
Review Article
*Address for Correspondence: Wendy CW Wang, Implant Resident, Ashman Department of Periodontology and Implant Dentistry New York University College of Dentistry, New York, USA, Tel: 9177679166; E-mail: wcw251@nyu.edu
Citation: Wang WCW, Hafez TH, Almufleh AS, Ochoa-Durand D, Manasse M, et al. A Guideline on Provisional Restorations for Patients Undergoing Implant Treatment. J Oral Bio. 2015;2(2): 7.
Copyright © 2014 Wang et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Oral Biology | ISSN: 2377-987X | Volume: 2, Issue: 2
Submission: 17 March 2015 | Accepted: 04 May 2015 | Published: 06 May 2015

Cantilever prostheses in the anterior region have been shown to have fewer clinical complications compared to the two-retainer prostheses. The risk of debonding is reduced in the cantilever design as problems associated with rigid splinting of two abutments of differential mobility are eliminated [17,18]. Resin bonded prostheses offer a conservative option for long-term fixed provisional restorations. They can be readily applied to mandibular anterior teeth where occlusal interferences are not a factor. However, such prosthesis may not be possible in patients with deep overbite due to interference with the retainers [17].

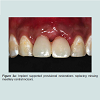
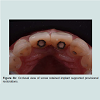
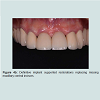
 It can be noted that the distal interdental papillae were supported by the interproximal bones of adjacent lateral incisors whereas the interdental papilla between the central incisors were formed by moving the contact points more apically (Figure 3d). Figure 3e showed the facial view of the definitive screw retained porcelain fused to metal crowns. Figure 4a and 4b demonstrated another case where the implant supported provisional restorations were used to assess the level of the ideal contact points between the two implant-supported restorations. A better papilla fill was seen in Figure 4b by shifting the contact points more apically.
It can be noted that the distal interdental papillae were supported by the interproximal bones of adjacent lateral incisors whereas the interdental papilla between the central incisors were formed by moving the contact points more apically (Figure 3d). Figure 3e showed the facial view of the definitive screw retained porcelain fused to metal crowns. Figure 4a and 4b demonstrated another case where the implant supported provisional restorations were used to assess the level of the ideal contact points between the two implant-supported restorations. A better papilla fill was seen in Figure 4b by shifting the contact points more apically.









A Guideline on Provisional Restorations for Patients Undergoing Implant Treatment
Wendy CW Wang*,Tarek H Hafez, Adi S Almufleh, Daniel Ochoa-Durand, Maryse Manasse, Stuart J Froum and Sang-Choon Cho
- Ashman Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, USA
*Address for Correspondence: Wendy CW Wang, Implant Resident, Ashman Department of Periodontology and Implant Dentistry New York University College of Dentistry, New York, USA, Tel: 9177679166; E-mail: wcw251@nyu.edu
Citation: Wang WCW, Hafez TH, Almufleh AS, Ochoa-Durand D, Manasse M, et al. A Guideline on Provisional Restorations for Patients Undergoing Implant Treatment. J Oral Bio. 2015;2(2): 7.
Copyright © 2014 Wang et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Oral Biology | ISSN: 2377-987X | Volume: 2, Issue: 2
Submission: 17 March 2015 | Accepted: 04 May 2015 | Published: 06 May 2015
Introduction
Implant therapy has been well documented to have high success rate to restore partially and fully edentulous patients [1,2]. With increased patient acceptance for implant treatment and demand for minimum disruption on the transition from natural dentition to implant supported restorations, a well-constructed provisional prosthesis that fulfills the functional, aesthetic and phonetics need is required prior to the delivery of the final restorations.An ideal provisional restoration should be strong, durable and aesthetic, and it ought not to produce excessive pressure to the underlying soft tissue, as undesirable transmucosal pressure can lead to interruption of healing at the grafted sites or implant osseointergration [3-5]. A tooth or implant supported provisional restoration is often the preferred option. It offers psychological benefit and convenience for the patient and the clinician has control over the amount of soft tissue pressure exerted. A tissue borne removable prosthesis is indicated for its lower cost or in cases where no fixed support is available but the fitting surface of the tissue borne prosthesis has to be carefully adjusted to avoid violation of healing.
Different types of provisional restorations should be considered depending on the treatment modality prescribed. For instances, treatment involving complex bone regeneration and grafting techniques requires longer uninterrupted healing time [6] and hence a provisional restoration that is durable and allows for easy modification is advantageous. On the other hand, implant placement with immediate provisionalisation [7] requires a provisional restoration that can support the peri-implant tissues. The predictability of the implant dentistry has shifted the therapy emphasis on not only the replacement of teeth but also the restoration of aesthetics. In addition to providing interim function, provisional restorations also serve as a template for the definitive restorations, and multiple sets of provisional restorations may be called for to formulate the best blue print for the definitive restorations. CAD/CAM prostheses are ideal alternatives where multiple sets of provisional prostheses are anticipated to fit the various treatment stages. The digital data acquired can be saved and modified accordingly and prostheses can be manufactured without repeated impression and inconvenience to the patients [8].
The purpose of this article is to offer a concise summary on the various provisional restorations currently used during implant therapy and provide a selection guideline based on their indications, contraindications, advantages, and disadvantages.
Types of Provisional Restorations
Provisional restorations for implant dentistry may be broadly categorized into removal and fixed provisional restorations. Removable provisional restorations are generally tooth and/or soft tissue borne whereas fixed provisional restorations are supported by adjacent teeth or implants. Provisional restorations may be used immediately following tooth extraction, during socket healing and site development, prior to implant placement and during osseointegration. Provisional restorations can also be used following implant uncovering for the purpose of soft tissue support, and aesthetics and function assessment prior to the delivery of the final restorations.
Removable Provisional Restorations
Removable partial prosthesisAn acrylic resin based removable partial prosthesis (Acrylic-RPP) is commonly prescribed as a provisional prosthesis for its fabrication simplicity, cost, and ease of insertion. The ability to modify an Acrylic-RPP to accommodate changes in ridge anatomy as a consequence of extraction, soft / hard tissue augmentation, and implant placement is also a welcome advantage. However, their bulkiness, palatal coverage and removable nature are often the cited reasons for dissatisfaction by patients. The possibilities of initiating soft tissue inflammation around gingival margins and the potential of exerting pressure to the underling surgical site are also causes of concerns for the clinicians. It is crucial that the removable prostheses should remain passive during the initial healing phase following soft/ hard tissue augmentation procedures and following implant placement as mucosal pressure could risk flap dehiscence, membrane exposure and bacterial contamination [9] whereas micro-movement may lead to fibrous encapsulation of the dental implants [10]. The creation of space between the prosthesis and the underlying tissue is sometimes necessary to minimize transmucosal pressure leading to an unsightly gap between the ridge and neck of the denture teeth.
Cobalt chromium based removable partial prosthesis (CoCr-RPP) may be designed to be supported by teeth and therefore eliminate the problems associated with the tissue borne acrylic resin based RPP. However, the additional fabrication cost and their inherent removable nature do not warrant their frequent use. However, patient’s existing CoCr-RPP may be modified to serve as the provisional prosthesis.
Vacuum-formed retainer
Vacuum-formed retainers, often referred as the Essix retainers,can be fabricated either in a commercial laboratory or in the dental office from clear thermoplastic sheets under high pressure and heat to retain pontics for missing teeth [11]. The matrix for the vacuum form is made with a pre-extraction stone cast, a duplicate cast of the diagnostic wax up of the missing teeth or a stone cast with denture teeth placed at the edentulous site. The tooth color resin is used to fill the space after the retainer is made whereas denture teeth are captured inside the vacuumed form during thermal suction. The retainers are easy and inexpensive to fabricate and they are able to protect the healing site, as they are tooth borne.
However, vacuum-formed retainers may not be appropriate for long-term use. As occlusal surface of the entire arch is covered, the retainers may interfere with speech and mastication and may be aesthetically unacceptable by some patients. Partial arch coverage is not recommended as it may lead to occlusal interference or possible supra-eruption of uncovered teeth [12]. Their durability is also limited as the thermoplastic material is vulnerable to occlusal wear and frequent replacement is often needed.
Fixed Provisional Restorations
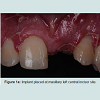
Chairside resin bonded provisional restorationA fixed provisional restoration offers psychological benefit and convenience for the patients and protects the surgical site from transmucosal pressure. Where the edentulous span is small and the provisional phase is short, bonding artificial teeth or patient’s extracted teeth to the adjacent natural teeth provide an easy and economical option. However, the bulk interproximal composite may result in unacceptable aesthetic outcome for some patients and the composite junctions are vulnerable to fracture. Mesh plates or fiber strips can be incorporated to reinforce the composite bridge and reduce the need for bulky interproximal composite [13,14]. However they are likely damaged on removal and new ones need to be constructed throughout the treatment. Figure 1a-1c demonstrated a chairside fiber reinforced composite provisional restoration. A root form titanium implant was placed and buried at maxillary left central incisor site (Figure 1a). The pontic was made of composite resin using a putty template of patient’s diagnostic wax up and secured with a fiber strip and flow able composite resin on adjacent teeth ( Figure 1b and 1c). Orthodontic brackets with an archwire are another alternative to secure pontics. It has the advantage that it can easily be detache dand replaced onto the brackets throughout the treatment. However, the presence of brackets maybe considered unsightly for some patients [15].
Laboratory made resin bonded fixed partial prosthesis
When extended healing time is anticipated, cast metal reinforced resin bonded fixed partial prosthesis (FPP) may be considered for their structural durability. They were developed as a conservative option for definitive tooth replacement, and have since become popular as provisional prostheses for implant therapy. However, optimal aesthetics may be difficult to achieve because thin or translucent teeth are often unable to mask the gray color of the palatal metal retainers.
All ceramic resin bonded FPP for missing anterior teeth may be used in selective patients when the aesthetic need is high during the provisional phase. The minimum connector dimensions, which vary according to the types of ceramics used, need to be respected to ensure sufficient rigidity and strength [16]. Although all ceramic resin bonded prostheses offer superior aesthetic potential compared to their metal base counterparts, the brittle nature of the ceramics does not permit intact removal for reuse whereas removal by mechanical tapping and recementation is possible with metal-based prostheses.
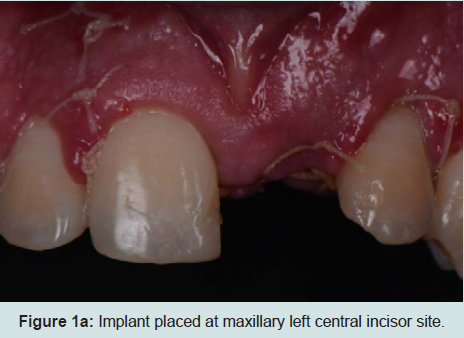
Figure 1a: Implant placed at maxillary left central incisor site.
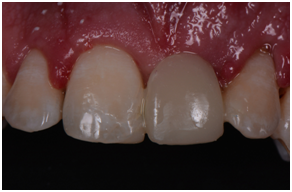
Figure 1b: Facial view of fiber reinforced composite resin provisional bridge.
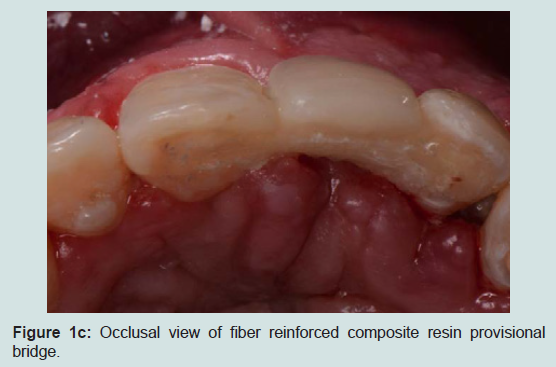
Figure 1c: Occlusal view of fiber reinforced composite resin provisional bridge.
Conventional fixed provisional restoration
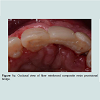
Where teeth adjacent to surgical sites are indicated for complete coverage restorations, conventional fixed provisional restorations involving tooth preparation offer a convenient and predictable option without compromising the implant site. Where multiple periodontally compromised teeth are indicated for extraction for implant placement, sequential treatment with serial extraction concept may be employed. The periodontally compromised teeth are strategically selected and prepared as abutments for provisional prostheses and the remaining periodontally compromised teeth are extracted and replaced with implants. The healing and osseointegration are protected by the fixed provisional prostheses as transmucosal pressures are eliminated. Once the implants are integrated and uncovered, the abutment teeth are extracted and replaced with more implants if indicted and the provisional prosthesis is converted to be supported by the integrated implants via relining intra-orally with auto polymerizingresin [19,20]. The serial extraction concept avoids the use of a removable prosthesis and its associated problems, however, because the extractions are staged, the treatment time is prolonged and the demand on the durability of the provisional prosthesis is increased.
In addition to elimination of harmful pressure at surgical sites, conventional provisional FPP can be mechanically retained by temporary cements; and removal for modification and reuse is relatively easy compared to the resin bonded restorations. However, the polymethylmethacrylate resin used for the fabrication of the provisional prosthesis is prone to fracture without reinforcement in long span situations. Loosening of the prosthesis, dentine sensitivity and secondary caries are some other possible complications.
Transitional implants
Provisional restorations supported by immediately loaded transitional implants (TI) offer a viable alternative to avoid any transmucosal loading in cases where a tooth supported provisional restoration is not possible [21-23]. TIs enable patients to use a provisional fixed restoration with form and function similar to those of the definitive prosthesis, at the same allows for uninterrupted healing at the implant and/or grafted site.
TIs can be placed in the edentulous sites before the ridge augmentation procedures or adjacent to the sites of the definitive implant placement. These implants are immediately loaded after a chairside reline of the interim removable partial dentures or polycarbonate crowns using auto polymerizing resin. Although these implants have been used with great success, excessive loading on TIs may result in their fracture. Moreover, placement of Tls too close to the definitive fixtures may prevent complete integration of the implant and the surrounding hard tissues [24].
Implant Supported Provisional Restoration
Following the uncovering of the implants, provisional restorations are often prescribed to support the peri-implant tissues and to assess the aesthetic outcome of the treatment thus far. The provisional restoration is used to evaluate if the future definitive restoration is in harmony with surrounding structures and to detect if any hard and soft tissues deficiency is present. The relationship between the provisional restoration and surrounding structures dictates the needs for further corrective surgeries and grafting procedures or prosthetic means to overcome the insufficiency in hard and soft tissue. Figure 2a demonstrated a case where pink acrylic was used to disguise the vertical deficiency but the aesthetic outcomes was unsatisfactory. The crown heights of the definitive restorations were subsequently lengthened to compensate for the additional space as seen in Figure 2b and further grafting procedures would be indicated to improve the aesthetic outcome.In optimal situations where no further corrective procedures are indicated, provisional restorations can shape the emergence profile of the restorations, and the matured soft tissue contour can be transferred to the definitive restorations with customized impression copings [25]. Figure 3a showed implant supported provisional restorations replacing both maxillary central incisors. The implants were placed in an ideal buccal-lingual position for screw-retained restorations (Figure 3b). The provisional restorations were modified with the addition of acrylic resins at the fitting surfaces and interproximal areas between the central incisors during the provisional phase to shape the underlying mucosa and to encourage the filling of interproximal papilla. Figure 3c demonstrated the mucosa contour shaped by the provisional restorations after 6 months of provisional phase.
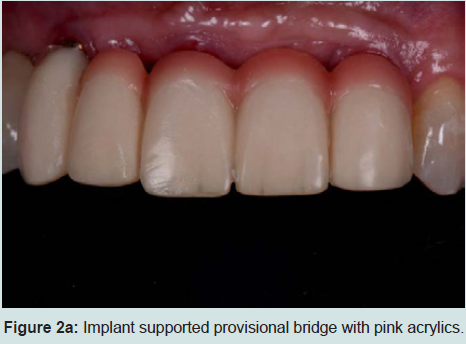
Figure 2a: Implant supported provisional bridge with pink acrylics.

Figure 2b: Implant supported definitive restorations replacing missing maxillary central and lateral incisors.
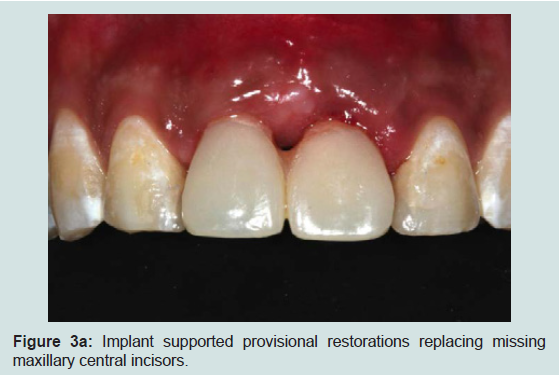
Figure 3a: Implant supported provisional restorations replacing missing maxillary central incisors.
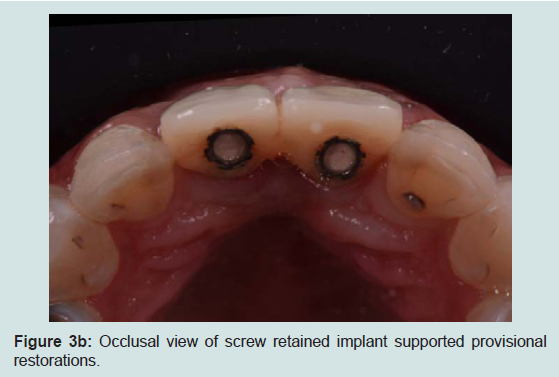
Figure 3b: Occlusal view of screw retained implant supported provisional restorations.
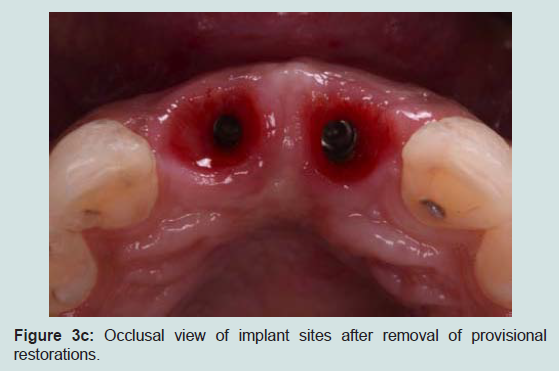
Figure 3c: Occlusal view of implant sites after removal of provisional restorations.
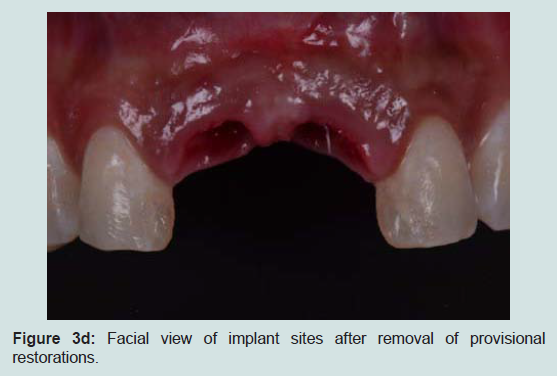
Figure 3d: Facial view of implant sites after removal of provisional restorations.
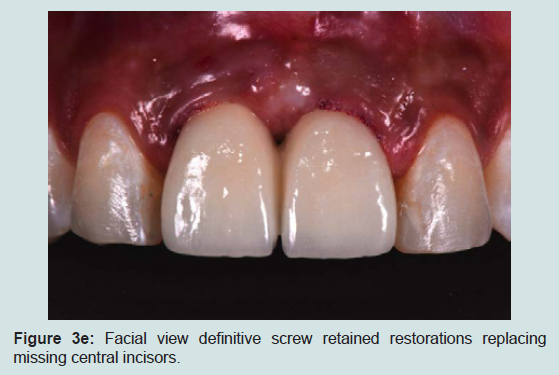
Figure 3e: Facial view definitive screw retained restorations replacing missing central incisors.
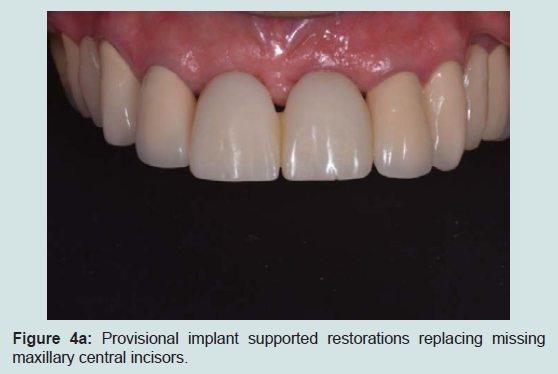
Figure 4a: Provisional implant supported restorations replacing missing maxillary central incisors.
CAD/CAM Provisional Prostheses
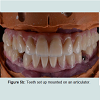
With the advance in digital dentistry, CAD/CAM (computer aided design/computer aided manufacture) is now gaining popularity for manufacturing prostheses. The construction of a CAD/CAM prosthesis starts with data acquisition involving the construction of a digital model using a dental scanner based on direct intra-oral scan or scanning an impression or a stone model of the patient. The prosthesis is designed virtually using a CAD program, which is thenrealized by processing with a milling machine, using the subtractive method or a 3-D printing machine, using the additive method [26]. Prostheses made from the subtractive method are milled from solid blocks of materials but such method has the inherent shortcomings of excessive material wastage and the impossibility of reproducing undercuts. On the other hand, the additive method, utilizing the rapid prototyping (RP) technique, does not create excessive waste as the materials used are in powder or liquid forms which are then hardened by eternal power source sand layered into the final prosthesis. The most common technologies employed for additive method in dentistry are the stereo lithography (SLA) and selective laser sintering (SLS) methods [27].CAD/CAM technology can be used for the fabrication of provisional restorations employing high-density polymers based on a highly cross-linked polymethylmetacrylate (PMMA) or composite resin. They allow for an extended provisionalisation phase as the high-density polymers used offer favorable mechanical behaviors and biocompatibility compared to the traditional indirect provisional prostheses [28]. Furthermore, the polymer-based materials enable reshaping, adding, and re-polishing procedures at chair side [29]. Another major advantage provided by the CAD/CAM technology is the ability to design and modify the pontic morphology digitally to accommodate for the changes in soft tissue architecture throughout the treatment. In addition, with the use of the dataset stored, multiple millings without the need for a new intra-oral impression are achievable. This feature allows for easy replacement of a fractured prosthesis and trying of various aesthetic designs. The customized provisional prosthesis could subsequently be scanned and digitally transferred into the definitive prosthesis for a seamless delivery. CAD/CAM fabrication can be a cost-effective alternative to a laboratory-manufactured, long-term provisional prosthesis. Figures demonstrated the utilization of CAD/CAM technology for the construction of full arch zirconia, implant supported fixed maxillary and mandibular prostheses [13-16]. Figure 5a showed the intra-oral teeth set up try-in of the full arch implant supported prostheses. Once the aesthetics, phonetics and occlusion were confirmed, the teeth set-up were placed onto the articulator and scanned for digital transfer (Figure 5b). Prototypes of the final prostheses based on the teeth set-up were subsequently milled from polymer based materials for further intra-oral reconfirmation (Figure 5c). Once all aspects of aesthetic, phonetic and occlusal needs were satisfied, the prototypes were scanned for the production of the definitive full arch zirconia prostheses. As all data were transferred digitally, errors sometimes encountered through multiple impressions and duplication processes were eliminated. The definitive prostheses were constructed to almost exact replica of the prototypes, and minimum adjustment was necessary on the day of delivery (Figure 5d).

Figure 4b: Definitive implant supported restorations replacing missing maxillary central incisors.

Figure 5a: Intra-oral teeth set up try in.
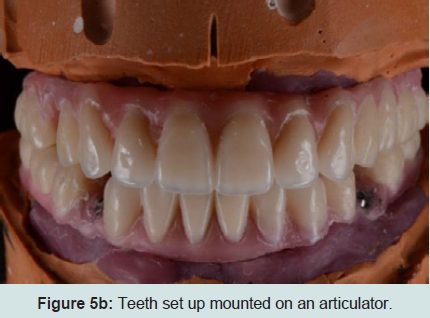
Figure 5b: Teeth set up mounted on an articulator.
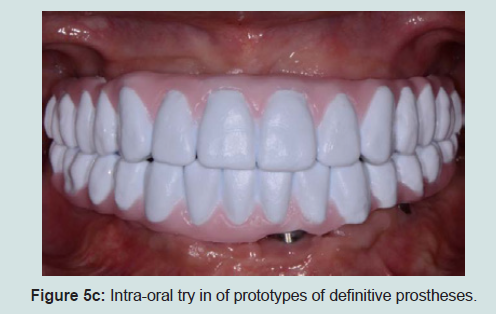
Figure 5c: Intra-oral try in of prototypes of definitive prostheses.

Figure 5d: Intra- oral view of definitive prostheses.
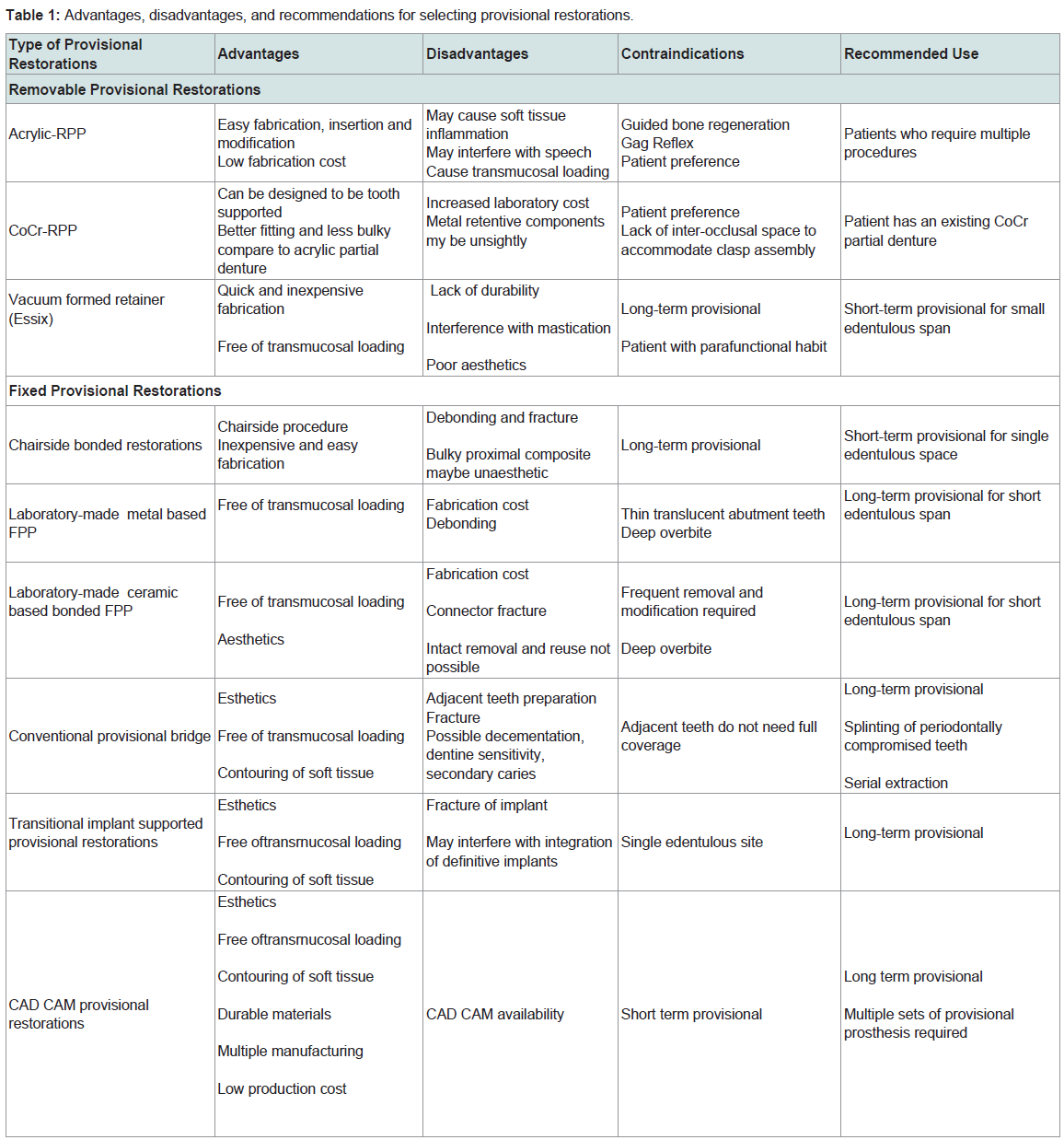
Table 1: Advantages, disadvantages, and recommendations for selecting provisional restorations.
Conclusions
The provisional treatment phase can be the most challenging aspect of implant dentistry. The options available today include removable, tooth-supported, and transitional implant-supported provisional restorations. The types of provisional restoration selected should be based on esthetic demands, functional requirements, financial considerations, duration required, and ease of fabrication. Implant supported provisional restorations play an important role in the successful outcome of the implant treatment. They are able to assess the relationships between the future definitive restorations and their surrounding hard and soft tissues, and provide crucial information on need for further surgical intervention or choices of prosthetic modalities for optima aesthetic outcome. CAD/CAM technology offers a promising provisional prosthesis fabrication alternative to conventional techniques and is now a viable and cost effective option. Distinct advantages and disadvantages (Table 1) of each provisional approach should be evaluated with respect to the specific needs of each patient (Table 2).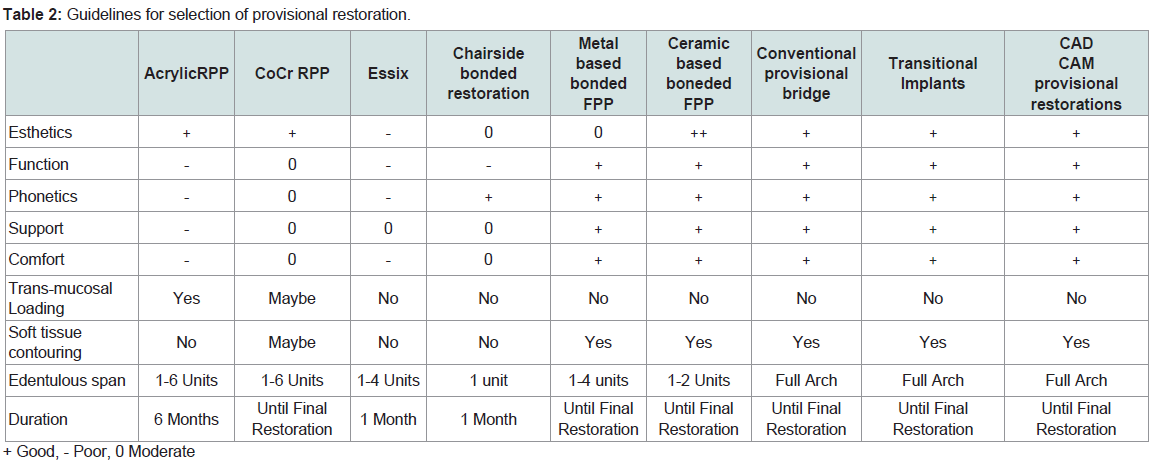
Table 2: Guidelines for selection of provisional restoration.
References
- Adell R, Lekholm U, Rockler B, Brånemark PI (1981) A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg 10: 387-416.
- Buser D, Mericske-Stern R, Bernard JP, Behneke A, Behneke N, et al. (1997) Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin Oral Implants Res 8: 161-172.
- Kan JY, Rungcharassaeng K, Kois JC (2001) Removable ovate pontic for peri-implant architecture preservation during immediate implant placement. Pract Proced Aesthet Dent 13: 711-715.
- Priest G (2006) Esthetic potential of single-implant provisional restorations: selection criteria of available alternatives. J Esthet Restor Dent 18: 326-338.
- Wang HL, Boyapati L (2006) "PASS" principles for predictable bone regeneration. Implant Dent 15: 8-17.
- Clementini M, Morlupi A, Canullo L, Agrestini C, Barlattani A (2012) Success rate of dental implants inserted in horizontal and vertical guided bone regenerated areas: a systematic review. Int J Oral Maxillofac Surg 41: 847-852.
- Wohrle PS (1998) Single-tooth replacement in the aesthetic zone with immediate provisionalization: fourteen consecutive case reports. Pract Periodontics Aesthet Den 10: 1107-1114.
- Güth JF, Almeida E Silva JS, Beuer F F, Edelhoff D (2012) Enhancing the predictability of complex rehabilitation with a removable CAD/ CAM-fabricated long-term provisional prosthesis: A clinical report. J Prosthet Dent 107: 1-6.
- Machtei EE (2001) The effect of membrane exposure on the outcome of regenerative procedures in humans: A meta-analysis. J Periodontol 72: 512-516.
- Cameron HU, Pilliar RM. MacNab I (1973) The effect of movement on the bonding of porous metal to bone. J Biomed Mater Res 7: 301-311.
- Moskowitr EM, Sheridan JJ, Celenza F Jr (1997) Essix appliances. Provisional anterior prosthesis for pre and post implant patients. N Y State Dent J 63: 32-35.
- Chate RA, Falconer DT (2011) Dental appliances with inadequate occlusal coverage: a case report. Br Dent J 210: 109-110.
- Poggio CE, Salvato A (2002) Bonded provisional restorations for esthetic soft tissue support in single- implant treatment. J Prosthet Dent 87: 688-691.
- Chafaie A, Portier R (2004) Anterior fiber-reinforced composite resin bridge: a case report. Pediatr Dent 26: 530-534.
- RE Santosa (2007) Provisional restoration options in implant dentistry. Aust Dent J 52: 234-242.
- Miettinen M, Millar BJ (2013) A review of the success and failure characteristics of resin-bonded bridges. Br Dent J 215: E3.
- Kern M, Gläser R (1997) Cantilevered all-ceramic, resin-bonded fixed partial dentures. a new treatment modality. J Esthet Dent 9: 255-264.
- Djemal S, Setchell D, King P, Wickens J (1999) Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. J Oral Rehabil 26: 302-320.
- Perel ML (1994) Progressive prosthetic transference for root form implants. Implant Dent 3: 442-446.
- Balshi TJ (1988) Converting patients with periodontally hopeless teeth to osseointegrated prostheses. Int J Periodontics Restorative Dent 8: 8-33.
- Froum S, Emtiaz S, Bloom MJ, Scolnick J, Tarnow DP (1998) The use of transitional implants for immediate fixed temporary prostheses in cases of implant restorations. Pract Periodontics Aesthet Dent 10: 737-746.
- Petrungaro PS, Smilanich MD (1999) Use of modular transitional implants in the partially edentulous patient. Contemp Esthet Restor Pract 3: 50-62.
- Petrungaro PS, Windmiller N (2001) Using transitional implants during the healing phase of implant reconstruction. Gen Dent 49: 46-51.
- Petrungaro PS (1997) Fixed temporization and bone augmented ridge stabilization with transitional implants. Pract Periodontics Aesthet Dent 9: 1071-1078.
- Priest G (2006) Esthetic potential of single-implant provisional restorations: selection criteria of available alternatives. J Esthet Restor Dent 18: 326-338.
- Strub JR, Rekow ED, Witkowski S (2006) Computer-aided design and fabrication of dental restorations: current systems and future possibilities. J Am Dent Assoc 137: 1289-1296.
- van Noort R (2012) The future of dental devices is digital. Dent Mater 28: 3-12.
- Magne P, Schlichting LH, Maia HP, Baratieri LN (2010) In vitro fatigue resistance of CAD/ CAM composite resin and ceramic posterior occlusal veneers. J Prosthet Dent 104: 149-157.
- Rocca GT, Bonnafous F, Rizcalla N, Krejci I (2010) A technique to improve the esthetic aspects of CAD/CAM composite resin restorations. J Prosthet Dent 104: 273-275.