in the increased production of aggrecanases or matrix metalloproteinase’s, such as MMP 1 and 3. Catabolic proteases such as cathepsin D are liberated from chondrocytes [5]. In the long run, biomechanical changes are indicative of PG degradation in OA.
Clinical treatment of articular cartilage degeneration includes the use of slow-acting drugs for the treatment of OA (SYSADOA, symptomatic slow acting drugs for OA); these drugs have a slow onset of action and improve OA symptoms after a couple of months or years [6]. Some are administered orally while others are given intra-articularly. Among them, (CS) is a glycosaminoglycan which is naturally found in the extracellular matrix of articular cartilage. It is a carbohydrate heteropolymer strongly negatively charged due to sulfate groups and carboxyl groups distributed along its carbohydrate chains. CS-PGs are highly hydrated and mainly responsible for the viscoelastic properties of cartilage [7]. It is important to note, that CS applied for pharmaceutical use must be under strict evaluation for quality and purity [8,9], as is the case for Condrosulf used as substrate for tracer labelling in the present publication. In contrast, so called nutraceutical preparations of CS are not subject to such rigorous restrictions. Pharmaceutical grade CS (e.g. Condrosulf) has also been shown to display structure-modifying effects, characterizing the S/ DMOAD (structure/disease modifying anti-OA drugs [10], class of anti-OA drugs [11]. Recent studies indicate that apart from important structural functions such as viscoelasticity and gel formation potential CS and CS-containing PGs display diverse biological activities, such as influencing cellular differentiation and migration, immunity, wound repair, inflammation and growth factor activity [12-15].
The aim of this study was to radiolabel CS with 99mTc and evaluate its action in osteoarthritis. It was important to verify whether the uptake of 99mTcCS correlates both in regional chondrocytes and cartilage tissue with the degree of cartilage degeneration. This finding could be crucial for diagnosis of osteoarthritis.
Materials and Methods
Patients4 patients with OA (3 females, 63 a, 73 a, 82 a and 1 male, 68 a) undergoing knee arthroplasty with different disease activity were studied. The use of samples from these patients was approved by the local ethic commission (EK-Nr. 523/2008). Of each patient, cartilage samples were analysed for mild and heavy degeneration areas according to histological examination and uptake of 99mTcCS was evaluated to prove tracer specificity.
Radiolabeling
We performed the radiolabeling using Condrosulf, a CS preparation of average molecular weight 24 kDa (IBSA, witzerland, and SANOVA Pharma, Vienna, Austria). The radiolabeling was performed using the 99mTcO4 −/stannous chloride method [16]. Briefly, 25 mg of CS (Condrosulf) were dissolved in 0.5 ml 0.3 NHCl followed by addition of 1mg of stannous chloride dissolved in 0.1 ml 0.3 NHCl, 150 MBq 99mTcO4 −/(0.25 ml) and 0.25 ml 0.5 M Na acetate, pH 5.0. The reaction mixture was gently stirred and incubated for 1 h at room temperature. Then, the radiolabeled product was applied to a PD 10 column (Amersham Pharmacia, Biotech.) for separation from free technetium. 0.50 M Na acetate, pH 5.0 buffer was used to elute radiolabeled CS from the column (3-5 ml). The free technetium was eluted from the column with the total volume (6-10 ml). In parallel the measurement of the optical density (O.D) for each of eluted fractions to estimate CS content was performed [17].
Quality control
ITLCSG chromatography was performed for the quality control of the tracer using 0.2 M saline in 10% ethanol as solvent to detect colloid content. Aluminium oxide IB-F TLC-sheets and ethanol as solvent were used to estimate free pertechnetate [18].
Chondrocyte cell lines
Cartilage tissue from each patient undergoing knee arthroplasty (n=4, 63-82 a) was divided into areas of mild (grade II) and heavy degeneration (grade III) according to histological examination. Chondrocytes were isolated from both tissue areas of cartilage samples (~0.5-1 g wet weight) using enzymatic digestion with 0.2% collagenase for 10 h and cultivated according to the standard procedure using CGM Chondrocyte Growth BulletKit (Lonza, US) [19]. The cells were harvested at passage 3.
Uptake studies in tissue samples
For uptake studies, human cartilage tissue samples (both heavy and mild degenerate) from same patients as used for chondrocyte isolation were cut into pieces of about 5 mg wet weight and used for uptake by incubation with 10 μCi/well of 99mTcCS. Uptake was monitored for 30 min, 1 h, 3 h, 6 h, 24 h, 48 h, 72 and 96 h. After each incubation period, the tissue was separated from incubation medium and washed twice with PBS buffer (150 μl). The radioactivity was separately counted in each tube (the tissue, supernatant and wash) giving in sum the total count of activity. The calculated % uptake (% total activity)=tissue activity/total activity×100%. The uptake of 99mTcCS in vitro was measured by a gamma counter (Packard, Meridien, CT, USA).
Autoradiography
For in vitro autoradiography -20 °C embedded frozen coronal cartilage sections (5 μ) from the same patients as used for chondrocytes isolation and uptake in tissue pieces, cut by microtome (Cryostat MTE, SLEE Technik GmbH, Mainz, Germany) were used. The use of these samples was approved by the institutional ethics committee and the national authority EK-Nr. 523/2008. These frozen sections were equilibrated first to room temperature for 1h. Then the slices were introduced in a drop-wise manner to cover the surface of each section (50 μl) for incubation with 10 μCi of 99mTcCS. The incubation was performed for 30 minutes, 1, 3, 6, 24, 48 and 72 h, thereafter the radioligand was aspirated and sections were rinsed 3 times with 5 ml PBS buffer to remove the excess of radioligand. After drying the uptake was evaluated using an Autoradiograph (Instant Imager, Packard, Meriden, CT, USA).
Uptake and binding of 99mTcCS to chondrocytes
Uptake studies were performed at 37 °C in chondrocytes of both mild and heavy degeneration in suspension cultures, one million cells/tube. Uptake was monitored for 30 min, 1 h, 3 h, 6 h, 24 h, 48 h, 72 h until saturation was achieved. In parallel, for binding studies adherent monolayer cultures of human chondrocytes (15,000 cells/ well) were incubated in 96-well plates together with increasing amounts of 99mTcCS (10-150 nmol/well). Incubation was performed at 4 °C for 2 h in the presence or absence of a 50-fold excess of unlabeled CS to estimate non-specific uptake. Cells were gently shaken during incubation. The medium was then aspirated and the cell layer washed twice with medium. The cells were lysed in 0.25 ml of a solution containing 0.1% sodium deoxycholate and 0.05 N sodium hydroxyde and counted in a gamma-counter.
Statistical analysis;
The results are expressed as mean values (SD). Statistical analysis was performed to compare the mean of the outcomes between heavy and mild degeneration samples from 4 patients (grade III versus grade II samples) at each time point (plots 3, 6, 7) using one-way ANOVA. P


Autoradiography


Binding and uptake of 99mTcCS by chondrocytes
Results
Specific activity of labelled CSLabeling efficiency ranged 82.3-93.3%. Specific activity achieved was 4.5-4.9 mCi/μMol.
Quality control
The tracer was stable in buffer over a 6 h period after labeling up to 95%, (n=4) of the radiochemical purity. The stability of the tracer using our method resulted in a very low colloid content up to 5% only.
Uptake of 99mTcCS in tissue pieces
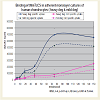
By the use of human articular cartilage tissue pieces (from both areas with heavy and mild degeneration from the same patient as shown in Figure 1 and histological examination in Figure 2) we found a correlation between the tracer uptake and degree of degeneration (Figure 3). We observed prolonged uptake of the tracer up to 96 h amounting to a maximum of 49.2±2.2% in heavy degenerated area (grade III) versus 29.7±3.1% in mild degenerate area (grade II). This fact indicates permanent incorporation of the tracer into the human cartilage and proved the chondrotropic effects. At the incubation time of 48 h saturation was already achieved.
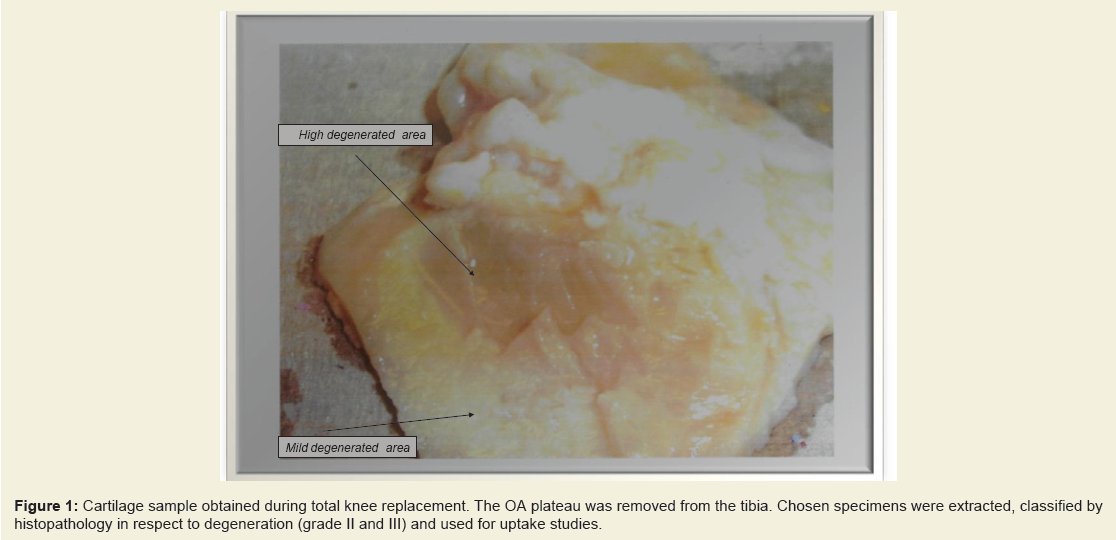
Figure 1: Cartilage sample obtained during total knee replacement. The OA plateau was removed from the tibia. Chosen specimens were extracted, classified by histopathology in respect to degeneration (grade II and III) and used for uptake studies.
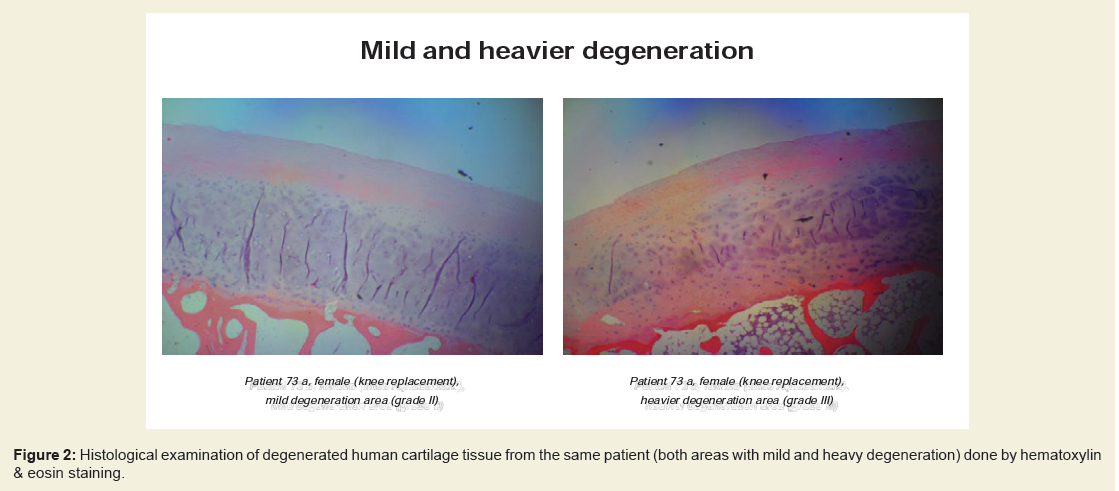
Figure 2: Histological examination of degenerated human cartilage tissue from the same patient (both areas with mild and heavy degeneration) done by hematoxylin& eosin staining.
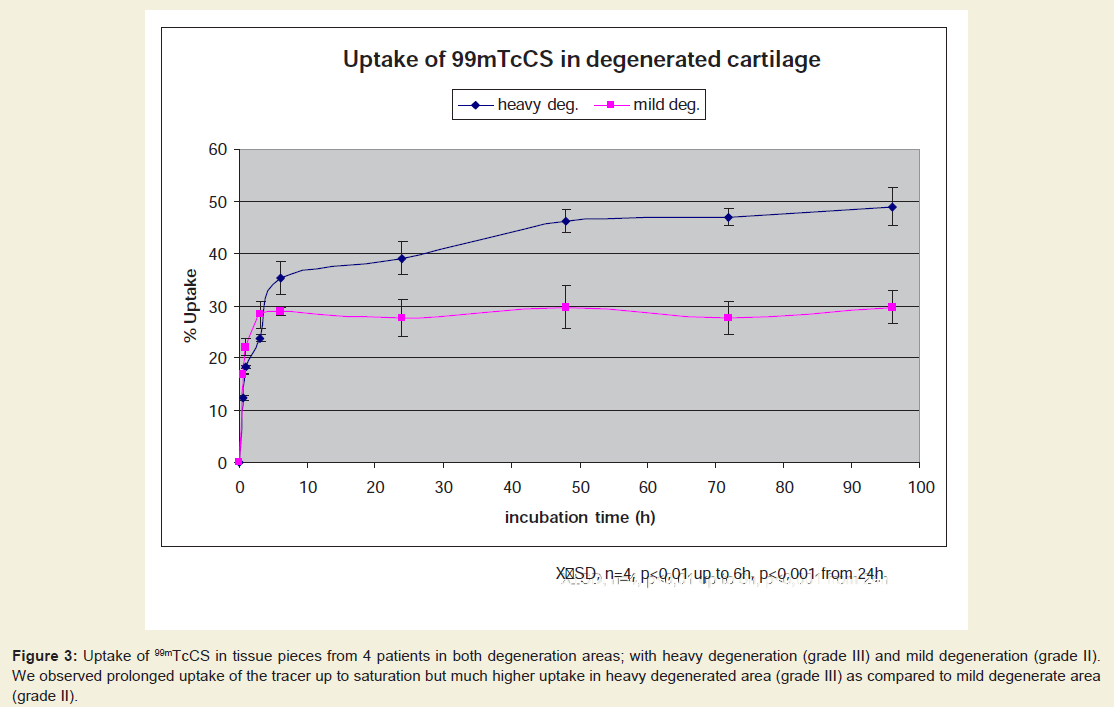
Figure 3: Uptake of 99mTcCS in tissue pieces from 4 patients in both degeneration areas; with heavy degeneration (grade III) and mild degeneration (grade II). We observed prolonged uptake of the tracer up to saturation but much higher uptake in heavy degenerated area (grade III) as compared to mild degenerate area (grade II).
Autoradiography of 99mTcCS in frozen tissue sections was performed from same patients as used for chondrocyte isolation and uptake in tissue pieces in both areas with heavy and mild degeneration from same patients according to histological evaluation. We obtained similar results regarding the correlation between 99mTcCS uptake intensity and degree of cartilage degeneration (grade III vs. grade II) as shown in Figure 4 and Figure 5. The uptake was also increasing with time in both areas of degeneration reaching saturation at 24 h. The maximal uptake by autoradiography was markedly higher by grade III (Figure 4) as compared to grade II (Figure 5) and amounted to 55.3±3.2% vs. 30.1±2.5% .
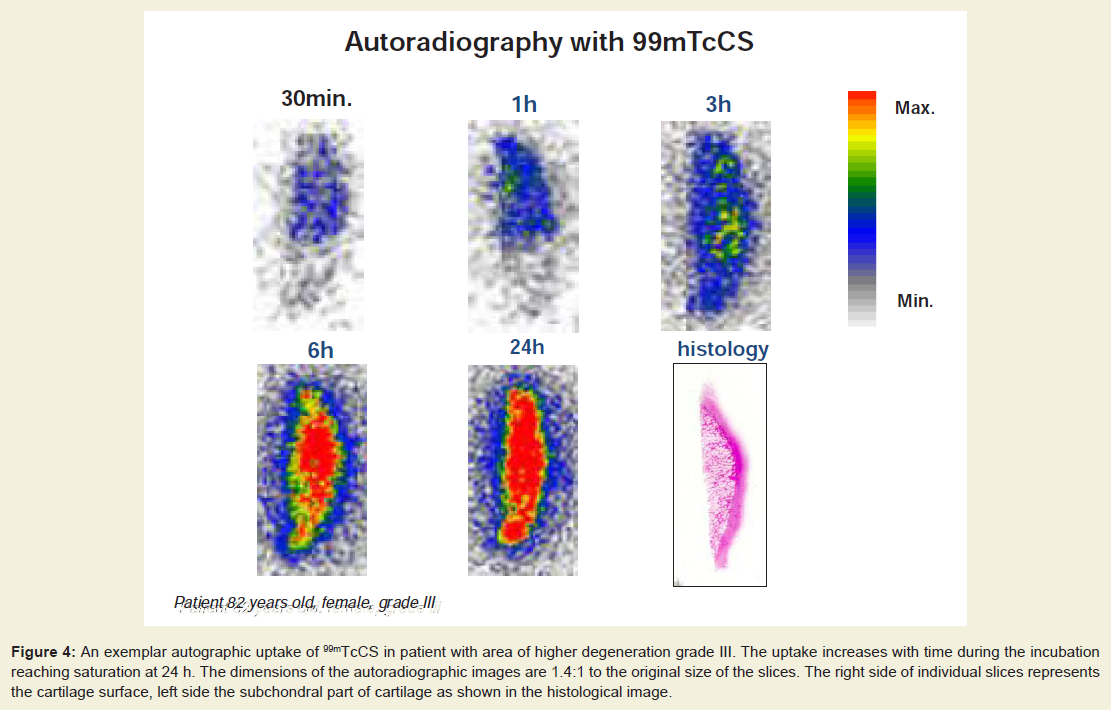
Figure 4: An exemplar autographic uptake of 99mTcCS in patient with area of higher degeneration grade III. The uptake increases with time during the incubation reaching saturation at 24 h. The dimensions of the autoradiographic images are 1.4:1 to the original size of the slices. The right side of individual slices represents the cartilage surface, left side the subchondral part of cartilage as shown in the histological image.
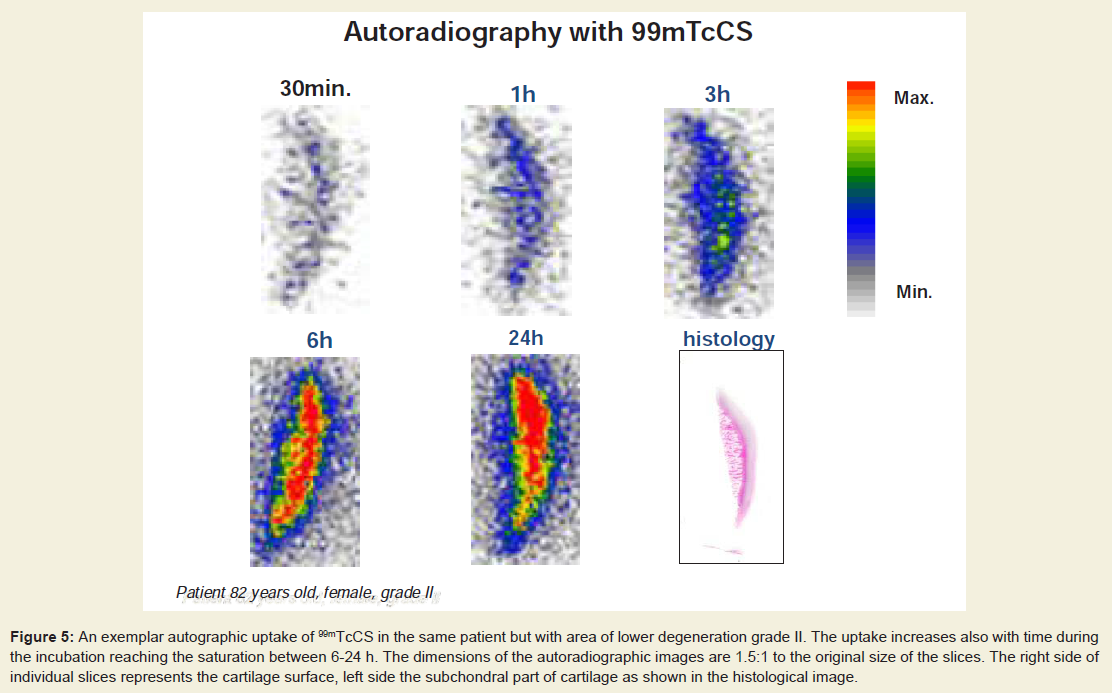
Figure 5: An exemplar autographic uptake of 99mTcCS in the same patient but with area of lower degeneration grade II. The uptake increases also with time during the incubation reaching the saturation between 6-24 h. The dimensions of the autoradiographic images are 1.5:1 to the original size of the slices. The right side of individual slices represents the cartilage surface, left side the subchondral part of cartilage as shown in the histological image.
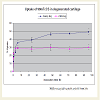
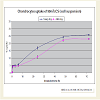
In suspension cultures (Figure 6) we found higher uptake in chondrocytes isolated from higher degenerated areas (grade III vs. grade II from same patient). The tracer uptake at 24 h amounted to 17.2±1.3% in chondrocytes from heavily degenerate and to 10.8±2.1% in chondrocytes from mildly degenerated cartilage (Figure 6) followed by saturation between 48 and 72 h. Concentration of 99mTcCS in suspension cultures was 2 nmol/ml. The binding studies in monolayer cultures at much higher supraphysiological CS concentrations (up to 150 nmol per well) showed, however, that both specific and nonspecific binding of heavily and mildly degenerated chondrocytes reached the maximum binding at 75 nmol/well already after 2 h even at 4 °C. Heavy degenerate binding for specific and non-specific at maximum by 75 nmol/well was 695,153±959 and 81,637±403 cpm respectively (Figure 7). Mild degenerate binding for specific and non-specific at maximum by 75 nmol/well was 530,892±136 and 51,246±772 cpm respectively (Figure 7). This corresponds to 46.8 vs. 36.6 nM specifically bound 99mTcCS per well, i.e., 62.4 vs. 48.8% of total added radioactivity. Non-specific binding was generally less than 15% of total binding.
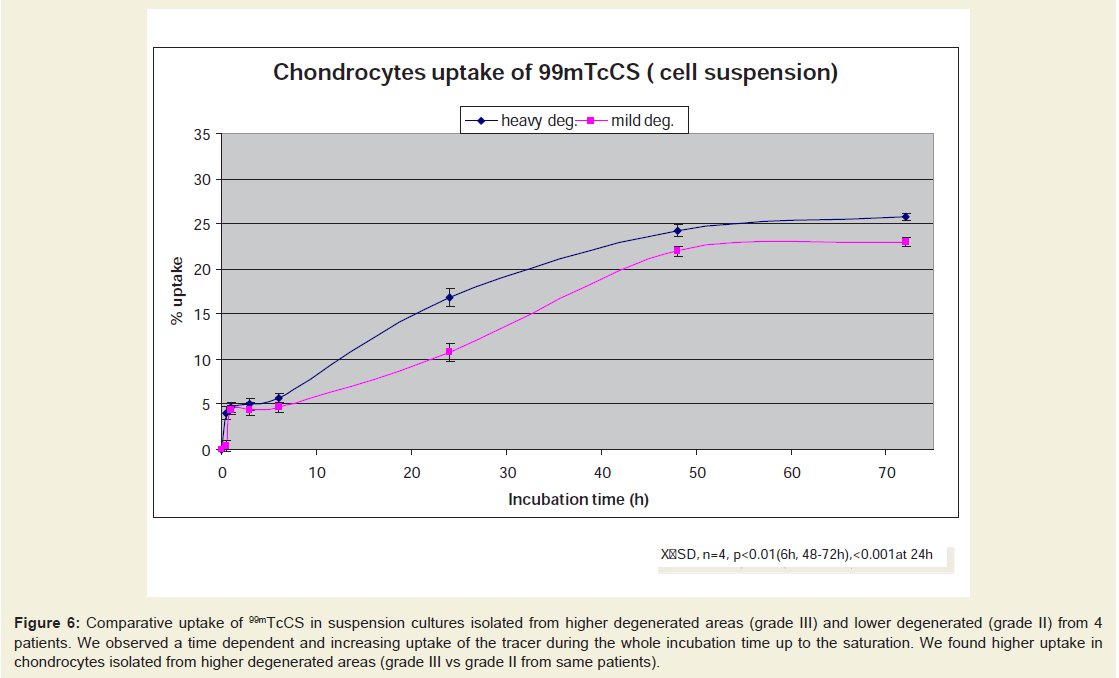
Figure 6: Comparative uptake of 99mTcCS in suspension cultures isolated from higher degenerated areas (grade III) and lower degenerated (grade II) from 4 patients. We observed a time dependent and increasing uptake of the tracer during the whole incubation time up to the saturation. We found higher uptake in chondrocytes isolated from higher degenerated areas (grade III vs grade II from same patients).
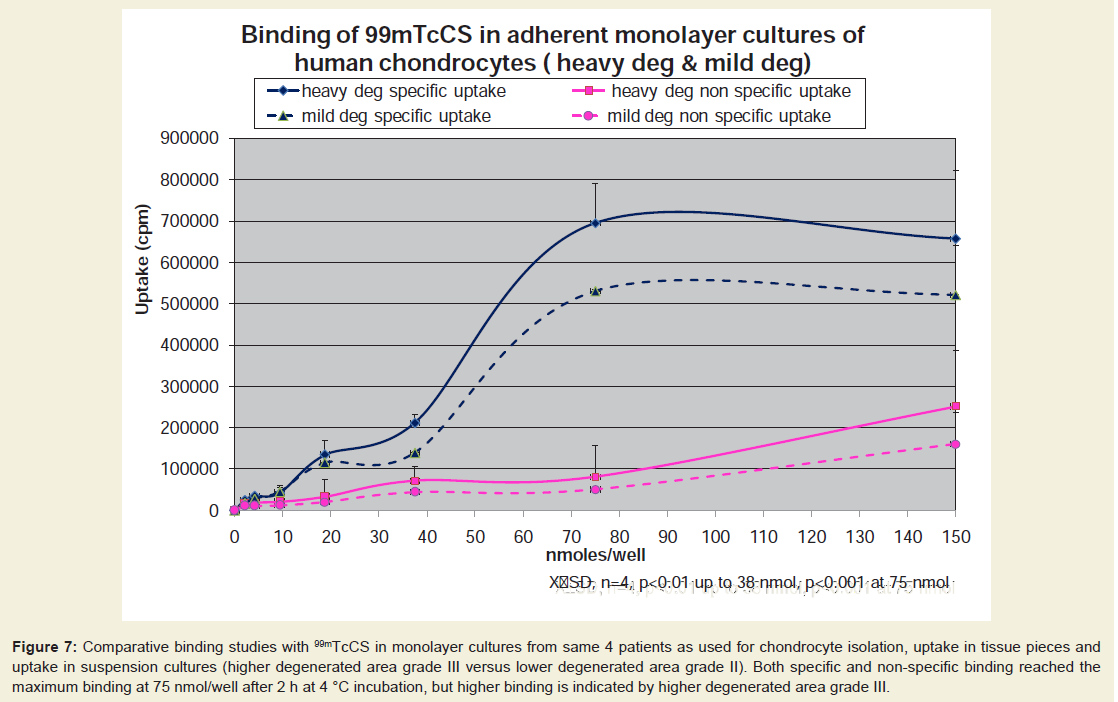
Figure 7: Comparative binding studies with 99mTcCS in monolayer cultures from same 4 patients as used for chondrocyte isolation, uptake in tissue pieces and uptake in suspension cultures (higher degenerated area grade III versus lower degenerated area grade II). Both specific and non-specific binding reached the maximum binding at 75 nmol/well after 2 h at 4 °C incubation, but higher binding is indicated by higher degenerated area grade III.
Discussion
The slow-acting symptomatic drugs (SADOAs) are agents that can alleviate OA symptoms with a longer term and in a safer way but with a delayed onset of action. Among them, a lot of natural and synthetic compounds of various origins have been introduced on the market, but only a few have been proven to be effective in reducing OA symptoms, i.e., pentosan polysulfate, high-molecularweighthyaluronan, diacerhein, doxycycline, glucosamine [20] and chondroitin sulfate, as well as mixtures of these two last compounds [6,21]. CS, a glycosaminoglycan chain made up of the repeating disaccharide D-glucuronic acid- N-acetylgalactosamine sulfated at the 4 or 6 position is a major constituent of cartilaginous tissues, representing the carbohydrate chains of aggrecan, a PG which is mainly responsible for cartilage hydration [22].One rationale for using this type of compound therapeutically is based upon the fact that OA cartilage becomes progressively depleted of glycosaminoglycans and that chondrocytes in OA cartilage respond to such a stress by increased synthesis of new PG, i.e., in a compensatory manner [2]. In this scenario of repair mechanisms CS seems to play a pivotal role [23]. Thus, a recent publication indicates that CS has important regulatory functions as a signalling factor in human chondrocytes [24]. Thus, in CS-treated chondrocytes, exogenous CS indirectly lowered matrix degradation by inhibiting matrix metalloproteinase activation (MMP 1 and MMP 3). In general, evidence of anti-angiogenic, anti-inflammatory and anticatabolic activities of CS have been described [24,25].
In this paper we have been comparing the incorporation of 99mTcCS into cartilage tissue and chondrocytes. The diffusion of ions such as negatively charged CS into cartilage is a passive process, which does not depend on living chondrocytes [26]. The rate of diffusion is important in this context as long as it is dissimilar in the mildly and heavily degenerate cartilage. Preliminary experiments had shown that a 48 h period gave the best difference in counts per minute between normal and diseased cartilage. Uptake of 99mTcCS by heavy degenerate tissues was indeed higher than by mild degenerate tissues, this is underlined by autoradiographic studies.
We also noted significant differences in the response to exogenous CS of chondrocytes originating from heavy degenerate and mild degenerate cartilage. A significantly higher interaction was observed for chondrocytes isolated from heavily degraded cartilage both in suspension culture and monolayer culture. For suspension cultures we used low CS concentrations (2 μM), as our biodistribution studies had shown, that only a small percentage of the injected tracer (0.2%) reaches the knee joint space and then diffuses into cartilage. For monolayer cultures, however, we used significantly higher CS concentrations to achieve saturation.
What is the importance of chondrocytes for overall CS uptake by cartilage? Among the cartilage constituents chondrocytes play only a minor role as far as their content is concerned (1-2% of total cartilage mass). However, since these cells, the only cells found in articular cartilage, are involved in the biosynthesis of ECM components such as collagen II and PG, whose main carbohydrate component is CS, it is worthwhile to study their role in CS uptake and binding. We therefore tested whether increased tissue repair correlates with uptake and binding of 99mTcCS by chondrocytes isolated from OA joints. Indeed, we found that uptake of labelled CS by chondrocytes from differently degraded cartilage mimics the response of cartilage tissue itself as demonstrated by tissue uptake and autoradiographic studies. Both in suspension culture and in monolayer culture, chondrocytes obtained from heavily degenerate OA cartilage showed a significantly higher uptake of 99mTcCS than chondrocytes from mildly degraded cartilage areas. Potential cellular binding and uptake mechanisms are already broadly discussed in our paper [18]. We now proved that cellular binding depends on the degree of tissue degeneration in OA cartilage.
OA in the ageing Western population is a major health problem. The limited treatment available for this disease (analgesics, nonsteroidal anti-inflammatory drugs) emphasizes the urgent need to elucidate the molecular mechanisms of disease progression. Disease-modifying osteoarthritis drugs (DMOADs) [10] which can interfere with joint remodelling and destruction, offer new promising therapeutic strategies. However, objective evaluation of treatment efficacy is hampered by the lack of diagnostic tools for assessing early stages of the disease, especially when its progression is to be controlled [27]. Furthermore, currently no imaging technique is sensitive enough to ensure objective evaluation of these new therapeutic strategies, targeting the intracellular signalling pathways responsible for OA progression.
Therefore, we investigated the in vitro uptake of 99mTcCS in human articular cartilage. Imaging with a labeled chondrotropic tracer of cartilage such as CS could be useful for the detection of OA, longitudinal follow-up of treated patients and evaluation of new therapies. Such a tool could provide a suitable set of criteria for assessing cartilage functions especially in OA and for testing the efficacy of new drugs such as DMOADs [10].
Conclusion
The findings of this study indicate that the uptake of 99mTcCS depends on the grade of degeneration in articular cartilage. In particular, significant variation was observed between heavily and mildly degenerated cartilage, which had altered uptake properties. Tissue uptake is mirrored by chondrocyte uptake. Our data demonstrate efficacy of 99mTcCS as an imaging tracer in OA and also show that 99mTcCS accumulates in the cartilage tissue, either by acting as possible substrate for further PG synthesis via chondrocytes and/ or by mere trapping in cartilage. We found out that the uptake of 99mTcCS correlates both in regional chondrocytes and cartilage tissue with the degree of cartilage degeneration. This finding could be crucial to detect OA at a stage in which therapy with DMOADs is still efficient.References
- Hardingham TE, Fosang AJ (1992) Proteoglycans: many forms, many functions. FASEB J 6: 861-870.
- Lipiello L (2003) Glucosamine and chondroitin sulfate: biological response modifiers of chondrocytes under simulated conditions of joint stress. Osteoarthritis Cartilage 11: 335-342.
- van der Kraan PM, van den Berg WB (2012) Chondrocyte hypertrophy and osteoarthritis: role in initiation and progression of cartilage degeneration? Osteoarthritis Cartilage 20: 223-232.<
- Dreier R (2010) Hypertrophic differentiation of chondrocytes in osteoarthritis: the developmental aspect of degenerative joint disorders. Arthritis Res Ther 12: 216.
- Troeberg L, Nagase H (2012) Proteases involved in cartilage matrix degradation in osteoarthritis. Biochim Biophys Acta 1824: 133-145.
- Bruyere O, Burlet N, Delmas PD, Rizzoli R, Cooper C, et al. (2008) Evaluation of symptomatic slow-acting drugs in osteoarthritis using the GRADE system. BMC Musculoskelet Disord 9: 165.
- Hardingham T (2008) Extracellular matrix and pathogenic mechanisms in osteoarthritis. Curr Rheumatol Rep 10: 30-36.
- Volpi N (2007) Analytical aspects of pharmaceutical grade chondroitin sulfates. J Pharm Sci 96: 3168-3180.
- Volpi N (2009) Quality of different chondroitin sulfate preparations in relation to their therapeutic activity. J Pharm Pharmacol 61: 1271-1280.
- Qvist P, Bay-Jensen AC, Christiansen C, Dam EB, Pastoureau P, et al. (2008) The disease modifying osteoarthritis drug (DMOAD): Is it in the horizon? Pharmacol Res 58: 1-7.
- Kahan A, Uebelhart D, De Vataire F, Delmas PD, Reginster JY (2009) Long-term effects of chondroitin 4 and 6 sulfate on knee osteoarthritis : the study on osteoarthritis progression prevention, a two-year, randomized, double-blind, placebo-controlled trial. Arthritis Rheum 60: 524-533.
- Sughara K, Mikami T, Uyyama T, Mizuguchi S, Nomura K, et al. (2003) Recent advances in the structural biology of chondroitin sulfate and dermatan sulfate. Curr Opin Struct Biol 13: 612-620.
- Mikami T, Kitagawa H (2013) Biosynthesis and function of chondroitin sulfate. Biochim Biophys Acta 1830: 4719-4733.
- Volpi N (2011) Anti-inflammatory activity of chondroitin sulphate: new functions from an old natural macromolecule. Inflammopharmacology 19: 299-306.
- Haylock-Jacobs S, Keough MB, Lau L, Yong VW (2011) Chondroitin sulphate proteoglycans: extracellular matrix proteins that regulate immunity of the central nervous system. Autoimmun Rev 10: 766-772.
- Sobal G, Menzel EJ, Sinzinger H (2008) Radiolabeling procedure, quality control and stability of 99mTc-labeled chondroitin sulfate. a new approach of targeting osteoarthritis. Appl Radiat Isot 66: 415-420.
- Sobal G, Sinzinger H (2002) Binding of [99mTc]chondroitin sulfate to scavenger receptors on human chondrocytes as compared to binding of oxidized [125I]LDL on human macrophages. J Recept Signal Transduct Res 22: 459-470.
- Sobal G, Menzel EJ, Sinzinger H (2009) Uptake of 99mTc-labeled chondroitin sulfate by chondrocytes and cartilage: a promising agent for imaging of cartilage degeneration? Nucl Med Biol 36: 65-71.
- Oseni AO, Butler PE, Seifalian AM (2013) Optimization of chondrocyte isolation and characterization for large-scale cartilage tissue engineering. J Surg Res 181: 41-48.
- Wollheim FA (2007) Prescription of glucosamine for osteoarthritis: does it work and is it safe? Nat Clin Pract Rheumatol 3: 364-365.
- Moskowitz RW (1991) Chondroprotective agents. Do they already exist? Eur J Rheum Inflamm 11: 21-25.
- Dudhia J (2005) Aggrecan, aging and assembly in articular cartilage. Cell Mol Life Sci 62: 2241-2256.
- Martel-Pelletier J, Kwan Tal S, Pelletier JP (2010) Effects of chondroitin sulfate in the pathophysiology of the osteoarthritic joint: a narrative review. Osteoarthritis Cartilage 18 Suppl 1: S7-S11.
- Calamia V, Lourido L, Fernandez-Puente P, Mateos J, Rocha B, et al. (2012) Secretome analysis of chondroitin sulfate-treated chondrocytes reveals anti-angiogenic, anti-inflammatory and anti-catabolic properties. Arthritis Res Ther 14: R202.
- Chan PS, Caron JP, Rosa GJ, Orth MW (2005) Glucosamine and chondroitin sulfate regulate gene expression and synthesis of nitric oxide and prostaglandin E(2) in articular cartilage explants. Osteoarthritis Cartilage 13: 387-394.
- Maroudas A, Evans H (1974) Sulphate diffusion and incorporation into human articular cartilage. Biochim Biophys Acta 338: 265-279.
- Miot-Noirault E, Vidal A, Pastoureau P, Bonafus J, Chomel A, et al. (2007) Early detection and monitoring of cartilage alterations in the experimental meniscectomised guinea pig model of osteoarthritis by 99mTc-NTP 15-5 scintigraphy. Eur J Nucl Med Mol Imaging 34: 1280-1290.