
Journal of Oral Biology
Download PDF
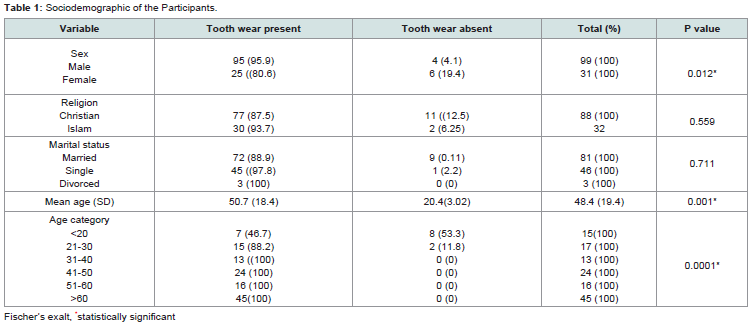 Table 1: Sociodemographic of the Participants.
Table 1: Sociodemographic of the Participants.
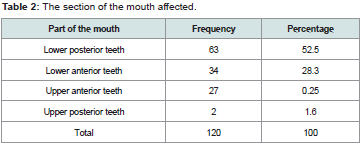 Table 2: The section of the mouth affected.
Table 2: The section of the mouth affected.
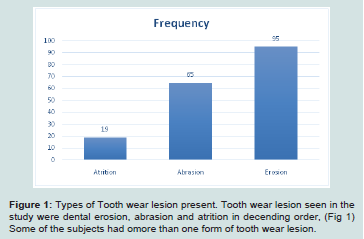 Figure 1: Types of Tooth wear lesion present. Tooth wear lesion seen in the
study were dental erosion, abrasion and atrition in decending order, (Fig 1)
Some of the subjects had omore than one form of tooth wear lesion.
Figure 1: Types of Tooth wear lesion present. Tooth wear lesion seen in the
study were dental erosion, abrasion and atrition in decending order, (Fig 1)
Some of the subjects had omore than one form of tooth wear lesion.
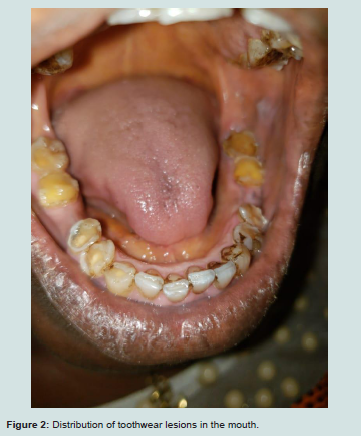 Figure 2: Distribution of toothwear lesions in the mouth.
Figure 2: Distribution of toothwear lesions in the mouth.
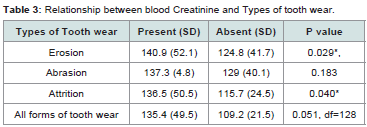 Table 3: Relationship between blood Creatinine and Types of tooth wear.
Table 3: Relationship between blood Creatinine and Types of tooth wear.
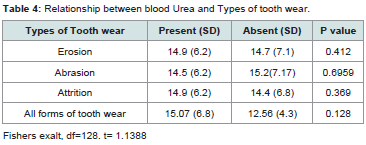 Table 4: Relationship between blood Urea and Types of tooth wear.
Table 4: Relationship between blood Urea and Types of tooth wear.
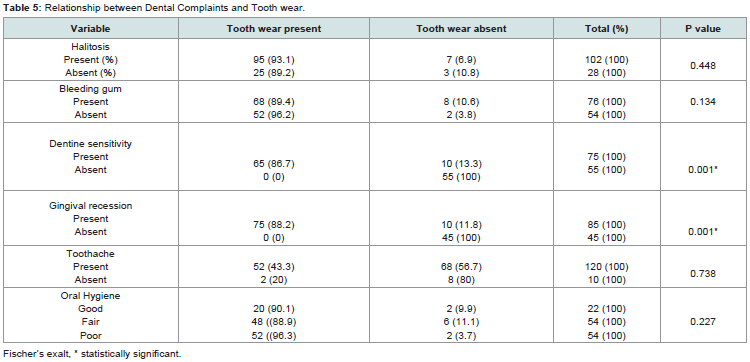 Table 5: Relationship between Dental Complaints and Tooth wear.
Table 5: Relationship between Dental Complaints and Tooth wear.
Research Article
Distribution and Clinical Implications of Tooth Wear Lesions among Chronic Kidney Disease Patients Attending a Tertiary Hospital in South Western Nigeria
Oyetola EO1*, Ayodele OA1, Ojo OM1, Mogaji IK2 and Aremu OA3
1Department of Preventive and Community Dentistry, Obafemi Awolowo University, Nigeria
2I K Department of Preventive and Community Dentistry, Obafemi Awolowo University, Nigeria
3Department of Medicine, Obafemi Awolowo University, Nigeria
*Address for Correspondence Oyetola EO, Department of Preventive and Community Dentistry, Obafemi Awolowo University, Ile Ife, Nigeria; E-mail: phemyhoye12@yahoo.com
Submission: 14 January 2020;
Accepted: 24 February 2020;
Published: 27 February 2020
Copyright: © 2020 Oyetola EO, et al. This is an open access article
distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Abstract
Background:
Often times, the oral health care of chronic renal failure
patients are often neglected, leaving such patients with serious complaints.
Tooth wear lesion is one of such problems which are often complicated
with dentinal and pulpal exposure. Little is known about its distribution and
clinical implications in renal patients.
Methodology:
This cross-sectional study was conducted among
chronic kidney patients being managed with medication and hemodialysis
attending at the renal Unit of the Obafemi Awolowo University, Ile- Ife. The
participants were selected using simple random methods from among
the pool of patients receiving treatment in the Renal clinic. Biodata of
each patient was recorded. They were also interviewed for presence of
oral complaints and other systemic problems. Oral examination was then
conducted on each participant, each tooth was examined for tooth wear
lesion and other oral problems. Blood sample was also taken for blood
creatinine and urea. Data was analyzed using STATA 14.
Results:
A total of 130 (99 male and 31 female) renal patients
participated in the study out of which 120 (92.3%) had form of tooth wear
lesions. Majority of those with oral lesion were above 60 years old. Tooth
wear lesion see were dental tooth wear lesion see were dental erosion
(95), attrition and abrasion. More than half (63, 52.5%) of the tooth wear
lesions were seen in the lower posterior teeth, followed by lower anterior
teeth and upper anterior teeth. Higher concentration of creatinine and
urea was associated with presence of tooth wear lesion. Lesions seen with
renal patients with oral lesion are dentine hypersensitivity, gingival recession.
Others are tooth ache, halitosis and tooth mobility.
Conclusion:
Prevalence of tooth wear lesion in renal patients was 92.3%.
The most frequent tooth wear lesion seen was dental erosion. The teeth in
the lower posterior segment of the mouth was the most frequently affected.
The blood urea and creatinine concentration were significantly higher in
patients with tooth wear lesion.
Introduction
Human teeth function together as a team and are important in
feeding (mastication), speech, self-defense, aesthetics and forensic
odontology [1]. Each types of teeth are known with their distinct
shape, sizes, angulation and position which is important in their
respective functions. However, the shapes and sizes tend to be altered
as the teeth naturally perform its function due to physiological loss
of tooth tissue, this is common during mastication [2]. The frequent
intake of some tooth wearing (hard) foods and presence of substances
(internal or external sources) that can predispose to tooth wear
lesions such acidic. Such external (such as medications or foods,
and appliance) and internal (such as regurgitation of gastric content
into the oral cavity) substances often predispose to the tooth wear
[2]. Since the formation of enamel (Amelogenesis) is completed by
the death of all ameloblast before eruption, repairs following tooth
eruption becomes impossible [3].
Common types of tooth wear are erosion, abrasion, attrition and
abfraction. Dental attrition is caused by tooth to tooth contact in the
mouth, it’s usually results from malocclusion and oral habits. Tooth
wear in dental abrasion is usually results from hard contact between
teeth and foreign substances such as tooth brush. Dental erosion
is caused by chemical substances such as acids that are introduced
internally or eternally into the oral cavity. Abfraction which is due to
flexure of the teeth from occlusal forces is not very common. Unlike
dental caries which is also a form of tooth wear, the above types of
tooth wear are physiological tooth wear lesions and are not due to any
microorganism [4]. Clinically attrition is noted with the presence of
wear facet at the point of opposing teeth and tends to be rough while
abrasion is seen at the site of foreign substances introduced usually at
the cervical margin. Dental erosion which is due to acidic substances
in contact with the teeth is usually smooth and are often seen on the
occlusal surfaces of the affected teeth or any other location where the
acid is in contact with the mouth [4].
Tooth wear lesions, if left untreated may progress to dentinal
exposure and eventual pulpal exposure. This (Dentinal and pulpal
exposure) lead to insult on the exposed dentine and pulp resulting
in dentinal hyper creativity and pulpitis respectively. Common
symptoms are the presence of sharp excruciating pain which
aggravated by air, touch and cold stimulus. This usually affect the
quality of life of the affected patients [5]. Other possible secondary
complications are periodontitis and periodontal abscess and space
infection.
Patients with chronic kidney disease are known to have raised
concentration of blood urea and in many cases are often complicated
with uremic syndrome, a clinical condition characterized by the retention of a host of compounds (such as urea) which in healthy
subjects are secreted into the urine by the healthy kidneys [6]. The
retained unwanted substances cause gross disturbances in almost all
organs/systems in the body such as gastroenteritis (uremic gastritis),
nervous system (uremic encephalopathy), hematology (anemia,
bleeding tendencies). Ureamic patients, therefore, due to gastric
irritation tends to vomit acidic gastric content of the stomach into the
mouth thus lowering the pH of the mouth predisposing the affected
teeth to tooth wear. The contact of the acidic gastric content with such
teeth will result in dental erosion, a common form of tooth wear and
also predisposes the teeth to other forms of tooth wear [7]. Moreso,
raised blood urea tends to bring about raised salivary urea because
primary saliva is essentially an ultra filtrate of plasma this further
lowers the mouth pH [8]. Ureamia also affects tooth development
and may predisposed to tooth hypoplasia, anther condition that may
further predispose a tooth to attrition abrasive tooth loss.
Scientific studies had reported higher prevalence of tooth wear
lesion in renal patients Klassen et al. in a study among patients on
dialysis reported a prevalence of 67% [9,10]. Because of the associated
complications of toothwear such as dentine sensitivity, pulpitis and
difficulty of eating, most patients suffer in silence as they cannot
feed nor use their medication effectively Unfortunately, studies
evaluating the relationship between the Chronic Kidney Disease
(CKD) and tooth wear lesions are scanty and emphasis on the
distribution of the tooth wear is grossly deficient in the literature
especially in African population where the prevalence of CKD is
on the increase. Information on relative distribution of toothwear
lesion is important in planning and preventive measure especially in
resource limited environment. This justifies the presence study which
is aimed at determine the distribution and clinical implications of
tooth wear lesions among CKD patients with a view to providing
appropriate recommendations on the prevention and appropriate
treatment strategies towards avoiding associated complications of
this distressing condition among renal patients.
Materials and Methods
Study Design:
This study was designed as a cross-sectional study
to determine the pattern of distribution of tooth wear lesions among
chronic renal patients
Subjects Selection:
Participants for this study were randomly
selected from the pool of patients on hemodialysis being managed
at attending renal Unit of Obafemi Awolowo University Teaching
Hospitals complex. Simple random sampling method was used to
select the participants. Each consenting patient were asked to blindly
pick from a box containing papers marked YES or NO, only those
whom picked YES were recruited. The details of the study were duly
explained to the patients.
Selection criteria:
Dentate patients with established case of
chronic kidney failure on hemodialysis and medications. Patients
with anorexia nervosa or bulimia nervosa or any debilitating disease
were excluded from the study.
Ethical consideration:
Ethical approval was obtained from the
Ethics and Research Committee of Obafemi Awolowo University Ile
Ife.
Data Collection
Data collection was recorded with use of questionnaire which was
organized into sections. Section A recorded the biodata of the patients
such as age, sex, and marital status. The section B records information
on oral and systemic symptoms associated with their kidney disease.
Specific oral symptoms/lesions that were evaluated include dentinal
hypersensitivity, tooth ache, tooth mobility, gingival recession, and
bleeding gum. Any other oral lesions were also recorded.
Section C records the finding from oral examinations.
Examination was done with patient comfortably sitting on a chair
of a well illuminated room in the clinic. Extra oral examination
done include checking for asymmetry, temporomandibular joint
tenderness and the integrity of sub mandibular lymph nodes. The
mouth is then thoroughly examined determine the oral hygiene status
using Green and Vermiliion criteria. Mouth opening was assessed
by measuring interincisal distance with the aid of Venieer caliper
findings, interincisal distance of between 3-6 cm was taken as normal.
Halitosis was also assessed with organoleptic method following
validation of the examiner using Miyazali method. Patients with or
above the point of perceivable order (score 2 and above) was taken as
having halitosis. Each tooth was examined also for gingival recession,
the migration of apical gingival below mucogingival junction was
taken as gingival recession. Oral mucosa was also examined for
presence of macular and papillary and white lesion and the findings
were recorded accordingly.
Hard tissue examination was also done by checking for their
integrity of the teeth. Tooth mobility was checked for by using
bimanual palpation. Attrition was diagnosed with the presence of wear
facet on the tooth at the point of tooth to tooth contact as well as the
presence of sharp borders. Abrasion was diagnosed when worn area is
devoid of tooth to tooth contact but evidence/history of introduction
of foreign substances into the mouth usually as tooth cleaning aid
(hard toothbrush), oral application e.t.c. In addition, surfaces of
abrasive tooth wear are rough and tend to follow the motion or forms
of application of the implicated foreign appliances. Dental erosion on
the other side was diagnosed when the tooth wear lesion is smooth
and rounded with no tooth to tooth contact, introduction of foreign
substances or infectious decay of the teeth.
Blood samples of the subjects were also taken and are transported
to the laboratory for assessment of blood urea and creatinine
Data analysis:
Data were analyzed using STATA 10 statistical software.
Continuous variables such age, blood urea and blood creatinine
were analyzed using mean, media and mode. For qualitative
variables such as the presence or absence of tooth wear lesion as
well as other oral symptoms, they were analyzed with frequency and
percentages, comparison of proportion were made using Fischer’s
exalt. For continuous variables were subjected to parametric test and
comparison of mean was done using appropriate test such as Students
t-test or Rank sum test as the case may be, p set at p< 0.05.
Results
Out of the 130 (99 male and 31 female) Chronic Kidney Disease patients that participated in the study, 120 (92.3%) had tooth wear
lesion. More than three quarter of those with tooth wear lesions were
male and of Christian religion. The mean age of those who developed
tooth wear lesion is significantly higher than those without the lesion.
Tooth wear lesion was most frequent among those older than 60 years
(Table 1).
The section of the mouth affected:
More than half (63,52.5%) of the tooth wear lesions were seen in
the lower posterior teeth, followed by lower anterior teeth and upper
anterior teeth. The upper posterior teeth were the least frequently
involved (Table 2 and Figure 1).
The section of the mouth affected:
More than half (63,52.5%) of the tooth wear lesions were seen in
the lower posterior teeth, followed by lower anterior teeth and upper
anterior teeth. The upper posterior teeth were the least frequently
involved (Table 2 and Figure 2).
Relationship between blood Creatinine, blood Urea and Types of tooth wear Lesion:
The mean blood creatinine was higher among those with all
tooth wear lesions but the difference was not statistically significant
(p=0.51) However, when each type of toothwear lesion is considered
individually: participants with attrition and erosion has a significant
increased blood creatinine (p=0.04 and 0.029 respectively. Likewise,
blood urea of those with dental tooth wear were higher than
those without tooth wear but the differences were not statistically
significant, p=0.128 (Table 3-5).
Discussion
Tooth wear lesion is one of the common oral manifestations
of renal patients [9]. It is associated with wide range of clinical
presentation depending on the severity of toothwear and type of teeth
affected. Following tooth wear, the associated dentinal and pulpal
exposure results in complications such as dentine hypersentivity,
pulpitis, crack tooth syndrome and periodontitis. These are clinical conditions that are associated with pain, discomfort and tends
to impair the quality life of affected patients [11].In this study, we
found the prevalence of toothwear lesions to be 92.3% and this is
significantly higher than the prevalent of tooth wear lesion in a group
of study participants in Benin city, Nigeria which was reported by
Ojehanon to be 17% [12]. The present study was conducted among
patients with oral complication from their systemic (renal) problems,
this, in addition to the relative older age group may be responsible
for the higher value in this study. The commonest form of tooth
wear lesion seen in this study was dental erosion and was found to
be present in70 (54%) patents. This may be due to acidic nature of
the oral environment of renal patients which predisposes to dental erosion. This results is also higher than the reports of Imirzalioglu
et al. which conducted among chronic renal failure patients which
showed a prevalence of 65% of erosion like lesion among chronic
renal failure patients [9]. Unlike Ojehanon et al. who found the
commonest toothwear lesion to be attrition, we found, in this study,
dental erosion as the commonest tooth wear lesion, seen in 70 (54%)
followed by abrasion and attrition. Tooth wear in chronic renal failure
is multifactorial. Constant regurgitation and gastro-esophageal reflux
in uremic patients lead to introduction of gastric acids in the oral
cavity. Tooth wear (erosion) results when acidic substance come in
contact with vulnerable tooth [7]. More so, chronic periodontitis
and gingival recession are prominent oral features in chronic renal
patients. Following gingival recession from the periodontal pathology
[13], exposure of the coronal pat of the root is inevitable and the
overlying cementum (of the root surface) is more vulnerable to wear
during tooth brushing compared to the enamel of the crown. Due to
poor oral hygiene and uremic smell, patients tend to observe more
aggressive tooth brushing with a view to alleviating the odour but this
will rather further compromise the integrity of the tooth structure,
leading to tooth wear. Enamel hypoplasia which is also known to be
prevalent in renal patients also further rendering the tooth to tooth
wear by attrition and abrasion.
Although any tooth can be affected by tooth wear in as much as it
is in contact with acidic substanbces, our study showed that the lower
posterior teeth the most frequent tooth affected by tooth wear, this
findings is in agreement with the findings of Braimoh et al. [14]. The
acidic content of regurgitated gastric juice and saliva tends to settle
in the floor of the mouth and occlusal surfaces of teeth and since
lower most proximal to the pharynx they are mostly to be the first to
be affected having also aided by gravity [7]. A study by Wang et al.
however reported upper central incisor as the most frequently teeth
affected, the study was however, conducted among children without
chronic kidney disease [15].
Blood creatinine is a good indicator of renal disease as chronic
kidney patients usually have significantly increased creatinine
concentration which is usually persistent as long as patient’s kidney
could not perform its physiological function of getting the body rid
of nitrogenous waste products. In this study, patients with tooth wear
lesion had a significantly higher concentration of blood creatinine
than those without tooth wear. This is in agreement with earlier
studies which showed that erosion and other tooth care lesion are
complications of chronic kidney disease which is associated with
elevated blood creatinine [9,16]. Likewise, blood urea was also found
to be higher among chronic kidney disease patients with dental wear
in this study consistent with Imirzalioglu et al. [9]. Patients with
chronic kidney disease tends to have raised salivary urea, studies
had shown that the presence of excess salivary urea tends to increase
plaque, a condition which is necessary for both physiological tooth
wear lesion and dental caries [17]. Acids are known for their ability to
dissolve the hydroxy appetite in dental hard tissue unlike floroapetite
which is resistant [18].
Patients with dental tooth wear tends to present with some oral
complaints which can be quite disturbing, affecting the quality of life
of affected individuals. In this study, the frequency of occurrence
of dentine sensitivity among renal patients with tooth wear lesion
was significantly higher. Similar relationship was observed with
gingival recession [19]. Tooth wear lesion may be complicated with
exposure of the dentinal tubules and the presence of stimulus such
as air or cold stimulus, the shock like pain signal is transmitted via
the exposed dental tubules to the pulp which will be perceived as
dentine hypersensitivity [20], Factors which predisposes to gingival
recession such as wrong brushing habit using third tooth brush might
as well responsible for tooth wear lesion. Halitosis, bleeding gum and
tooth ache were also more frequency seen in renal patients with tooth
wear lesion. The presence of tooth wear may create rough surface
which precludes effective tooth brushing and tends to encourage
plaque accumulation and hence accumulation of bacteria that may
cause inflammation of tooth supporting tissue, bleeding gum and
periodontal infection [21].
Conclusion
Prevalence of toothwear lesion is significantly higher among renal
patients. The commonest tooth wear lesion was dental erosion closely
followed by attrition. Lower posterior teeth were the most frequent
teeth affected. Common oral complaints among renal patients tooth
wear lesion is dentine hypersensitivity, gum bleeding and toothache.
Since majority of renal patients with tooth wear lesion has oral lesions
it is recommended that prophylactic dental treatment to prevent
dental tooth wear such as fluoride therapy, avoidance of refined sugar
consumption and maintenance of good oral hygiene and correct
tooth brushing method. Patients with chronic renal failure are thus
advised to pay much attention to their oral health.
References
Citation
Oyetola, EO, Ayodele OA, Ojo, OM, Mogaji, IK and Aremu, OA. Distribution and Clinical Implications of Tooth Wear Lesions among Chronic Kidney Disease Patients Attending a Tertiary Hospital in South Western Nigeria. J Oral Biol. 2020; 7(1): 5.