
Journal of Oncobiomarkers
Download PDF
Research Article
*
Address for Correspondence: Hidefumi Sasaki, Department of Oncology, Immunology and Surgery, Nagoya City University Graduate School of Medical Sciences, Kawasumi, Mizuho-cho, Mizuho-ku, Nagoya 467-8601, Japan, Tel: +81-52-853-8231; Fax: +81-52-853-6440; E-mail: hisasaki@med.nagoya-cu.ac.jp
Citation: Sasaki H, Tatematsu T, Shitara M, Okuda K, Hikosaka Y, et al. Extracellular Domain Mutation of ErbB2 Status in Japanese Lung Cancer Patients. J Oncobiomarkers. 2013;1(2): 5.
Copyright © 2013 Sasaki H, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.Journal of Oncobiomarkers | ISSN: 2325-2340 | Volume: 1, Issue: 2
Submission: 11 November 2013 | Accepted: 03 December 2013 | Published: 09 December 2013
Reviewed & Approved by: Dr. John M. Varlotto, Professor, Department of Radiation Oncology, University of Massachusetts, USA
Extracellular domain of erbB2 gene mutation status in Japanese lung cancer patientsOf 210 patients, only one patient had G309E (926 guanine to adenine; Glycine to Glutamic acid). This case was male, smoker with stage I well differentiated squamous cell carcinoma. Adjacent normal lung tissue was available and the sequence result showed the wild type, suggesting that the mutation was somatic (Figure 1). The kinase domain of the erbB2 gene sequencing result showed the case was wild type. The patient had no recurrence for 48 months. No mutation at 310 amino acid position was found. In 6 erbB2 mutation cases at kinase domain, the sequences of extracellular domain were wild type.

Discussion
Extracellular Domain Mutation of ErbB2 Status in Japanese Lung Cancer Patients
Hidefumi Sasaki*, Tsutomu Tatematsu, Masayuki Shitara, Katsuhiro Okuda, Yu Hikosaka, Satoru Moriyama, Motoki Yano and Yoshitaka Fujii
- 1Department of Oncology, Immunology and Surgery, Nagoya City University Graduate School of Medical Sciences, Nagoya 467-8601, Japan
*
Address for Correspondence: Hidefumi Sasaki, Department of Oncology, Immunology and Surgery, Nagoya City University Graduate School of Medical Sciences, Kawasumi, Mizuho-cho, Mizuho-ku, Nagoya 467-8601, Japan, Tel: +81-52-853-8231; Fax: +81-52-853-6440; E-mail: hisasaki@med.nagoya-cu.ac.jp
Citation: Sasaki H, Tatematsu T, Shitara M, Okuda K, Hikosaka Y, et al. Extracellular Domain Mutation of ErbB2 Status in Japanese Lung Cancer Patients. J Oncobiomarkers. 2013;1(2): 5.
Copyright © 2013 Sasaki H, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.Journal of Oncobiomarkers | ISSN: 2325-2340 | Volume: 1, Issue: 2
Submission: 11 November 2013 | Accepted: 03 December 2013 | Published: 09 December 2013
Reviewed & Approved by: Dr. John M. Varlotto, Professor, Department of Radiation Oncology, University of Massachusetts, USA
Abstract
Purpose: The erbB pathway involves a family of tyrosine kinases and has contributed to resistance or sensitivity for chemotherapy in many tumor types. Somatic mutations of the erbB family receptor gene at kinase domain were found in lung cancer patients. However, the incidence of extracellular domain mutation of erbB2 in Japanese patients has been rarely described. We report on the incidence of these mutations and clinical factors associated with these mutations.Material and Methods: We have investigated extracellular domain mutations of erbB2 status in non-small cell lung cancer (NSCLC) patients by reverse transcript polymerase chain reaction (RT-PCR) and direct sequencing. The study included 210 surgically removed EGFR or ALK gene wild type lung cancer cases from Nagoya City University Hospital.
Results: One G309E erbB2 mutation case was found from squamous cell carcinoma. Within adenocarcinoma, no erbB2 mutation was found in extracellular domain. We have previously detected six erbB2 mutations at kinase domain all in adenocarcinomas. Among the 7 erbB2 gene mutation cases, one case with kinase domain mutation was Hercep test positive.
Conclusion: The extracellular domain mutation of erbB2 was rare in Japanese population. Although this mutation is rare, its identification could result in more precise treatment of patients.
Keywords: Extracellular domain; squamous cell carcinoma; Lung cancer; Mutations; erbB2; G309E
Introduction
ErbB family signaling pathway plays a crucial role in many carcinogenic processes such as proliferation, angiogenesis, invasion, and metastasis, and resistance to apoptosis [1,2]. Because deregulation of erbB family pathway genes has been observed frequently in various types of tumors, including non-small cell lung cancer (NSCLC), the development of targeted agents for lung cancer therapy has focused mainly on erbBs and its downstream networks [3], such as RAS/RAF/MAP kinase and PI3K/AKT being the two major pathways [3,4].The erbB family comprises 4 structurally related receptors: erbB1(EGFR), 2, 3 and 4. On ligand stimulation, the receptor forms either homodimers or heterodimers, which activate their cytoplasmic domain. Several reports have shown that somatic mutations of the EGFR gene were found in about 25-40% of Japanese NSCLC patients [5,6], but only in about 10% of NSCLC patients in USA [7,8]. EGFR mutations were predominantly found in female, non-smoker with adenocarcinomas [5-9]. Actually, EGFR mutations in NSCLC have been correlated with clinical response to gefitinib therapy [10-12]. In addition, it has been reported that erbB2 mutations at kinase domain were found in 2-4% of European-derived NSCLC patients [13,14]. The somatic erbB2 mutations were more frequent in never smoker and adenocarcinoma history [14]. The erbB2 mutation was also investigated in Japanese NSCLC [6,15,16].
The advent of next-generation sequencing technologies has enabled to compilation of large somatic mutation datasets from lung cancer sequencing studies [17]. To identify new lung cancer oncogenes, Greulich et al. [18] additionally assessed somatic alleles of significantly mutated receptor tyrosine kinase genes [17] for activity in cellular transformation assays. Although most receptor tyrosine kinase mutations tested failed to score, the extracellular domain mutations of erbB2 were oncogenic. Additional reports of extracellular domain mutations of erbB2 included G309E in 1/193 breast cancer samples and S310Y in 1/63 squamous lung cancer samples [19], S310F in 2/112 breast cancers [20], S310F in 1/65 breast cancers [21], and S310F in ovarian cancers [22]. These results indicate a unique therapeutic opportunity for patients with lung, breast and ovarian cancer who harbor extracellular domain mutations of erbB2.
Whereas the insertion mutation of the kinase domain of erbB2 is already characterized [23,24], extracellular domain mutations of erbB2 mutation frequency in Japanese NSCLC is not well known. We have previously described erbB2 mutation cases at kinase domain [6,16], however, in this study, we have additionally investigated erbB2 mutation status at extracellular domain in 210 surgically treated NSCLC cases.
Patients and Methods
PatientsThis is the retrospective study and the study group included 210 lung cancer patients who had undergone surgery at the Department of Surgery, Nagoya City University Hospital between 1997 and 2013. We have also investigated EGFR, Kras, Braf, EML4-ALK, and KIF5B/RET mutation status for the most of the same patients group. EGFR, Braf, EML4-ALK, or KIF5B/RET mutation positive samples were excluded from this study. All tumor samples were immediately frozen and stored at -80°C until assayed. The clinical and pathological characteristics of the 210 lung cancer patients are as follows; 123 cases at stage I, 38 at stage II, and 59 at stage III-IV. The mean age was 67.9 years (range, 44-86). Among the 210 lung cancer patients, 130 (61.9%) were diagnosed as adenocarcinoma, and 78 (37.1%) were squamous cell carcinoma. We have previously tested 269 patients to see if the erbB2 kinase mutation was exclusive without containing overlapping mutations (EGFR, Braf, EML4-ALK, or KIF5B/RET) [16]. Of 269, 102 samples were overlapped with this study.
PCR assays for erbB2
Total RNA was extracted from lung cancer tissues and adjacent non-malignant lung tissues using Isogen kit (Nippon gene, Tokyo, Japan) according to the manufacturer’s instructions. RNA concentration was determined by spectrophotometer and adjusted to a concentration of 200 ng/ml. About 20 cases were excluded because tumor cells were too few to sufficiently extract tumor RNA. RNA (1μg) was reverse transcribed by Superscript II enzyme (Gibco BRL, Gaithersburg, MD) with 0.5 μg oligo (dT)12-16 (Amersham Pharmacia Biotech Inc. Piscataway, NJ) . The reaction mixture was incubated at 42°C for 50 minutes and then at 72°C for 15 minutes. We then used 1 μl of each DNA for PCR analyses. The PCR reactions were performed using LA-Taq kit (Takara Bio Inc, Shiga, Japan) in a 50- μl reaction volume. The primer sequences for erbB2 gene for extracellular domain (779-1070, 292bp) were as follows: the forward primer, 5-ACAGTGGCATCTGTGAGCTG-3 and the reverse primer, 5-GTAACTGCCCTCACCTCTCG-3. The cycling conditions were as follows: initial denaturation at 94°C for 5 minutes, followed by 40 cycles at 94°C for 45 seconds, 60°C for 45 seconds, 72°C for 30 seconds. The primer sequences for erbB2 gene for kinase domain (exon 19-22) were as follows: the forward primer, 5-CGCTTTTGGCACAGTCTACA -3 and the reverse primer, 5-GGGATCCCATCGTAAGGTTT -3 (594bp). The cycling conditions were as follows: initial denaturation at 94°C for 5 minutes, followed by 35 cycles at 94°C for 40 seconds, 60°C for 40 seconds, 72°C for 45 seconds. The products were purified by Qiagen PCR purification kit (Qiagen, Valencia, CA). Amplified cDNAs were separated on 1% agarose gels, and the bands were visualized by ethidium bromide and photographed under ultraviolet transillumination. These samples were sequenced by ABI prism 3100 analyzer (Applied Biosystems Japan Ltd., Tokyo, Japan) and analyzed by BLAST and chromatograms by manual review form forward and reverse, both side. EGFR, Kras and Braf sequencing methods were already submitted elsewhere [5,6,9,16,25].
ErbB2 Immunohistochemistry
7 cases were immunostained by methods for HercepTest II (Dako Japan Co., Tokyo, Japan) using the rabbit polyclonal antibody against HER2/neu. Unstained 4-μm sections of FFPE tumor tissue were submitted to the analysis. The Dako HercepTestTM, system included pretreatment with Target Retrieval solution, pH 6 (Dako Co.) 97°C for 40 minutes, followed by incubation with rabbit polyclonal anti-HER2/neu at room temperature for 30 minutes. Antibody incubation was followed by standard signal amplification including HRP conjugated polymer solution at room temperature for 30 minutes, DAB reaction for 10 minutes and counter staining with hematoxylin for 3 minutes. An IHC score was assigned to each case according to the following criteria showing the designated staining pattern; 3+, intense staining; 2+, moderately staining; 1+, faint staining at membrane; and no staining. Tumors with intensity involving a minimum of 10% of the positive stained tumor cells were considered positive for erbB2 expression.Statistical analysis
Statistical analyses were done using the Mann- Whitney U-test for unpaired samples. Correlation coefficients were determined by rank correlation using Spearman’s test and χ2test. All analysis was done using the Stat-View software package (Abacus Concepts Inc. Berkeley, CA, USA), and was considered significant when the p -value was less than 0.05.
Results
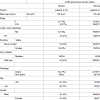
ErbB2 gene mutation status in Japanese lung cancer patientsWe have previously sequenced kinase domain of erbB2 for 269 NSCLC patients [16]. Among 269 patients, 5 patients (2.0%) had erbB2 mutations. All mutations were at exon 20. Three were female. All were non-smoker. Four had 12 amino acids insertion mutation (2324-2325 ins ATACGTGATGGC), located in the exon 20 at kinase domain (775-776 ins YVMA). One had amino acids insertion mutation (2326 G to TTGT), located in the exon 20 at kinase domain (776 Glycine to Leucine plus Cystein). We have additionally sequenced 17 samples, and one had ins YVMA. This case was male, smoker with adenocarcinoma. Totally, never smoker had significantly higher erbB2 mutation rate than in smoker (p=0.0328). There was no significant difference of erbB2 mutation rate in gender(p=0.4202), age (p=0.6849) and pathological stages (p=0.6803) (Table 1). All 6 are survived, however, 3 of them had relapsed and underwent conventional chemothepary.Within these NSCLC, five genes (EGFR, erbB2, Kras, Braf and KIF5B/RET) mutations were exclusively existed. Only one patient had EGFR and EML4/ALK mutations (data not shown). In the same period, 232 had EGFR mutations within kinase domain, including 107 exon19 deletions and 102 L858R mutations. 7 had ALK translocations and 3 had KIF5B/RET translocations. 7 Braf mutations were within kinase domain (data not shown).
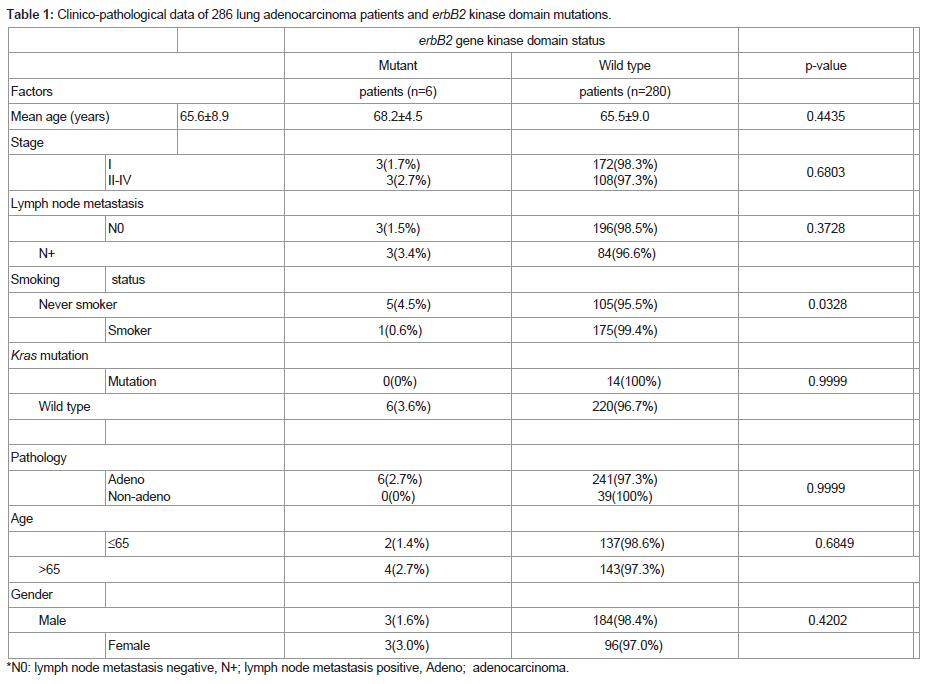
Table 1: IFA and IHC Staining for KSHV LANA and Tropoelastin in Sarcomas of the mECK model for KSHV Induced KS.
Figure 1: G309E (926 guanine to adenine; Glycine to Glutamic acid) mutation at extracellular domain of erbB2. Adjacent normal lung tissue was available and the sequence result showed the wild type, suggesting that the mutation was somatic.
Immunohistochemistry
An immunohistochemical approach, Hercep Test was used to study erbB2 protein expression in 7 NSCLC cases, including 6 mutants at kinase domain and one mutant at extracellular domain. One erbB2 ins YVMA mutant adenocarcinoma showed more than 10% membrane signal with 1+ (Figure 2). In addition, another ins YVMA case had the 1+ staining intensity, less than 10% of tumors. In other cases, including extracellular domain mutant case, there were no-stained.]
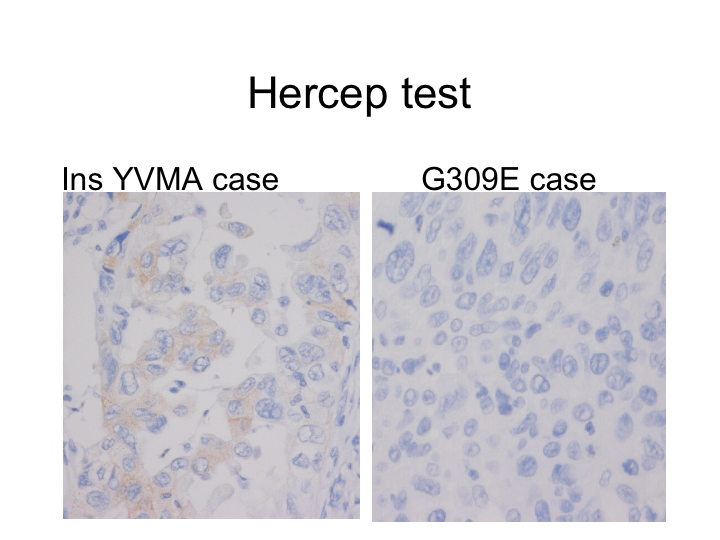
Figure 2: Hercep test results for erbB2 mutant case at kinase domain (775-776 ins YVMA) (left) and at extracellular domain (right).
Discussion
In this study, we found that an extracellular domain mutation of erbB2 case out of 210 NSCLC. The erbB2 mutation was exclusively found without erbB2 mutation at kinase domain. Extracellular domain mutation of erbB2 was found in squamous cell carcinomas but not in adenocarcinoma. On the other hands, in our analysis, erbB2 genes mutations at kinase domain were predominantly found in non-smoker with adenocarcinomas.
The recurrent mutated erbB2 residue 309-310 lies in domain II of the extracellular region has considered to mediate receptor dimerization [26]. Furthermore, residue S310 is involved in interactions with a therapeutic antibody that prevents erbB2 dimerization [27]. Hence the recurrent mutation of this site probably alters the function of erbB2. ErbB2 mutations have reported in breast cancers, with two being identical S310F mutations [20]. These two samples were distinct on the basis of their germline and somatic genotypes [20], suggested the mutation was somatic. Neither sample with the S310F activating mutation had erbB2 amplification. This is consistent with our results showing Hercep-test negative for our G309E sample. However, the two mutant breast cancer samples belong to the erbB2-enriched and luminal B subtypes, which typically have erbB2 amplification, indicated the observed mutations have a driving role in these tumors. The G309E, S310F and S310Y mutants over expressed NIH 3T3 cells supported robust colony formation in soft agar [18]. AALE human lung epithelial cells were similarly transformed to anchorage independence by the extracellular mutants of erbB2 [18]. These mutants have two distinct mechanisms: elevation of C-terminal phosphorylation and formation of disulfide-linked dimmers [18]. Whereas only a slight increase in phosphopeptide ratio was seen in the erbB2 G309E-expressing cells over wild type, the cells expressing erbB2 S310F exhibited a more substantial increase in peptide phosphorylation [18]. Ba/F3 cells transformed with the erbB2 extracellular domain mutants had effective results using the irreversible erbB2 inhibitor neratinib and afatinib [18], however the sensitivity was lower than ins YVMA cells. The reversible inhibitor afatinib had sensitive effect for the lung cancer cell line NCI-H1781, haboring an erbB2 kinase domain mutation [28]. A combination of erbB2 inhibition and Mek inhibition was necessary for abrogation of 5637 bladder cancer cell line, haboring an erbB2 S310F mutation [18,29].
Mutations in erbB2 gene were found in approximately 2% of primary non-small cell lung cancers, dominantly in never smoker like EGFR mutations [4-9]. It has shown that the common erbB2 mutation, A775insYVMA, lead to oncogenic transformation in a cellular assay [23]. Because one co-existed case with erbB2 and Kras mutation was reported [30], we have also examined the Kras mutant cases. However, in our cohort, Kras and erbB2 mutations were exclusive. The mutant cells [28] and patients [31] exhibited exquisite sensitivity to the irreversible dual-specificity EGFR/ERBB2 kinase inhibitor BIBW2992, afatinib. Trastuzumab-besed therapies effective cases were previously reported [30]. However in our cohort, only one case had Hercep Test 1+. Usually in breast cancer, 2+ or 3+ cases were administered with trastuzumab, and it may not useful for our patients.
In our analysis, extracellular domain mutation of erbB2 was only found from squamous cell carcinoma but not from adenocarcinoma. In contrast, erbB2 mutations at kinase domain were found only in 6/279 adenocarcinomas dominantly in never smokers. Our data showed that mutations of erbB2 gene as a mechanism of tumorigenesis is unlikely to be associated with many of Japanese NSCLC. Despite the promise of irreversible erbB inhibitors, our findings indicated that a small percentage of NSCLC actually harbor erbB2 mutations and, in turn that a few patients with these tumors likely benefit from these anticancer agents. However, completely exclusive EGFR, erbB2, Kras and Braf mutation status would help us to choose order-made molecular target therapy for NSCLC. Further studies are needed to confirm the mechanisms of erbB2 mutations for the sensitivity or resistance of targeted therapy for the lung cancer. Now that in 2013, afatinib has been approved for lung cancer treatment in USA [32].
Acknowledgements
This work was supported by Grants-in-Aid for Scientific Research, Japan Society for the Promotion of Science (JSPS) (Nos, 23659674, 24592097, 25293303). We would like to thank Mr. Yoichi Tani and Miss Ito Yamamoto for their excellent technical assistances.References
- Yarden Y, Sliwkowski MX (2001) Untangling the ErbB signaling network. Nat Rev Mol Cell Biol 2: 127-137.
- Rowinsky EK (2004) The erbB family: targets for therapeutic development against cancer and therapeutic strategies using monoclonal antibodies and tyrosine kinase inhibitors. Annu Rev Med 55: 433-457.
- Wieduwilt MJ, Moasser MM (2008) The epidermal growth factor receptor family: biology driving targeted therapeutics. Cell Mol Life Sci 65: 1566-1584.
- Laurent-Puig P, Lievre A, Blons H (2009) Mutations and response to epidermal growth factor receptor inhibitors. Clin Cancer Res 15: 1133-1139.
- Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, et al. (2004) EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science 304: 1497-1500.
- Sasaki H, Shimizu S, Endo K, Takada M, Kawahara M, et al. (2006) EGFR and erbB2 mutation status in Japanese lung cancer patients. Int J Cancer 118: 180-184.
- Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, et al. (2004) Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med 350: 2129-2139.
- Pao W, Miller V, Zakowski M, Doherty J, Politi K, et al. (2004) EGF receptor gene mutations are common in lung cancers from ‘never smokers’’ and are associated with sensitivity of tumors to gefitinib and elrotinib. Proc Natl Acad Sci 101: 13306-13311.
- Sasaki H, Endo K, Konishi A, Takada M, Kawahara M, et al. (2005) EGFR mutation status in Japanese lung cancer patients: genotyping analysis using LightCycler. Clin Cancer Res 11: 2924-2929./a>
- Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, et al. (2009) Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. New Eng J Med 361: 947-957.
- Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, et al. (2010) Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer habouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomized phase 3 trial. Lancet Oncol 11: 121-128..
- Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, et al. (2010) Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med 362: 2380-2388.
- Stephens P, Hunter C, Bignell G, Edkins S, Davies H, et al. (2004) Lung cancer: Intragenic erbB2 kinase mutations in tumors. Nature 431: 525-526.
- Shigematsu H, Takahashi T, Nomura M, Majmudar K, Suzuki M, et al. (2005) Somatic mutations of the HER2 kinase domain in lung adenocarcinomas. Cancer Res 65: 1642-1646.
- Tomizawa K, Suda K, Onozato R, Kosaka T, Endoh H, et al. (2011) Prognostic and predictive implications of HER2/ERBB2/neu gene mutations in lung cancers. Lung Cancer 74: 139-144.
- Sasaki H, Shitara M, Yokota K, Okuda K, Hikosaka Y, et al. (2012) Braf and erbB2 mutations correlate with smoking status in lung cancer patients. Exp Ther Med 3: 771-775.
- Ding K, Getz G, Wheeler DA, Mardis ER, McLellan MD, et al. (2008) Somatic mutations affect key pathways in lung adenocarcinoma. Nature 455: 1069-1075.
- Greulich H, Kaplan B, Mertins P, Chen TH, Tanaka KE, et al. (2012) Functional analysis of receptor tyrosine kinase mutations in lung cancer identifies oncogenic extracellular domain mutations of erbB2. PNAS 109: 14476-14481.
- Kan Z, Jaiswal BS, Stinson J, Janakiraman V, Bhatt D, et al. (2010) Diverse somatic mutation patterns and pathway alterations in human cancers. Nature 466: 869-873.
- Banerji S, Cibulskis K, Rangel-Escareno C, Brown KK, Carter SL, et al. (2012) Sequence analysis of mutations and translocations across breast cancer subtypes. Nature 486: 405-409.
- Shah SP, Roth A, Goya R, Oloumi A, Ha G, et al. (2012) The clonal and mutational evolution spectrum of primary triple-negative breast cancers. Nature 486: 395-399.
- Cancer Genome Atlas Research Network (2011) Integrated genomic analyses of ovarian carcinoma. Nature 474: 609-615./a>
- Minami Y, Shimamura T, Shah K, LaFramboise T, Glatt KA, et al. (2007) The major lung cancer-derived mutants of ERBB2 are oncogenic and are associated with sensitivity to the irreversible EGFR/ERBB2 inhibitor HKI-272. Oncogene 26: 5023-5027.
- Wang SE, Narasanna A, Perez-Torres M, Xiang B, Wu FY, et al. (2006) HER2 kinase domain mutation results in constitutive phopsholylation and activation oh HER2 and EGFR and resistance to EGFR tyrosine kinase inhibitors. Cancer Cell 10: 25-38.
- Sasaki H, Hikosaka Y, Kawano O, Moriyama S, Yano M, et al. (2011) Evaluation of Kras mutation and copy number gain in non-small cell lung cancer. J Thorac Oncol 6: 15-20.
- Burgess AW, Cho HS, Eigenbrot C, Ferguson KM, Garrett TP, et al. (2003) An open-and-shut case? Recent insights into the activation of EGF/ErbB receptors. Mol Cell 12: 541-552.
- Franklin MC, Carey KD, Vajdos FF, Leahy DJ, De Vos AM, et al. (2004) Insights into ErbB signaling from the structure of the ErbB2-pertuzumab complex. Cancer Cell 5: 317-328.
- Li D, Ambrogio L, Shimamura, T, Kubo S, Takahashi M, et al. (2008) BIBW2992, an irreversible EGFR/HER2 inhibitor highly effective in preclinical lung cancer models. Oncogene 27: 4702-4711.
- Barretina J, Caponigro G, Stransky N, Venkatesan K, Margolin AA, et al. (2012) The cancer cell line encyclopedia enables predictive modeling of anticancer drug sensitivity. Nature 483: 603-607.
- De Greve J, Teugels E, Geers C, Decoster L, Galdermans D, et al. (2012) Clinical activity of afatinib (BIBW2992) in patients with lung adenocarcinoma with mutations in the kinase domain of HER2/neu. Lung Cancer 76: 123-127.
- Mazieres J, Peters S, Lepage B, Cortot AB, Barlesi F, et al. (2013) Lung cancer that habors an HER2 mutation: epidemiologic characteristics and therapeutic prospectives. J Clin Oncol 31: 1997-2003.
- Sequist LV, Yang JCH, Yamamoto N, O’Byrne K, Hirsh V, et al. (2013) Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with epidermal growth factor receptor mutations. J Clin Oncol 31: 3327-3334.