
Research Article
*Address for Correspondence: Sang Choon Cho, Ashman Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, USA, E-mail: scc2@nyu.edu
Citation: Lagoudis M, Ceballos L, Manasse M, Trushkowsky RD, et al. 3-D Printed Bite Registration Jigs for Distal Free End Implant Restorations. J Oral Bio. 2016; 3(2): 4.
Copyright © 2016 Lagoudis, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Oral Biology | ISSN: 2377-987X | Volume: 3, Issue: 2
Submission: 08 July, 2016 | Accepted: 20 July, 2016 | Published: 25 July, 2016
Reviewed & Approved by: Reviewed & Approved by: Dr. George E. White, Department of Pediatric Dentistry at Nova Southeastern University, USA






 The conventional method requires a construction of a base and a wax occlusal rim to provide adequate support for the registration material and to facilitate mounting of an opposing cast (Figure 8) [5].
The conventional method requires a construction of a base and a wax occlusal rim to provide adequate support for the registration material and to facilitate mounting of an opposing cast (Figure 8) [5].
 The extra time required to fabricate the working cast and record base results in increased cost and necessitates additional appointments. Inaccuracies may also be incorporated due to compression of the ridge under the record base [6].
The extra time required to fabricate the working cast and record base results in increased cost and necessitates additional appointments. Inaccuracies may also be incorporated due to compression of the ridge under the record base [6].
 An alternative technique that has been reported is the use of the healing abutments that are located within an edentulous distal extension space (Figure 10). Those serve as the vertical stops for an interocclusal record with the use of acrylic resin. Nevertheless, this requires having the same healing abutments that the patient has in the mouth, which in turn, increases the fee and patient discomfort due to the acrylic resin [8]. Another disadvantage is the positioning of the healing abutments on the cast. This is occurring because it is not going to be exactly the same as intraorally due to the different torque and the non-engaging nature of the healing abutments. This technique may also not be the most accurate, because healing abutments are short, so the space between them and the opposing dentition is usually more than 5mm. This results in the use of undesirable amount of autopolymerizing acrylic resin to fill the space leading to shrinkage and possible inaccuracy.
An alternative technique that has been reported is the use of the healing abutments that are located within an edentulous distal extension space (Figure 10). Those serve as the vertical stops for an interocclusal record with the use of acrylic resin. Nevertheless, this requires having the same healing abutments that the patient has in the mouth, which in turn, increases the fee and patient discomfort due to the acrylic resin [8]. Another disadvantage is the positioning of the healing abutments on the cast. This is occurring because it is not going to be exactly the same as intraorally due to the different torque and the non-engaging nature of the healing abutments. This technique may also not be the most accurate, because healing abutments are short, so the space between them and the opposing dentition is usually more than 5mm. This results in the use of undesirable amount of autopolymerizing acrylic resin to fill the space leading to shrinkage and possible inaccuracy.
 On the other hand, one manufacturer has developed a specific plastic “bite registration aid” (Straumann AG, Basel, Switzerland), specifically made applicable on their dental implants in order to obtain and transfer an interocclusal record (Figure 11). Although this bite registration aid eliminates the necessity of constructing a tissue supported record base, it still remains expensive and is disposable. Moreover, its use is limited to one implant system.
On the other hand, one manufacturer has developed a specific plastic “bite registration aid” (Straumann AG, Basel, Switzerland), specifically made applicable on their dental implants in order to obtain and transfer an interocclusal record (Figure 11). Although this bite registration aid eliminates the necessity of constructing a tissue supported record base, it still remains expensive and is disposable. Moreover, its use is limited to one implant system.

3-D Printed Bite Registration Jigs for Distal Free End Implant Restorations
Miltiadis Lagoudis, Lara Ceballos, Maryse Manasse, Richard D. Trushkowsky, Yung Cheng Paul Yu and Sang-Choon Cho*
- Ashman Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, USA
*Address for Correspondence: Sang Choon Cho, Ashman Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, USA, E-mail: scc2@nyu.edu
Citation: Lagoudis M, Ceballos L, Manasse M, Trushkowsky RD, et al. 3-D Printed Bite Registration Jigs for Distal Free End Implant Restorations. J Oral Bio. 2016; 3(2): 4.
Copyright © 2016 Lagoudis, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Oral Biology | ISSN: 2377-987X | Volume: 3, Issue: 2
Submission: 08 July, 2016 | Accepted: 20 July, 2016 | Published: 25 July, 2016
Reviewed & Approved by: Reviewed & Approved by: Dr. George E. White, Department of Pediatric Dentistry at Nova Southeastern University, USA
Abstract
Objective: To demonstrate a technique to minimize the cost and the time by recording the bite at the time of impression taking procedure.Materials and methods: During the impression procedure, bite registration was obtained, by engaging one Bite Registration Jig (BRJ) on the distal implant. Vertical height was adjusted instantly, using a round-end taper acrylic bur. Retention grooves were pre-designed and fabricated by the printer. Blu-Mousse material was injected around the fabricated jig and patient occluded in a centric relation position. Subsequently, the BRJ, embedded in Blu-Mousse material, was used extraorally to mount the fixture level cast with the opposing cast.
Results: All implant restorations had stable interocclusal contacts with no eccentric contacts, hence all accepted. All the four Fixed Dental Prostheses were delivered at the try in procedure, with minimal chair side adjustments using the porcelain polishing burs.
Conclusion: Bite registration with BRJ is an accurate and effective technique, which can be used for the distal extension implant cases. In addition, unlimited BRJ’s can be produced by the 3D printing in a short amount of time and inexpensively.
Introduction
Before mankind was introduced to sugarThe accurate transfer of intra-oral information for extraoral use is the purpose of impression taking and is the first step of successful restorative procedures [1]. Moreover, this transfer of intra-oral information to a maxillary and a mandibular cast requires appropriate articulation. In order to mount the casts in the correct and reproducible position, three points of contact need to be established. These points of contact should be adequately spaced so as to provide adequate stability [2]. An adequate bite registration is the key to provide the correct orientation between the maxillary and mandibular casts and is often not considered.
Accurate recording of maxillary-mandibular relations will minimize occlusal adjustments that are required when placing final restorations [3]. Inaccurate mounting of casts can create havoc when fitting the restorations as they may be too high or not in occlusal contact. Either may result in the need for a new restoration. This may be detrimental to the longevity of the restoration and involves increased treatment time and possibly expense.
Ideally, occlusal stops should consist of three adequately spaced points of stabilization so as to provide a stable tripod. Missing teeth eliminates the more traditional means of stabilization. If the missing teeth are distally located, the soft tissue of the edentulous region has to be utilized to establish the tripod. This will greatly diminish the stability of the final record. To properly incorporate the edentulous area, construction of a base and a wax occlusal rim are required to provide adequate support for the registration material and to facilitate mounting of an opposing cast [4]. Unfortunately, additional treatment time and appointments may be required to fabricate a master working cast and record base [5]. However, due to the compressible nature of the edentulous ridge, a degree of distortion may be present and create some inaccuracy of the bite registration [6]. Several techniques have been introduced in order to eliminate the necessity of constructing a tissue supported record base. These included provisional restorations, Bite Registration Aid (Straumann AG, Basel, Switzerland), Implant Bite Posts (IBP™, Lebeau Dental), adjusted height of temporary cylinders, and auto-polymerizing resin between healing abutments and the opposing occlusal plane with the remaining teeth, in maximum intercuspation [7,8]. All of the above can be costly and time consuming.
At the time of the impression procedure, bite registration can be accomplished, by engaging one Bite registration Jig(BRJ) on the distal implant. Fabricated by a 3-D printer (Formlab Inc, Somerville, MA). Vertical height can be adjusted intraorally in a short time using a round - end tapered carbide bur (Brasseler USA, Savannah, GA). Retention grooves are pre-designed and fabricated by the printer. Bite registration material can be injected around the BRJ and patient occludes in a centric relation position. Subsequently, the BRJ, embedded in the bite registration material, can be used extraorally to mount the fixture level cast with the opposing cast. This has the potential to be a very promising technique regarding bite registration, for distal extension implant restorations, via a BRJ.
The purpose of the present case series is to demonstrate a technique that minimizes cost, time, and complications by recording the bite at the time of the impression taking procedure utilizing 3-D printer fabricated bite registration jigs.
Materials and Methods
Clinical data in this study was obtained from the Implant Database (ID). This data set was extracted as de-identified information from the routine treatment of patients at the Ashman Department of Periodontology and Implant Dentistry at New York University College of Dentistry. The ID was certified by the Office of Quality Assurance at NYUCD. This study is in compliance with the Health Insurance Portability and Accountability Act (HIPAA) requirements.Study subjects
Three subjects with posterior edentulous spans were included in the study. They were retrospectively chosen from the ID having satisfied the inclusion/exclusion criteria of the study. The first subject had a two unit implant supported Fixed Dental Prosthesis (FDP). The second subject had a three unit implant supported FDP with a mesial cantilever. The third subject had a single unit implant supported FDP on the mandibular right (area # 30) and a single unit FDP on the mandibular left side (area # 19). All the subjects selected had to have had the permanent implant restoration in function for a minimum of 6 months. The population consisted of 1 male and 2 female patients with a mean age of 50 years (range: 29 to 65).
Each subject selected from the database for this study had to have conformed to the following criteria prior to undergoing the bite registration technique. Inclusion criteria were: a unilateral posterior edentulous span, minimum one missing tooth, maximum 3 missing teeth, and intact opposing dentition. Exclusion criteria were: bilateral edentulous span, more than 3 missing teeth and opposing arch was edentulous.
The clinical procedures were standardized and followed the steps as described below: Pick up impression was taken fist using a polyether material - Impregum (3M - ESPE).
At the same appointment, bite registration was performed by engaging one BRJ on the distal implant (Figures 1 and 2). Vertical height was then adjusted, intraorally, using a round - end tapered carbide bur (Brasseler USA, Savannah, GA). Retention grooves were fabricated by the printer (Figures 3a and 3b). Bite registration material, Blu-Mousse (Parkell Bio-Materials, Farmingdale, NY), was injected around the BRJ and the patient was instructed to close in a centric relation position (Figure 4). Subsequently, the BRJ, embedded in the bite registration material, was used extraorally to mount the fixture level cast with the opposing cast (Figures 5 and 6). Finally, insertion of the prosthesis at the try-in procedure was done (Figure 7).
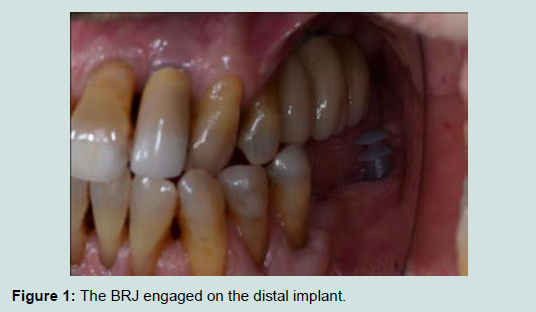
Figure 1: The BRJ engaged on the distal implant.
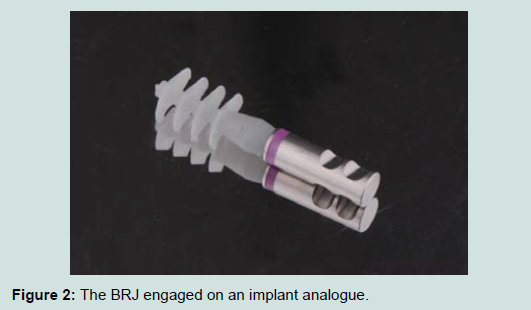
Figure 2: The BRJ engaged on an implant analogue.
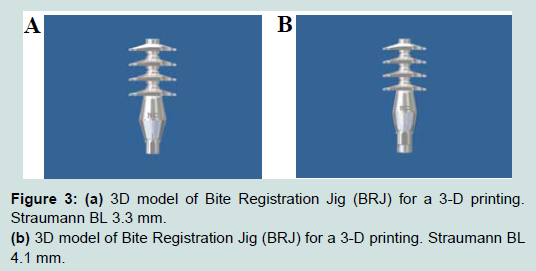
Figure 3: (a) 3D model of Bite Registration Jig (BRJ) for a 3-D printing. Straumann BL 3.3 mm.(b) 3D model of Bite Registration Jig (BRJ) for a 3-D printing. Straumann BL4.1 mm.

Figure 4: The bite registration material was injected around the BRJ just before the patient closed in centric relation.

Figure 5: The BRJ embedded with bite registration material as the interocclusal record.

Figure 6: Articulation of fixture cast and opposing cast utilizing the BRJ interocclusal record.
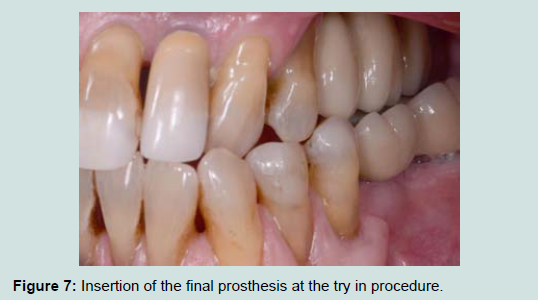
Figure 7: Insertion of the final prosthesis at the try in procedure.
Results
All implant restorations had stable interocclusal contacts with no eccentric contacts, hence all accepted. All the four FDPs were delivered at the try-in procedure, with minimal chairside adjustments using the porcelain polishing burs.
Discussion
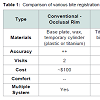
A comparison of similar techniques of bite registration for distal extension implant restorations is contained in Table 1. These techniques included the conventional - occlusal rim, temporary cylinders, auto polymerizing resin - healing abutments, bite registration aid and BRJ.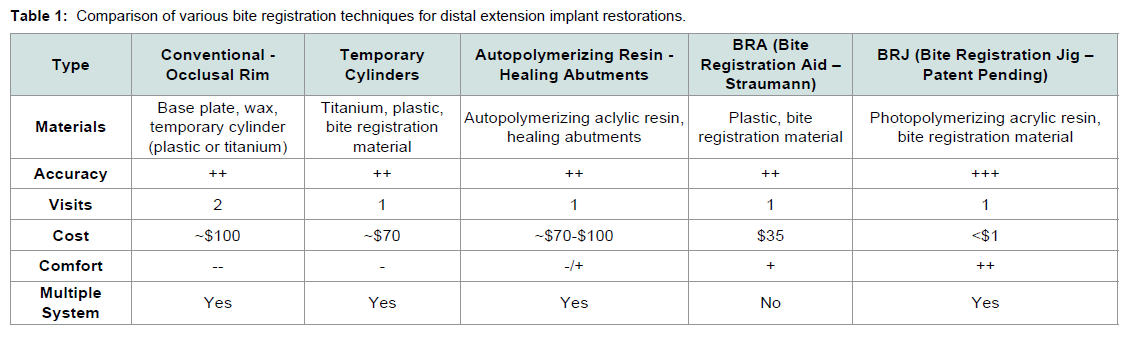
Table 1: Comparison of various bite registration techniques for distal extension implant restorations.
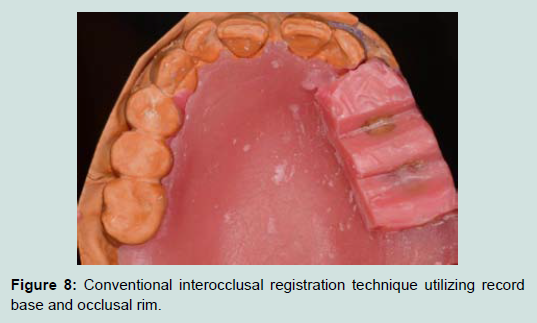
Figure 8: Conventional interocclusal registration technique utilizing record base and occlusal rim.
Temporary cylinders can be used in another technique by engaging them on a distal implant at the time of the fixture level impression (Figure 9). Injecting the bite registration material around the cylinder is used to record the bite when in maximum intercuspation, eliminating an additional patient visit. However, temporary cylinders are expensive, non-reusable and uncomfortable for the patient when adjusted in the mouth and they might not be long enough. This induces the use of excessive bite registration material which might lead to discrepancies, e.g. shrinkage in case of auto polymerizing acrylic resin.

Figure 9: Alternative interocclusal registration technique utilizing temporary cylinder and autopolymerizing acrylic resin.

Figure 10: The four maxillary Locators connected to the misangled implants.

Figure 11: Bite registration aid.
Conclusion
The advantages of the BRJ as shown in this study, present a practical and time saving method by recording the bite at the time of the impression taking procedure thus, reducing patient visits. Moreover, it provides more precision in comparison with other techniques for bite registration for distal free end implant cases, due to its anti-rotational feature, non-interference with the soft tissue, its narrow interface (platform switch design) and also it is high enough which does not necessitates large amounts of bite registration material that might cause discrepancies. In addition, 3-D printing of one hundred BRJs in two hours, at a low cost (less than one dollar), makes this technique feasible and beneficial. It can also be used with any implant system.References
- Perakis N, Belser UC, Magne P (2004) Final impressions: a review of material properties and description of a current technique. Int J Periodontics Restorative Dent 24: 109-117.
- Freilich MA, Altieri JV, Wahle JJ (1992) Principles for selecting interocclusal records for articulation of dentate and partially dentate casts. J Prosthet Dent 68: 361-367.
- Goldstein RE (2008) A precise bite registration technique. Inside Dentistry 4.
- Langer A (1981) The validity of maxillomandibular records made with trial and processed acrylic resin bases. J Prosthet Dent 45: 253-258.
- Rosenstiel SF, Land MF, Fujimoto Jc(2006) Contemporary fixed prosthodontics. In: St.Louis ( 4th edn) Mosby, pp. 62.
- Henderson D, Steffel VL (1977) Mc Craken's removable partial prosthodntics. In: St. Louis (5th edn) Mosby pp. 290-291.
- Wilhelm MW (2013) New method for improving the accuracy of bite registrations in restorative implant dentistry. Compend Contin Educ Dent 34.
- Wicks R, Ahuja S, Jain V, Ferreira CF (2013) A technique to create an interocclusal bite registration using in situ implant healing abutments. J Tenn Dent Assoc 93:47-49.