
Case Report
*Address for Correspondence: Dr. Franz Fogt, MD, med. M.B.A., Department of Pathology, Department of Ophthalmic Pathology (Scheie Eye Institute), WS 551, University of Pennsylvania, 39th and Market Streets, Philadelphia PA 19104, E-mail: fogt@mail.med.upenn.edu
Citation: Fogt F, Wellmann A, Lee V. Immunoglobulin G4-Related Disease (IgG4-RD) with Associated Sarcoidosis. J Ocular Biol. 2013;1(1): 3.Copyright © 2013 Fogt F, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Ocular Biology | ISSN: 2334-2838 | Volume: 1, Issue: 1
Submission: 25 June 2013 | Accepted: 15 August 2013 | Published: 19 August 2013
 An orbital biopsy of the right side was performed and showed lacrimal gland tissue with fibrosis and chronic inflammation, including predominantly non-caseating granulomas (Figure 2). At the time of his initial ophthalmology visit, the patient was not on any systemic treatment for sarcoidosis, though he had been treated with oral prednisone in the past. A computed tomography scan of the orbits was performed, which demonstrated massive bilateral lacrimal gland masses extending to the orbital apex with involvement of the superior oblique and superior and lateral recti with reactive orbital bone formation (Figure 3). Because of worsening symptoms and radiologic findings, he underwent orbital decompression and resection of the masses from both orbits in succession.
An orbital biopsy of the right side was performed and showed lacrimal gland tissue with fibrosis and chronic inflammation, including predominantly non-caseating granulomas (Figure 2). At the time of his initial ophthalmology visit, the patient was not on any systemic treatment for sarcoidosis, though he had been treated with oral prednisone in the past. A computed tomography scan of the orbits was performed, which demonstrated massive bilateral lacrimal gland masses extending to the orbital apex with involvement of the superior oblique and superior and lateral recti with reactive orbital bone formation (Figure 3). Because of worsening symptoms and radiologic findings, he underwent orbital decompression and resection of the masses from both orbits in succession.
 Histological examination of the orbital masses showed focal dense fibrous tissue with mild to moderate chronic inflammation with foci of prominent lymphoplasmacytic inflammation; poorly formed granulomas; and lacrimal gland tissue with atrophy and chronic lymphoplasmacytic infiltrate (Figure 4A-4C). Plasma cells throughout the specimen were densely positive for IgG and IgG4 immunohistochemical staining with a IgG4 ratio of 46% (Figure 4E). In addition, the vasculature within the involved tissue showed the presence of obliterative phlebitis (Figure 4F and 4G). The biopsies from the initial bronchial and orbital biopsies were subsequently reviewed.
Histological examination of the orbital masses showed focal dense fibrous tissue with mild to moderate chronic inflammation with foci of prominent lymphoplasmacytic inflammation; poorly formed granulomas; and lacrimal gland tissue with atrophy and chronic lymphoplasmacytic infiltrate (Figure 4A-4C). Plasma cells throughout the specimen were densely positive for IgG and IgG4 immunohistochemical staining with a IgG4 ratio of 46% (Figure 4E). In addition, the vasculature within the involved tissue showed the presence of obliterative phlebitis (Figure 4F and 4G). The biopsies from the initial bronchial and orbital biopsies were subsequently reviewed. Immunohistochemical stain for IgG4 was performed on both prior specimens, which showed only focal IgG4 positive inflammatory cells in the orbital tissue (Figure 2), and dense non-necrotizing granulomas and absence of IgG4 positive cells in the bronchial biopsy (biopsy 1). Therefore, a diagnosis of IgG4 related dacryoadenitis was made. The patient recovered well from surgery with nearly complete recovery of his visual function.
Immunohistochemical stain for IgG4 was performed on both prior specimens, which showed only focal IgG4 positive inflammatory cells in the orbital tissue (Figure 2), and dense non-necrotizing granulomas and absence of IgG4 positive cells in the bronchial biopsy (biopsy 1). Therefore, a diagnosis of IgG4 related dacryoadenitis was made. The patient recovered well from surgery with nearly complete recovery of his visual function.
Immunoglobulin G4-Related Disease (IgG4-RD) with Associated Sarcoidosis
Franz Fogt1,2*, Axel Wellmann3 and Vivian Lee2
- 1Department of Pathology, Penn Presbyterian Medical Center, University of Pennsylvania, PA, USA
- 2Department of Ophthalmic Pathology, Scheie Eye Institute, University of Pennsylvania, PA, USA
- 3Institute of Pathology, Celle, Germany
*Address for Correspondence: Dr. Franz Fogt, MD, med. M.B.A., Department of Pathology, Department of Ophthalmic Pathology (Scheie Eye Institute), WS 551, University of Pennsylvania, 39th and Market Streets, Philadelphia PA 19104, E-mail: fogt@mail.med.upenn.edu
Citation: Fogt F, Wellmann A, Lee V. Immunoglobulin G4-Related Disease (IgG4-RD) with Associated Sarcoidosis. J Ocular Biol. 2013;1(1): 3.Copyright © 2013 Fogt F, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Ocular Biology | ISSN: 2334-2838 | Volume: 1, Issue: 1
Submission: 25 June 2013 | Accepted: 15 August 2013 | Published: 19 August 2013
Abstract
Immunoglobulin G-4 related disease represents a collection of tumefactive entities associated with an abundance of infiltrating IgG4 positive plasma cells, which was described first in patients with chronic pancreatitis. Since then, IgG4 related disease has been described in multiple organ systems including the orbit. We describe here a patient with a history of sarcoidosis who was subsequently found to have IgG4 related disease of the orbits, diagnosed by histology and immunohistochemical staining for IgG and IgG4. Microscopic examination of the orbital biopsy demonstrated storiform fibrosis and obliterative phlebitis, as well as a specific IgG4 ratio > 40%. Six years prior, the patient was diagnosed with sarcoidosis clinically and histologically, which proposes the question of a relationship between the two entities. It is unclear from the literature whether IgG 4 related disease represents a diagnosis of its own, and therefore an incidental finding in our case; or whether it is associated with or a consequence of chronic inflammatory diseases in general or in specific cases such as long standing sarcoidosis. Chronic inflammatory processes are known to terminate in proliferative fibrosis at times, rich with IgG4 predominant plasma cells that are histologically identical to findings seen in IgG4 related disease.Introduction
Immunoglobulin G-4 related disease represents a collection of tumefactive entities associated with tissue infiltrating IgG4 positive plasma cells, which was described first by Hamano et al. in 2001 [1]. Here, the disorder was associated with chronic pancreatitis. The main features of IgG4 associated lymphoproliferative syndrome microscopically include tumor like swelling of the stroma with fibrosis, associated frequently with elevated serum IgG4 values in up to 86% of cases [2]. Key histological findings have since been determined, which include dense lymphoplasmacytic infiltrate, fibrosis that is at least focally storiform, and obliterative phlebitis [3].At least two of the three features should be present to make a confident diagnosis of IgG4 related disease [3].Since its initial description, IgG4 related disease has been described in every aspect of the human body, including the head and neck; thorax including breast; abdomen including hepatobiliary system and retroperitoneal structures, and even systemically. However, there appears to be an interesting high frequency of bulky inflammatory lesions of salivary type glands such as the lacrimal, parotid, and mixed salivary glands associated with IgG4 related disease. Moreover, histological resemblance of diseases previously known by different names have since then been subsumed under this new disease category. Sarcoidosis, contrarily, is a chronic granulomatous disease of unknown etiology that has not been systematically associated with IgG4 related disease with the exception of one single case report of contemporaneous involvement of chronic IgG4 associated pancreatitis and pulmonary sarcoidosis [4]. Metachronous development of IgG4 related disease years after a diagnosis of sarcoidosis has not been described previously. Here we present a case of a patient previously diagnosed with sarcoidosis who subsequently developed IgG4 related disease of the orbit.
Case Report
A 36-year-old African-American male presented with gradual onset of bilateral periorbital swelling of at least one-month duration. On exam, firm palpable masses were appreciated in both superior temporal orbits, which were causing significant proptosis and intermittent binocular diplopia. His past medical history was significant for pulmonary sarcoidosis, which was diagnosed six years prior with characteristic chest x-ray findings, pulmonary function tests, and transbronchial biopsy. The biopsy demonstrated noncaseating, granulomatous inflammation, negative for acid-fast bacilli and fungal organisms on special stains (Figure 1).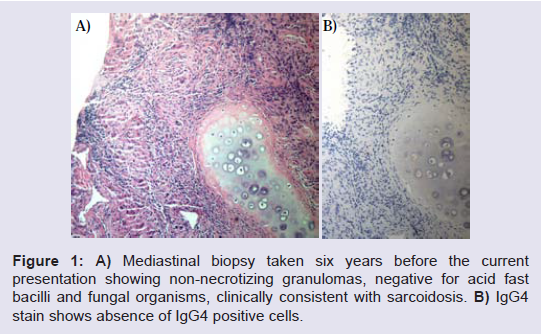
Figure 1: A) Mediastinal biopsy taken six years before the current presentation showing non-necrotizing granulomas, negative for acid fast bacilli and fungal organisms, clinically consistent with sarcoidosis. B) IgG4 stain shows absence of IgG4 positive cells.
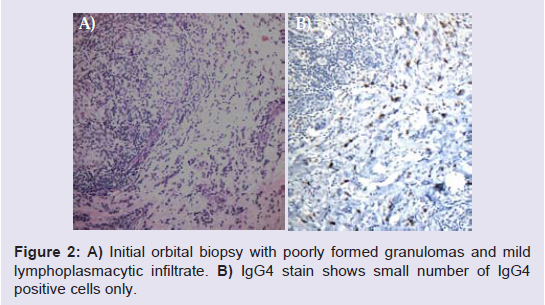
Figure 2: A) Initial orbital biopsy with poorly formed granulomas and mild lymphoplasmacytic infiltrate. B) IgG4 stain shows small number of IgG4 positive cells only.
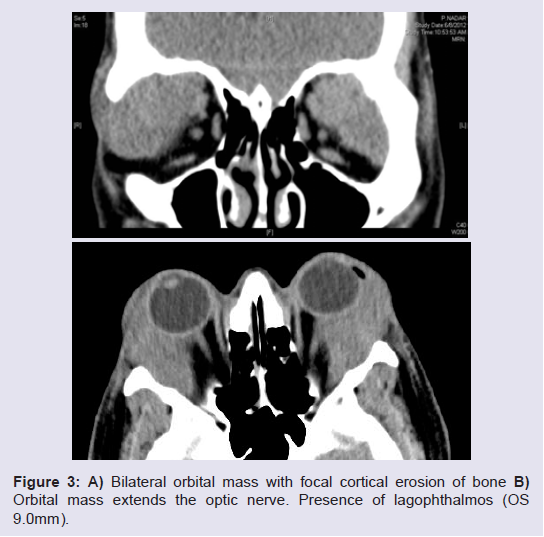
Figure 3: A) Bilateral orbital mass with focal cortical erosion of bone. B)Orbital mass extends the optic nerve. Presence of lagophthalmos (OS9.0 mm).
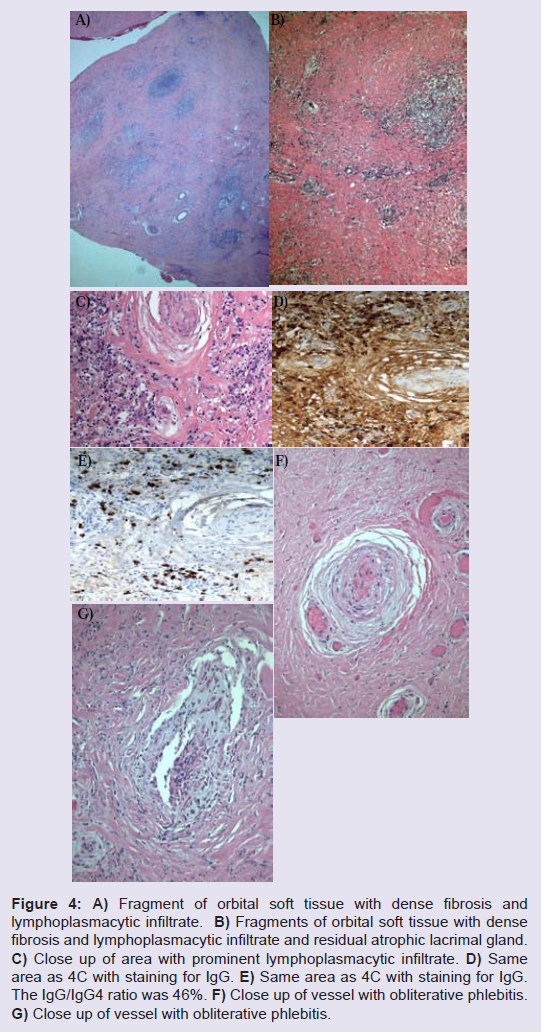
Figure 4: A) Fragment of orbital soft tissue with dense fibrosis and lymphoplasmacytic infiltrate. B) Fragments of orbital soft tissue with dense fibrosis and lymphoplasmacytic infiltrate and residual atrophic lacrimal gland. C) Close up of area with prominent lymphoplasmacytic infiltrate. D) Same area as 4C with staining for IgG. E) Same area as 4C with staining for IgG. The IgG/IgG4 ratio was 46%. F) Close up of vessel with obliterative phlebitis. G) Close up of vessel with obliterative phlebitis.
Discussion
The initial association between a tumefactive chronic inflammatory condition and IgG4 was made in cases of chronic inflammation of the pancreas, where the presence of IgG4 positive plasma cells in biopsied tissues and increased serum values of IgG4 were noted [5]. Subsequently, IgG4 related disease has been described in multiple organ systems, including the orbit.The main histological features of IgG4 associated lymphoproliferative syndrome include tumor like swelling of the stroma with fibrosis that has been classically described as storiform and a lymphoplasmacytic infiltrate with IgG4 positive plasma cells. In a recent consensus statement, three major histopathological features were determined to be significantly associated with IgG4 related disease: dense lymphocytic infiltrate, focal storiform fibrosis, and obliterative phlebitis [3]. A minimum of two out of the three criteria should be present in cases diagnosed as IgG4 related disease [3]. Associated elevated serum IgG4 values were also found to be increased in up to 86% of cases [2]. In rare cases, IgG4 related disease may be associated with hyperviscosity with polyclonal IgG4 predominant hypergammaglobulinemia [6].
Characteristic organ involvement includes salivary type glands, such as the pancreas, parotid and lacrimal glands, as well as small mixed salivary glands. Involvement of the pancreas is associated with type 1 autoimmune pancreatitis. The parotid, submandibular, and lacrimal glands, on the other hand, present with a specific distribution pattern, such as involvement of lacrimal gland with other salivary glands in Mikulicz’s disease, now called IgG4-related dacryoadenitis and sialadenitis [7]; and involvement of submandibular salivary glands with an inflammatory type tumor, known as Küttner’s tumor [8]. Other conjectured lesions include the lacrimal glands [9] and surrounding orbital soft tissue in the setting of idiopathic orbital inflammatory disease, representing IgG4-related orbital inflammatory disease or sclerosing dacryoadenitis [10].
The pathogenesis of IgG4 related disease is poorly understood. Both autoimmune and allergic disorders have been associated with the disease. In a recent review in the New England Journal of Medicine, Stone et al. proposed genetic alterations such as specific HLA subtypes; bacteria associated antibody cross reactions with pancreatic soft tissue; and autoimmune reactions against salivary gland duct epithelium as possible causes for the development of IgG4 associated disease [11].
Sarcoidosis is another tumefactive inflammatory disorder, characterized by non-necrotizing granulomas which may involve the orbit. An association between IgG4 related disease and sarcoidosis has not widely been published. The first report on the association of sarcoidosis and IgG4 related disease was by Michel et al. [4]. They reported a patient with IgG4 associated autoimmune pancreatitis and sarcoidosis of the salivary gland and celiac lymph nodes [4]. The clinical presentation and radiologic features confirmed sarcoidosis, while pancreas biopsies showed chronic pancreatitis with elevated serum IgG4 values. In the current case, sarcoidosis was diagnosed seven years prior to the development of his ocular findings. Similar to the first report, clinical and radiologic features confirmed a diagnosis of sarcoidosis. The orbital biopsies in this patient revealed lacrimal gland with fibrosis and non-necrotizing granulomas, which initially did not demonstrate significant increase of IgG4 positive cells but on subsequent biopsy did.
The question therefore arises whether the histological findings which led to the diagnosis of IgG4 related disease, namely the three major diagnostic criteria of dense lymphoplasmacytic infiltrate, storiform fibrosis, and obliterative phlebitis, represent a primary inflammatory event with secondary sequelae of organ destruction; or alternatively, does the development of IgG4 specific plasma cells represent an unusual late and secondary development from a primary chronic inflammatory event, in this case sarcoidosis. It has been shown that IgG4 associated immune complexes inhibit immune precipitation and complement activation by IgG antibodies [12]. Additionally, IgG4 may protect against the effects of complement fixing IgG1 classes [13]. Thus, a chronic inflammatory response may, in certain situations, change venue from an IgG1 or IgE response to an IgG4 driven response. Such IgG changes have been observed in asthmatic patients treated with immunotherapy, where a switch to IgG4 resulted in an altered immunologic response not seen in patients without an IgG4 shift [13]. This may be supported further by previous observations of spontaneous regression of IgG4 related lesions in the lung and the lacrimal gland [14,15]. In the case demonstrating regression of lung involvement, an altered immune response secondary to the biopsy was assumed to be responsible for the regression of the disease [14]. In addition, spontaneous regression in a case of dacryoadenitis was also reported, where a potential T-cell mediated response, secondary to infection or trauma, leading to spontaneous regression similar to regression of B-cell lymphoma was purported [15]. A recent study reviewing patients with suspected sarcoidosis prospectively over five years noted a subset of patients with sarcoidosis who showed increased serum IgG4 and increased serum IgG4/IgG values [16]. This suggests that long standing sarcoidosis may be associated with a serum IgG value distribution similar to that seen in IgG4 related disease. Additional studies therefore need to be designed to review the pattern of IgG response in these tumefactive lesions to further define and delineate IgG4 related mass lesions.
References
- Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, et al. (2001) High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med 344 :732-738.
- Zen Y, Nakanuma Y (2010) IgG4-related disease: a cross-sectional study of 114 cases. Am J Surg Pathol 34: 1812-1819.
- Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, et al. (2012) Consensus statement on the pathology of IgG4-related disease. Mod Pathol 25: 1181-1192.
- Michel L, Clairand R, Néel A, Masseau A, Frampas E, et al. (2010) Association of IgG4-related disease and sarcoidosis. Thorax 66: 920-921.
- Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, et al. (2003) A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol 38: 982-984.
- Wong PC, Fung AT, Gerrie AS, Moloney G, Maberley D, et al. (2013) IgG4-related disease with hypergammaglobulinemic hyperviscosity and retinopathy. Eur J Haematol 90: 250-256.
- Takahashi H, Yamamoto M, Suzuki C, Naishiro Y, Shinomura Y, et al. (2010) The birthday of a new syndrome: IgG4-related diseases constitute a clinical entity. Autoimmun Rev 9: 591-594.
- Kitagawa S, Zen Y, Harada K, Sasaki M, Sato Y, et al. (2005) Abundant IgG4-positive plasma cell infiltration characterizes chronic sclerosing sialadenitis (Küttner's tumor). Am J Surg Pathol 29: 783-791.
- Cheuk W, Yuen HK, Chan JK (2007) Chronic sclerosing dacryoadenitis: part of the spectrum of IgG4-related Sclerosing disease? Am J Surg Pathol 31: 643-645.
- Sato Y, Ohshima K, Ichimura K, Sato M, Yamadori I, et al. (2008) Ocular adnexal IgG4-related disease has uniform clinicopathology. Pathol Int 58: 465-470.
- Stone JH, Zen Y, Deshpande V (2012) IgG4-related disease. N Engl J Med 366: 539-551.
- van der Zee JS, van Swieten P, Aalberse RC (1986) Inhibition of complement activation by IgG4 antibodies. Clin Exp Immunol 64: 415-422.
- Nakagawa T, Miyamoto T (1985) The role of IgG4 as blocking antibodies in asthmatics and in bee keepers. Int Arch Allergy Appl Immunol 77: 204-205.
- Seki N, Yamazaki N, Kondo A, Nomura K, Himi T (2012) Spontaneous regression of lung lesions after excision of the submandibular gland in a patient with chronic sclerosing sialadenitis. Auris Nasus Larynx 39: 212-215.
- Kase S, Yamamoto T, Ishijima K, Noda M, Ishida S (2012) Spontaneous regression of IgG4-related dacryoadenitis. Mod Rheumatol [Epub ahead of print].
- Tsushima K, Yokoyama T, Kawa S, Hamano H, Tanabe T, et al. (2011) Elevated IgG4 levels in patients demonstrating sarcoidosis-like radiologic findings. Medicine (Baltimore) 90: 194-200.