
Journal of Obesity and Bariatrics
Download PDF
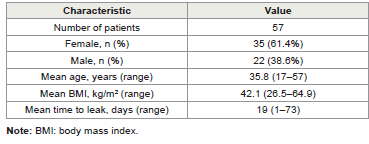 Table I-A: Baseline demographics (n=57)
Table I-A: Baseline demographics (n=57)
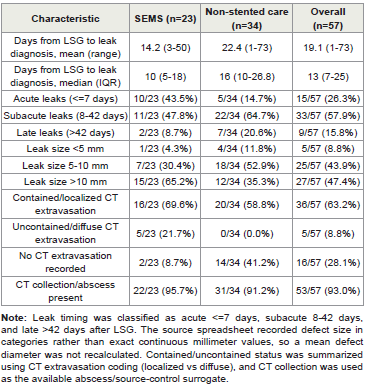 Table I-B: Baseline leak characteristics by index strategy
Table I-B: Baseline leak characteristics by index strategy
 Table II: Outcomes by index strategy and E-VAC rescue outcomes
Table II: Outcomes by index strategy and E-VAC rescue outcomes
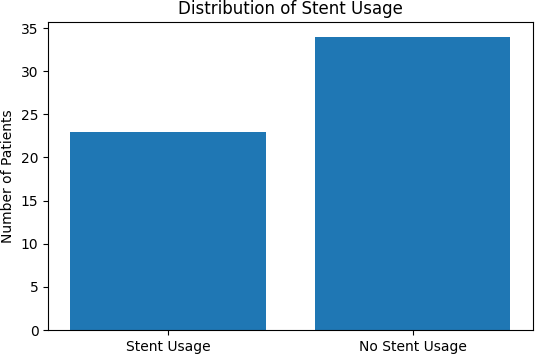 Figure 1: Distribution of index strategy (SEMS ± fixation vs non-stented care)
in the study cohort (n=57).
Figure 1: Distribution of index strategy (SEMS ± fixation vs non-stented care)
in the study cohort (n=57).
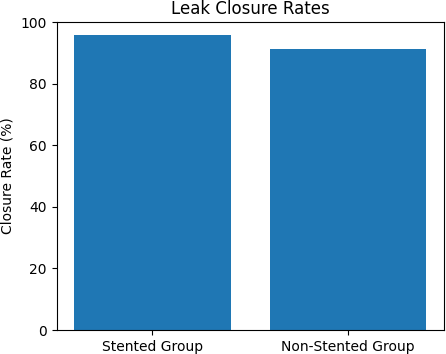 Figure 2: Leak closure rates by index strategy.
Figure 2: Leak closure rates by index strategy.
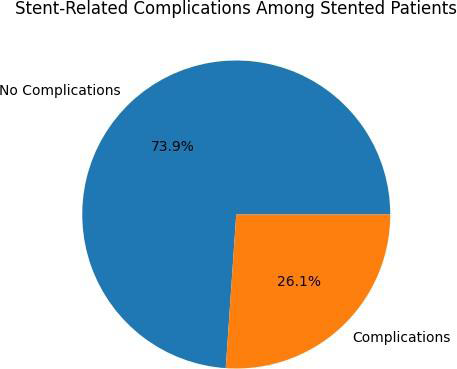 Figure 3: Stent-related adverse events among SEMS patients (n=23).
Figure 3: Stent-related adverse events among SEMS patients (n=23).
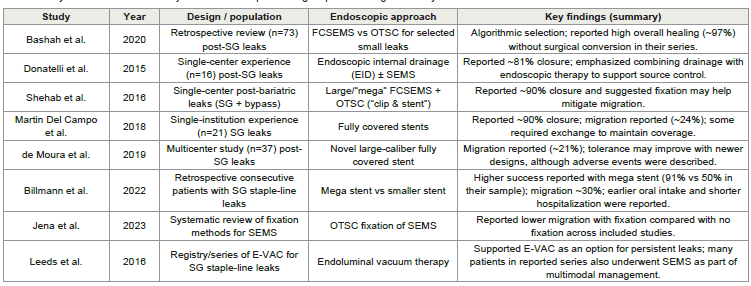 Table III: Key studies from the last 10 years on endoscopic stenting for post-sleeve gastrectomy leaks
Table III: Key studies from the last 10 years on endoscopic stenting for post-sleeve gastrectomy leaks
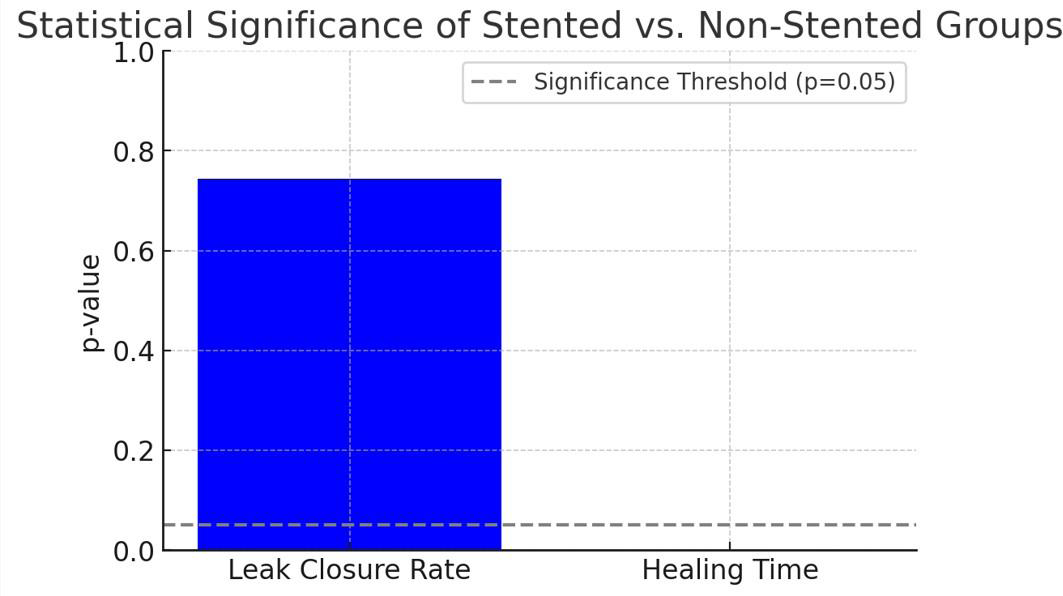 Figure 4: Bar chart illustrating the statistical significance (p-values) for the
comparison between stented and non-stented cohorts:
• Leak Closure Rate: Not statistically significant (p = 0.743, blue bar).
• Healing Time: Statistically significant (p < 0.001, red bar).
The dashed line at p = 0.05 indicates the conventional threshold for statistical
significance.
Figure 4: Bar chart illustrating the statistical significance (p-values) for the
comparison between stented and non-stented cohorts:
• Leak Closure Rate: Not statistically significant (p = 0.743, blue bar).
• Healing Time: Statistically significant (p < 0.001, red bar).
The dashed line at p = 0.05 indicates the conventional threshold for statistical
significance.
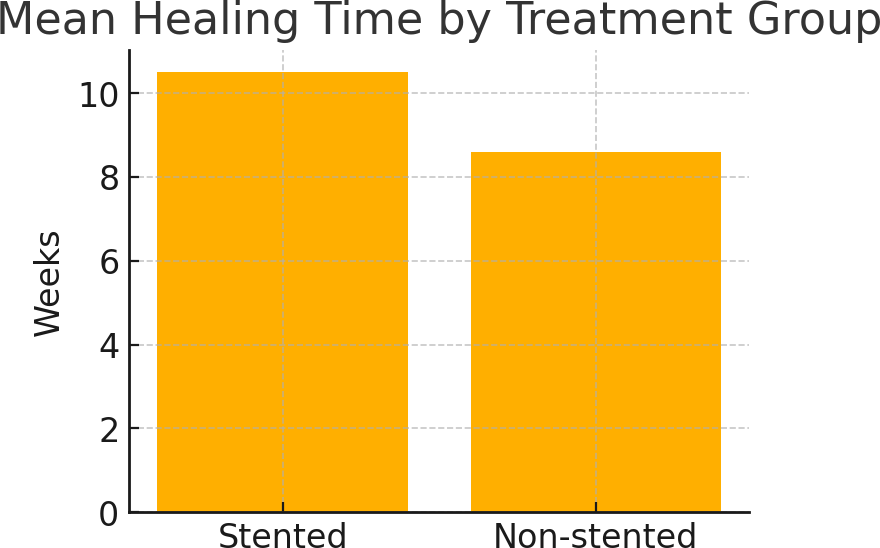 Figure 5: Mean Healing Time by Treatment Group
Figure 5: Mean Healing Time by Treatment Group
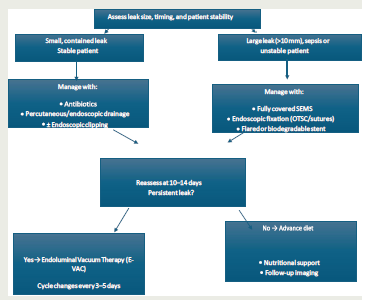 Figure 6: Goal-Oriented Algorithm for Post-Sleeve Leak Management
Figure 6: Goal-Oriented Algorithm for Post-Sleeve Leak Management
Research Article
Endoscopic Management of Sleeve Gastrectomy Leaks: Outcomes of SEMS and Non-Stented Strategies in a Single Tertiary Center
Nesreen K1, El Matbouly M2*, Bashah M1 and AL-Kuwari M1
1Bariatric and Metabolic Center, Hamad Medical Corporation,
Doha, Qatar
2Department of Surgery, Hamad Medical Corporation, Doha, Qatar
2Department of Surgery, Hamad Medical Corporation, Doha, Qatar
*Address for Correspondence:Moamena El Matbouly, Department of Surgery, Hamad Medical
Corporation Ahmed Bin Alit Street, P.O. Box 3050, Doha, Qatar. E-mail Id: momenaelmatbouly@gmail.com
Submission: 25 May, 2026
Accepted: 13 June, 2026
Published: 16 June, 2026
Copyright: © 2026 Nesreen K, et al. This is an open access
article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is
properly cited.
Keywords: Gastrectomy, Sleeve; Anastomotic Leak; Endoscopy; Stents; Negative-
Pressure Wound Therapy; Bariatric Surgery
Abstract
Background:Staple-line leaks following laparoscopic sleeve gastrectomy (LSG)
cause substantial morbidity. Endoscopic options include self-expandable metal stents
(SEMS), drainage with or without endoscopic closure, and endoluminal vacuum therapy
(E‑VAC).
Methods:We performed a retrospective cohort study of adults with imaging confirmed post-LSG leaks treated at a tertiary bariatric center (2018–2023). Index management was SEMS (± fixation) or non-stented care (antibiotics, percutaneous/ endoscopic drainage, ± endoscopic closure). E‑VAC was reserved as rescue after stent removal or failure of non-stented therapy. Primary outcomes were leak closure and time to healing.
Results:Fifty-seven patients were included; 23 received SEMS and 34 received non-stented care. Overall leak resolution occurred in 53/57 (93.0%). Closure was achieved in 22/23 SEMS patients (95.7%) and 31/34 non-stented patients (91.2%). Mean time to healing was 10.5 weeks in the SEMS group and 8.6 weeks in the nonstented group. Stent-related adverse events occurred in 6/23 (26.1%) SEMS patients and were managed with repositioning, exchange, or planned removal. E-VAC rescue therapy was used in 9 patients; all achieved leak closure (9/9, 100%), with closure documented over 4-8 weeks (mean 5.7 weeks; median 5 weeks).
Conclusions:Both SEMS-based and non-stented strategies achieved high closure in selected patients. We propose a pragmatic, goal-oriented pathway that aligns initial therapy with leak complexity and reserves E‑VAC strictly as rescue; prospective validation is needed.
Methods:We performed a retrospective cohort study of adults with imaging confirmed post-LSG leaks treated at a tertiary bariatric center (2018–2023). Index management was SEMS (± fixation) or non-stented care (antibiotics, percutaneous/ endoscopic drainage, ± endoscopic closure). E‑VAC was reserved as rescue after stent removal or failure of non-stented therapy. Primary outcomes were leak closure and time to healing.
Results:Fifty-seven patients were included; 23 received SEMS and 34 received non-stented care. Overall leak resolution occurred in 53/57 (93.0%). Closure was achieved in 22/23 SEMS patients (95.7%) and 31/34 non-stented patients (91.2%). Mean time to healing was 10.5 weeks in the SEMS group and 8.6 weeks in the nonstented group. Stent-related adverse events occurred in 6/23 (26.1%) SEMS patients and were managed with repositioning, exchange, or planned removal. E-VAC rescue therapy was used in 9 patients; all achieved leak closure (9/9, 100%), with closure documented over 4-8 weeks (mean 5.7 weeks; median 5 weeks).
Conclusions:Both SEMS-based and non-stented strategies achieved high closure in selected patients. We propose a pragmatic, goal-oriented pathway that aligns initial therapy with leak complexity and reserves E‑VAC strictly as rescue; prospective validation is needed.
Abbreviations
FCSEMS = fully covered self-expandable metal stent; OTSC =
over-the-scope clip; SG = sleeve gastrectomy; E‑VAC = endoluminal
vacuum therapy.
Introduction
Laparoscopic sleeve gastrectomy (LSG) is among the most
performed bariatric operations worldwide. Despite technical
refinements, staple‑line leaks occur in ~1-3% and drive much of
the morbidity, readmission, and cost after LSG [1-3]. Historically,
management spanned conservative measures (antibiotics and
percutaneous drainage) and early reoperation; however, neither
approach reliably balances efficacy with patient comfort and organ
preservation [4].
Over the last decade, endoscopy has redefined the treatment landscape. Fully covered self‑expandable metal stents (SEMS) routinely achieve closure in >85-90% of post‑LSG leaks, but migration and intolerance have limited durable success, particularly when dwell times are short or fixation is absent [8–13,15]. Newer techniques— including over‑the‑scope clip (OTSC) or endoscopic suturing fixation—appear to reduce migration to single‑digit percentages and enhance dwell stability [13,15,17]. Parallel to stenting, endoluminal vacuum therapy (E‑VAC) has emerged as an effective rescue strategy for chronic or complex defects and can facilitate granulation and source control in anatomies where stenting is suboptimal [16]. Yet, despite these advances, no broadly accepted, data‑driven algorithm dictates the initial endoscopic choice; leak timing (acute vs subacute vs late), size/containment, patient stability, and local expertise all plausibly influence outcomes [5–7,12,14,16].
Over the last decade, endoscopy has redefined the treatment landscape. Fully covered self‑expandable metal stents (SEMS) routinely achieve closure in >85-90% of post‑LSG leaks, but migration and intolerance have limited durable success, particularly when dwell times are short or fixation is absent [8–13,15]. Newer techniques— including over‑the‑scope clip (OTSC) or endoscopic suturing fixation—appear to reduce migration to single‑digit percentages and enhance dwell stability [13,15,17]. Parallel to stenting, endoluminal vacuum therapy (E‑VAC) has emerged as an effective rescue strategy for chronic or complex defects and can facilitate granulation and source control in anatomies where stenting is suboptimal [16]. Yet, despite these advances, no broadly accepted, data‑driven algorithm dictates the initial endoscopic choice; leak timing (acute vs subacute vs late), size/containment, patient stability, and local expertise all plausibly influence outcomes [5–7,12,14,16].
We report a single-center cohort of 57 post-LSG leaks managed
between 2018 and 2023 using two index strategies—SEMS (±
fixation) versus non-stented care (drainage ± endoscopic closure)—
with E-VAC reserved as a rescue measure after stent removal or failed
non-stented therapy. We aimed to: (1) describe patient/leak features
and real‑world outcomes for each strategy; (2) contextualize healing
trajectories and complications relative to contemporary literature;
and (3) present a pragmatic, goal‑oriented pathway that aligns initial
therapy with case complexity while explicitly acknowledging the
limits of retrospective inference [5,10,12,15–17]. This manuscript
builds upon—and explicitly distinguishes itself from—our earlier
experience by integrating standardized fixation practices, transparent
reporting of non-stented pathways, and an embedded statistical
analysis plan. More importantly, all cases were managed at a single
tertiary hospital by one coordinated endoscopy–surgery team,
minimizing practice variation and ensuring a consistent protocol
across the cohort.
Materials and Methods
The study was conducted in accordance with the Helsinki
Declaration as revised in 2024. For this retrospective chart review,
the requirement for informed consent was waived by the approving
board.Ethical approval for this retrospective chart review was
obtained from the Institutional Review Board (IRB No. 16208/16),
and the requirement for informed consent was waived by the
approving board.
Design and Oversight:Consent was waived for retrospective
chart review. Reporting adheres to STROBE guidelines and includes
a prespecified Statistical Analysis Plan (SAP).
Setting and case identification:Consecutive patients were
identified through institutional surgical and endoscopy databases and
cross-referenced with imaging reports. A post-LSG leak was defined
by contrast extravasation on upper gastrointestinal swallow study or
contrast-enhanced computed tomography, and/or direct endoscopic
visualization of a defect with associated collection. Leak timing was
classified as acute, subacute, or late according to the prespecified
statistical analysis plan; for transparency we defined acute as ≤7 days,
subacute as 8–42 days, and late as >42 days after index surgery.
Population:Consecutive adults with post‑LSG staple‑line leaks confirmed by contrast swallow or contrast‑enhanced CT operated in major tertiary center from 2018-2023.
Supportive care:Across both pathways, patients received protocolized sepsis management and nutrition support. Source control was pursued through percutaneous or endoscopic drainage when a collection was present. Nutritional optimization (enteral feeding distal to the leak when feasible, or parenteral nutrition when necessary) was coordinated with bariatric surgery, nutrition, and interventional radiology teams.
Population:Consecutive adults with post‑LSG staple‑line leaks confirmed by contrast swallow or contrast‑enhanced CT operated in major tertiary center from 2018-2023.
Supportive care:Across both pathways, patients received protocolized sepsis management and nutrition support. Source control was pursued through percutaneous or endoscopic drainage when a collection was present. Nutritional optimization (enteral feeding distal to the leak when feasible, or parenteral nutrition when necessary) was coordinated with bariatric surgery, nutrition, and interventional radiology teams.
Index Strategies:SEMS group—Fully covered SEMS with or
without anti‑migration fixation (OTSC or endoscopic suturing).
Planned dwell 4–6 weeks with reassessment at removal. Non‑stented
group—Antibiotics, percutaneous or endoscopic drainage, and/
or direct endoscopic closure (e.g., OTSC or endoscopic clipping).
Rescue therapy: E‑VAC is reserved for persistent leaks after stent
removal or failure of non‑stented therapy. E‑VAC was not performed
with a stent in situ.
SEMS pathway details:The SEMS strategy aimed to exclude gastric contents from the leak and restore luminal continuity. Fixation (over-the-scope clip or endoscopic suturing) was used when feasible to reduce migration risk, particularly in proximal leaks and when longer dwell times were planned. Stent dwell was typically 4–6 weeks, with earlier intervention reserved for clinical deterioration, intolerance, or device migration.
SEMS pathway details:The SEMS strategy aimed to exclude gastric contents from the leak and restore luminal continuity. Fixation (over-the-scope clip or endoscopic suturing) was used when feasible to reduce migration risk, particularly in proximal leaks and when longer dwell times were planned. Stent dwell was typically 4–6 weeks, with earlier intervention reserved for clinical deterioration, intolerance, or device migration.
Non-stented pathway details:Non-stented management
prioritized drainage, antimicrobial therapy, and selective endoscopic
closure for small, contained defects in stable patients. Endoscopic
closure options included through-the-scope clipping or OTSC
for focal defects when local conditions were favorable (minimal
inflammation, adequate drainage, and no large uncontained cavity).
Outcomes:Primary—leak closure (clinical/radiologic) and time‑to‑healing (weeks from index endoscopy to closure). Secondary—adverse events (AEs), stent migration, reinterventions, nutrition support, and length of stay.
Outcome definitions:Leak closure required clinical resolution with radiologic confirmation (no contrast extravasation) and/or endoscopic confirmation of healing. Time to healing was measured from the index endoscopic intervention (stent placement or first endoscopic/drainage procedure in the non-stented pathway) to the date closure was first documented. Adverse events were recorded using standard clinical documentation and included device migration, intolerance requiring early removal, bleeding, perforation, and need for re-intervention.
Outcomes:Primary—leak closure (clinical/radiologic) and time‑to‑healing (weeks from index endoscopy to closure). Secondary—adverse events (AEs), stent migration, reinterventions, nutrition support, and length of stay.
Outcome definitions:Leak closure required clinical resolution with radiologic confirmation (no contrast extravasation) and/or endoscopic confirmation of healing. Time to healing was measured from the index endoscopic intervention (stent placement or first endoscopic/drainage procedure in the non-stented pathway) to the date closure was first documented. Adverse events were recorded using standard clinical documentation and included device migration, intolerance requiring early removal, bleeding, perforation, and need for re-intervention.
Statistical Analysis: Continuous variables were summarized as
mean (SD) or median (IQR); categorical as n (%). Group comparisons
used t‑test/Mann–Whitney and chi‑square/Fisher’s exact. Time-tohealing
with Kaplan–Meier medians (95% CI) and log-rank were
informative. Adjusted models: logistic regression for closure and Cox
proportional hazards for time‑to‑healing adjusted for leak timing
(acute/subacute/late), leak size/containment, baseline drainage,
and hemodynamic instability. Effect sizes with 95% CIs; sensitivity
analyses excluded crossovers and modeled treatment as time‑varying.
Data availability: De-identified data supporting the findings of this study are available from the corresponding author upon reasonable request.
Data availability: De-identified data supporting the findings of this study are available from the corresponding author upon reasonable request.
Results
Fifty‑seven patients met the inclusion criteria (mean age
35.8 ± 10.2 years; 61.4% female; mean BMI 42.1 ± 7.8 kg/m²). Leaks
were diagnosed a mean of 19 days post‑LSG. Twenty‑three (40.4%)
received SEMS (with/without fixation) and 34 (59.6%) received
non‑stented care consisting of antibiotics, targeted drainage, and/
or endoscopic closure. Overall resolution occurred in 53/57 (93%).
(Table I) demonstrates the demographic characteristics.
Additional leak-characteristic data were extracted from the study spreadsheet and are summarized by index strategy in (Table I-B). The median interval from sleeve gastrectomy to leak diagnosis was 13 days (IQR 7-25; mean 19.1; range 1-73), with 15 acute (<=7 days), 33 subacute (8-42 days), and 9 late (>42 days) leaks. By index strategy, SEMS patients were diagnosed earlier than non-stented patients (mean 14.2 vs 22.4 days; median 10 vs 16 days), and acute leaks were more frequent in the SEMS group (10/23, 43.5%) than in the non-stented group (5/34, 14.7%). Defects >10 mm were also more common with SEMS (15/23, 65.2%) than with non-stented care (12/34, 35.3%), whereas 5-10 mm defects were more frequent in the non-stented group (18/34, 52.9%). CT collection/abscess was common in both pathways (22/23, 95.7% vs 31/34, 91.2%). Contained/localized CT extravasation was observed in 16/23 (69.6%) SEMS patients and 20/34 (58.8%) non-stented patients; diffuse/ uncontained extravasation was recorded only in SEMS patients (5/23, 21.7%), while no CT extravasation was recorded in 14/34 (41.2%) non-stented cases.
Additional leak-characteristic data were extracted from the study spreadsheet and are summarized by index strategy in (Table I-B). The median interval from sleeve gastrectomy to leak diagnosis was 13 days (IQR 7-25; mean 19.1; range 1-73), with 15 acute (<=7 days), 33 subacute (8-42 days), and 9 late (>42 days) leaks. By index strategy, SEMS patients were diagnosed earlier than non-stented patients (mean 14.2 vs 22.4 days; median 10 vs 16 days), and acute leaks were more frequent in the SEMS group (10/23, 43.5%) than in the non-stented group (5/34, 14.7%). Defects >10 mm were also more common with SEMS (15/23, 65.2%) than with non-stented care (12/34, 35.3%), whereas 5-10 mm defects were more frequent in the non-stented group (18/34, 52.9%). CT collection/abscess was common in both pathways (22/23, 95.7% vs 31/34, 91.2%). Contained/localized CT extravasation was observed in 16/23 (69.6%) SEMS patients and 20/34 (58.8%) non-stented patients; diffuse/ uncontained extravasation was recorded only in SEMS patients (5/23, 21.7%), while no CT extravasation was recorded in 14/34 (41.2%) non-stented cases.
Closure occurred in 22/23 (95.7%) SEMS patients (mean healing
10.5 weeks) and 31/34 (91.2%) non‑stented patients (mean healing
8.6 weeks). At face value, the non-stented cohort exhibited a shorter
crude time-to-healing; however, non-stented cases were more likely
to represent earlier or contained leaks, suggesting that case-mix
explains much of the difference. In keeping with our hypothesisgenerating
posture, we report descriptive measures and refrain from
making claims of superiority.
Stent-related adverse events occurred in 6/23 (26.1%) SEMS
patients (predominantly migration or intolerance) and were managed
with repositioning, exchange, or planned removal. Adverse-event
profiles were otherwise comparable between pathways.
E‑VAC therapy was reserved for persistent leaks after stent
removal or failure of non‑stented therapy. Consistent with best
practice, E‑VAC was not performed with a stent in situ;Timing was
individualized in collaboration with surgery and nutrition teams,
while sponge-exchange frequency/count was not clearly reported
in the source records. Table II demonstrates the outcomes of both
groups (stented and non-stented) and summarizes E-VAC rescue
variables.
E-VAC was used as rescue therapy in 9 patients. All 9 patients
achieved leak closure (9/9, 100%). Time to closure after E-VAC was
6, 5, 7, 4, 6, 8, 5, 5, and 5 weeks (mean 5.7 weeks; median 5 weeks;
range 4-8 weeks). Sponge-exchange frequency/count was not
clearly reported in the source records. Although the exact spongeexchange
count was not consistently captured, the E-VAC pathway
was managed as a prolonged rescue course: sponges were generally
exchanged under general anesthesia at longer intervals, approximately
every 5 days when clinically stable, with an expected average total of
10-11 sponge-exchange procedures per patient and total treatment
lasting 4-8 weeks until leak healing.
The revised algorithm, therefore, functions less as a head‑to‑head
comparison and more as a triage map: SEMS for uncontained/large
or later leaks where luminal exclusion aids healing; non‑stented care
for early/contained leaks where drainage and local closure suffice.
The aggregate results—high closure across arms with different case
profiles—support this pragmatic selection logic.
These findings underscore that, in a real-world cohort where management is triaged by leak complexity, both luminal exclusion (SEMS) and drainage-centered strategies can deliver high closure. Given the observational design, comparisons of healing time should be interpreted as descriptive and primarily reflective of baseline leak features and clinical stability at presentation.
These findings underscore that, in a real-world cohort where management is triaged by leak complexity, both luminal exclusion (SEMS) and drainage-centered strategies can deliver high closure. Given the observational design, comparisons of healing time should be interpreted as descriptive and primarily reflective of baseline leak features and clinical stability at presentation.
Discussion
This experience aligns with the broader literature, which
demonstrates that endoscopic therapy has largely supplanted routine
surgery for post-LSG leaks. SEMS achieves high closure rates in
appropriately selected patients, and E-VAC provides an effective
rescue option [8-13, 15, 16]. Device migration has historically limited
SEMS, but contemporary fixation (OTSC or suturing) can reduce
migration to <10% and may improve comfort and dwell stability
[13,15,17]. Non‑stented strategies (drainage ± endoscopic closure)
offer credible efficacy in earlier, contained defects—potentially
explaining shorter crude healing times in that subgroup—yet require
meticulous source control and nutritional optimization [6,12].
Interpretation must remain cautious, as this is a retrospective, single-center series with selection bias—sicker or later leaks are more likely to be triaged to SEMS—and limited power to support multivariable adjustment. As such, we position our algorithm as operational and testable, not definitive. Future work should (i) prospectively capture leak timing/size/containment with standardized imaging; (ii) predefine fixation and dwell protocols; (iii) compare SEMS vs E‑VAC as index therapy in late or uncontained leaks; and (iv) evaluate patient‑reported outcomes and cost. Emerging innovations—including biodegradable or drug‑eluting stents and AI‑assisted risk stratification—may further personalize device choice and aftercare [14,18].
Interpretation must remain cautious, as this is a retrospective, single-center series with selection bias—sicker or later leaks are more likely to be triaged to SEMS—and limited power to support multivariable adjustment. As such, we position our algorithm as operational and testable, not definitive. Future work should (i) prospectively capture leak timing/size/containment with standardized imaging; (ii) predefine fixation and dwell protocols; (iii) compare SEMS vs E‑VAC as index therapy in late or uncontained leaks; and (iv) evaluate patient‑reported outcomes and cost. Emerging innovations—including biodegradable or drug‑eluting stents and AI‑assisted risk stratification—may further personalize device choice and aftercare [14,18].
Our results support a triage-first pathway in which the leak’s
biology—timing, size/containment, and clinical stability—selects the
initial endoscopic track rather than a one-size-fits-all doctrine. In
practice, earlier, contained defects (often already drained) performed
well with a non-stented approach (antibiotics, targeted drainage, ±
focal closure), while later, larger, or uncontained defects benefited
from SEMS with fixation to restore luminal physiology and promote
healing (Figures 1–2) (Tables I–II). The apparent crude difference in
healing time favoring the non-stented group mirrors this selection,
not superiority. This is reinforced by the statistical panel, which
shows no significant difference in closure (p = 0.743) yet a significant
difference in crude healing time (p < 0.001)—a case-mix signal rather
than evidence of an intrinsic advantage (Figure 4). Stent-related AEs,
dominated by migration, were manageable and mitigated by routine
fixation (OTSC/sutures) (Figure 3) (Table II)
Accordingly, the Goal-Oriented Algorithm (Figure 6) operationalizes three bedside signals at diagnosis—timing, size/ containment, and stability/drainage—to determine whether to choose between Non-stented Care (for small, contained, early leaks) and SEMS+ Fixation (for large/uncontained, or late leaks). We emphasize that there is no E-VAC with a stent in situ. Reassessment is planned
Accordingly, the Goal-Oriented Algorithm (Figure 6) operationalizes three bedside signals at diagnosis—timing, size/ containment, and stability/drainage—to determine whether to choose between Non-stented Care (for small, contained, early leaks) and SEMS+ Fixation (for large/uncontained, or late leaks). We emphasize that there is no E-VAC with a stent in situ. Reassessment is planned
after stent removal at 4–6 weeks, not at 10–14 days, unless clinical
deterioration compels an earlier intervention. If a leak persists after
the planned dwell (or after non-stented therapy), escalation proceeds
to E-VAC as a rescue measure, with integrated sepsis and nutrition
bundles throughout the pathway; sponge-exchange frequency/
count was not clearly reported in the source records. This algorithm
harmonizes our cohort’s real-world performance with contemporary
device behavior (migration reduction via fixation) and provides a
reproducible, bedside-ready framework for multicenter validation
(Figures 1-6) (Tables I–III). When E-VAC is selected, the need for
serial sponge exchanges should be anticipated early, as this prolonged
treatment phase can increase procedural burden and resource use
despite high closure potential.
Finally, prevention remains paramount. Standardized staple-line
reinforcement, intraoperative leak testing, and real-time perfusion
assessment (e.g., indocyanine green) may reduce index leak rates
to approximately 1%, while rapid, protocolized sepsis control and
nutrition support likely improve healing once a leak occurs. Our
revised pathway consolidates these principles into a coherent bedside
tool that warrants multicenter validation.
Our closure rates are consistent with contemporary series
reporting high success for fully covered SEMS when combined
with aggressive source control. [8-13,15]. At the same time, internal
drainage and selective closure have been increasingly used for early,
contained leaks, offering a stent-sparing pathway in appropriately
selected patients.[6,12]. The practical implication is that ‘one device
for all leaks’ is unlikely to be optimal; instead, standardized triage
criteria can help align therapy with the dominant physiological goal
(exclusion vs drainage vs closure).
Stent migration remains the central limitation of SEMS therapy.
Systematic efforts to fixate stents with OTSC or suturing have been
associated with lower migration rates in the recent literature and can
improve dwell stability, particularly for proximal defects. [13,15,17].
In our cohort, stent-related adverse events were manageable,
supporting the feasibility of routine fixation as part of a standardized
SEMS pathway.
E‑VAC therapy has expanded the endoscopic armamentarium
for chronic or complex leaks by enabling continuous drainage and
granulation. It is resource intensive and often requires multiple
endoscopies, but can be effective as rescue when luminal exclusion
alone is insufficient. [16,17]. Our protocolized separation—no E‑VAC
with a stent in situ—reflects the need to avoid competing mechanisms
and to ensure adequate cavity access for vacuum therapy. In our
rescue cohort, E-VAC was used in 9 patients and achieved closure
in all cases, with healing documented over 4-8 weeks (mean 5.7
weeks; median 5 weeks), reinforcing its role as a salvage option after
stent removal or failed non-stented therapy. Its use should also be
interpreted in light of procedure burden: E-VAC commonly requires
repeated sponge exchanges under general anesthesia at longer
intervals of approximately every 5 days when the patient is clinically
stable, with an expected average total of 10-11 exchanges per patient.
Limitations warrant emphasis. First, treatment assignment was not randomized and was influenced by leak timing, size/containment, drainage status and clinical stability; residual confounding is therefore unavoidable. Second, patient-reported outcomes (tolerance, dysphagia, quality of life) and cost were not captured systematically. Third, the sample size limits precision for multivariable modeling, and some model outputs cannot be fully reproduced from summary data. Nevertheless, the value of this series lies in its pragmatic operationalization of a triage-first pathway and its clear separation of index strategies and rescue escalation.
From an implementation standpoint, we propose that future prospective work should standardize: (i) definitions and imaging schedules for leak characterization; (ii) dwell time and fixation criteria for SEMS; (iii) drainage and nutrition bundles common to both pathways; and (iv) objective escalation triggers to E‑VAC or surgery.
Limitations warrant emphasis. First, treatment assignment was not randomized and was influenced by leak timing, size/containment, drainage status and clinical stability; residual confounding is therefore unavoidable. Second, patient-reported outcomes (tolerance, dysphagia, quality of life) and cost were not captured systematically. Third, the sample size limits precision for multivariable modeling, and some model outputs cannot be fully reproduced from summary data. Nevertheless, the value of this series lies in its pragmatic operationalization of a triage-first pathway and its clear separation of index strategies and rescue escalation.
From an implementation standpoint, we propose that future prospective work should standardize: (i) definitions and imaging schedules for leak characterization; (ii) dwell time and fixation criteria for SEMS; (iii) drainage and nutrition bundles common to both pathways; and (iv) objective escalation triggers to E‑VAC or surgery.
Such standardization would enable higher-quality comparisons and
would support multicenter validation of bedside algorithms.
From a technical standpoint, SEMS success is rarely “just placing a stent.” Adequate sizing and positioning to cover the defect and to bridge the gastroesophageal junction when necessary, combined with measures that minimize migration (fixation, appropriate dwell, and structured follow-up), likely explain why newer series report lower migration than early experience. [13,15,17] Standardizing peri-procedural care—acid suppression, symptom-driven reassessment, and clear triggers for exchange or early removal— may also improve tolerance and reduce unplanned interventions. Importantly, prolonged dwell without reassessment risks pressure injury; conversely, premature removal risks persistent leakage. Our pathway therefore favors a planned dwell window (4–6 weeks) with reassessment at removal, while allowing earlier action for clinical deterioration.
The non-stented pathway similarly benefits from protocolization. Drainage is the cornerstone: when collections are adequately drained, small and contained defects may close with antibiotics, nutritional optimization, and selective endoscopic closure. Internal drainage strategies have been increasingly adopted in the literature as a “drainfirst” approach, particularly for early leaks with a mature cavity. [6,12] In practice, candidacy for focal closure depends on local tissue conditions (inflammation, necrosis), defect geometry, and whether the cavity is collapsing under drainage; attempting definitive closure without source control risks failure and recurrent sepsis. These considerations support the central premise of our algorithm: match the first-line goal (drain vs exclude) to leak biology rather than to operator preference alone.
Finally, the algorithm is meant to be measurable. Prospective validation should predefine bedside variables (timing, size/ containment, drainage status, stability) and auditable endpoints (closure, time to oral intake, procedure burden, adverse events, and patient-reported tolerance). Algorithm adherence and crossovers should be captured explicitly, and reporting should follow STROBE to facilitate comparison across centers. [5–7,14,18] With such data, the field can move beyond device-by-device debates toward reproducible pathways that integrate drainage, exclusion, and rescue therapy in a coherent escalation framework.
Beyond closure, patient-centered outcomes matter: dysphagia, reflux, nausea, procedure burden, length of stay, and time to resumption of oral intake can differ meaningfully between strategies even when closure rates are similar. Future studies should therefore incorporate standardized symptom assessment and cost/resource metrics alongside imaging-confirmed healing. Such outcomes will help refine thresholds for stent fixation, dwell time, and escalation to E‑VAC or surgery.
Registry-based, pragmatic trials may be particularly suitable for this question because leaks are uncommon and heterogeneous, yet pathway-level standardization is feasible across bariatric centers.
From a technical standpoint, SEMS success is rarely “just placing a stent.” Adequate sizing and positioning to cover the defect and to bridge the gastroesophageal junction when necessary, combined with measures that minimize migration (fixation, appropriate dwell, and structured follow-up), likely explain why newer series report lower migration than early experience. [13,15,17] Standardizing peri-procedural care—acid suppression, symptom-driven reassessment, and clear triggers for exchange or early removal— may also improve tolerance and reduce unplanned interventions. Importantly, prolonged dwell without reassessment risks pressure injury; conversely, premature removal risks persistent leakage. Our pathway therefore favors a planned dwell window (4–6 weeks) with reassessment at removal, while allowing earlier action for clinical deterioration.
The non-stented pathway similarly benefits from protocolization. Drainage is the cornerstone: when collections are adequately drained, small and contained defects may close with antibiotics, nutritional optimization, and selective endoscopic closure. Internal drainage strategies have been increasingly adopted in the literature as a “drainfirst” approach, particularly for early leaks with a mature cavity. [6,12] In practice, candidacy for focal closure depends on local tissue conditions (inflammation, necrosis), defect geometry, and whether the cavity is collapsing under drainage; attempting definitive closure without source control risks failure and recurrent sepsis. These considerations support the central premise of our algorithm: match the first-line goal (drain vs exclude) to leak biology rather than to operator preference alone.
Finally, the algorithm is meant to be measurable. Prospective validation should predefine bedside variables (timing, size/ containment, drainage status, stability) and auditable endpoints (closure, time to oral intake, procedure burden, adverse events, and patient-reported tolerance). Algorithm adherence and crossovers should be captured explicitly, and reporting should follow STROBE to facilitate comparison across centers. [5–7,14,18] With such data, the field can move beyond device-by-device debates toward reproducible pathways that integrate drainage, exclusion, and rescue therapy in a coherent escalation framework.
Beyond closure, patient-centered outcomes matter: dysphagia, reflux, nausea, procedure burden, length of stay, and time to resumption of oral intake can differ meaningfully between strategies even when closure rates are similar. Future studies should therefore incorporate standardized symptom assessment and cost/resource metrics alongside imaging-confirmed healing. Such outcomes will help refine thresholds for stent fixation, dwell time, and escalation to E‑VAC or surgery.
Registry-based, pragmatic trials may be particularly suitable for this question because leaks are uncommon and heterogeneous, yet pathway-level standardization is feasible across bariatric centers.
Conclusions
In post-sleeve gastrectomy leaks, the strategy should follow the
leak, not the other way around. Our triage-first pathway utilizes three
bedside signals (timing, size/containment, and stability/drainage) to
select either non-stented care for early, contained defects or SEMS
with routine fixation for late, large, or uncontained leaks, with E-VAC
reserved strictly as a rescue measure after stent removal. Across our
cohort, both tracks achieved high closure rates; apparent differences
in healing time reflect case mix rather than inherent superiority.
Embedding sepsis control and nutrition bundles is integral to
success. These real-world results are hypothesis-generating and invite
prospective, multicenter validation focused on patient-centered
outcomes—faster healing, fewer procedures, better tolerance, and
earlier return to nutrition.
Work Was Done:
Department of Surgery, Hamad Medical Corporation, Doha,
Qatar
Patient Permission/Consent Declarations: For this retrospective
chart review, the requirement for informed consent was waived by
the approving Institutional Review Board (IRB No. 16208/16).
Authors’ contributions:
Nesreen Khidir: Conceptualization of the manuscript and data
curation. Moamena El Matbouly: writing the manuscript and data
analysis, Moataz Bashah: conceptualization of the manuscript,
and proofreading , Mohammed Al‑Kuwari:: data validation and
conceptualization of the manuscript, and proofreading.
References
Citation
Nesreen K, El Matbouly M, Bashah M, AL-Kuwari M. Endoscopic Management of Sleeve Gastrectomy Leaks: Outcomes of SEMS and Non-Stented Strategies in a Single Tertiary Center. J Obes Bariatrics. 2026;8(1): 1.