
Journal of Obesity and Bariatrics
Download PDF
Research Article
*Address for Correspondence: Zvi H. Perry, Surgical Ward A, Soroka University Medical Center, PO Box 151, Beer-Sheva 64101, Israel, Tel: +972-8-6400610; Fax: +972-8-6477633; E-mail: zperry@bgu.ac.il
Citation: Perry ZH, Netz U, Glazer Y, Atias S, Lantsberg L, et al. The Results of Hiatal Hernia not Amended During Gastric Banding - A Case Report and the Conclusions Stemming from it. J Obes Bariatrics. 2016;3(1): 3.
Copyright © 2016 Perry GH, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Obesity and Bariatrics | ISSN: 2377-9284 | Volume: 3, Issue: 1
Submission: 05 September, 2016| Accepted: 05 October, 2016 | Published: 15 October, 2016
The Results of Hiatal Hernia not Amended During Gastric Banding - A Case Report and the Conclusions Stemming from it
Zvi H. Perry1,2*,Uri Netz1,Yair Glazer1,Shahar Atias1,Leonid Lantsberg1,Solly Mizrahi1,Yael Rafaeli-Alal3 and Eliezer Avinoh1
- 1Surgical Ward A, Soroka University Medical Center, Beer-Sheva, Israel
- 2Moshe Prywes Center for Medical Education, Ben-Gurion University of the Negev, Beer-Sheva, Israel
- 3Head of Thoracic Surgery Unit, Soroka University Medical Center, Beer-Sheva, Israel
*Address for Correspondence: Zvi H. Perry, Surgical Ward A, Soroka University Medical Center, PO Box 151, Beer-Sheva 64101, Israel, Tel: +972-8-6400610; Fax: +972-8-6477633; E-mail: zperry@bgu.ac.il
Citation: Perry ZH, Netz U, Glazer Y, Atias S, Lantsberg L, et al. The Results of Hiatal Hernia not Amended During Gastric Banding - A Case Report and the Conclusions Stemming from it. J Obes Bariatrics. 2016;3(1): 3.
Copyright © 2016 Perry GH, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Obesity and Bariatrics | ISSN: 2377-9284 | Volume: 3, Issue: 1
Submission: 05 September, 2016| Accepted: 05 October, 2016 | Published: 15 October, 2016
Abstract
Introduction: Hiatal hernia is frequent in patients undergoing bariatric surgery [1].There is evidence that laparoscopic gastric banding is associated with deterioration of GERD, however, the treatment of a hiatal hernia accidentally discovered during a LGB is still under debate. We would like to use the current case report to shed some light upon the decision not to close a hiatal hernia discovered accidentally during Lap band, and its grave consequences.Patient description: A 36 old female, with a known LGB, was admitted to the Urology ward due to suspected nephrolithiasis and Left flank pain. Deterioration in her status and worsening of the LUQ pain has led to a CT with subsequent drain insertion due to a suspected effusion. A follow up CT showed the stomach in the left hemithorax, with the drain inserted in the upper border of the stomach. The patient was taken to the OR, and there a multidisciplinary team of general and cardiothoracic surgeons operated upon her. In the operation a left thoracotomy was done to enable the reduction of the stomach back to the abdomen and a thorough drainage of the left chest. After that, in a formal laparotomy a sleeve gastrectomy was done due to necrosis of the greater curvature. An esophagostomy was performed to enable diversion of esophageal content from the stomach.
Discussion and conclusions: Many changes have occurred in thebariatric field since the 1990’s when hiatal hernia was considered a contraindication for LAGB. But, a change of paradigm has occurred, and just like our patient has shown, not operating upon a hiatal hernia during LAGB is extremely dangerous for the patient.
From this stems only one conclusion - If one encounters a hiatal band during a LAGB procedure, be it a primary or revisional one, one has to fix this defect or else endanger his patient unnecessarily
Keywords
LGB; Hiatal hernia; Thoracic drainageIntroduction
In 1541 Sennertus first described the postmortem finding of a strangulated stomach associated with a diaphragmatic hernia. 38 years later, Ambrose Pare reported the death of a patient from colonic strangulation in a diaphragmatic hernia caused by a gunshot wound. Over 4 centuries later, recognition and management of diaphragmatic lesions remains a challenge to surgeons as it was to Pare.Just a reminder - the hiatus is an opening in the diaphragm: the muscular wall separating the chest cavity from the abdomen.
Normally, the esophagus goes through the hiatus and attaches to the stomach. In a hiatal hernia the stomach bulges up into the chest through that opening. So, hiatal hernia is the protrusion (or herniation) of the upper part of the stomach into the thorax through a tear or weakness in the diaphragm (or an enlarged hiatus). Incidence of hiatal hernias increases with age, and other risk factors like obesity, frequent vomiting or coughing, smoking and pregnancy, all these even more frequent in the bariatric patients [1,2]. It has been long debated if patients with hiatal hernia should be operated upon, and when to operate upon these patients was and still is controversial [3,4]. The advocates state that patients with evidence of severe esophageal injury (ulcer, stricture or Barrett’s mucosa) and incomplete resolution of symptoms or relapses while on medical therapy are appropriate candidates to consider for operative intervention [5]. Other patients with a long duration of symptoms, or those in whom symptoms persist at a young age are also considered for operative treatment initially. In these patients, operative therapy is considered an alternative to medical therapy rather than a treatment of last resort.
This is all well known, but what if the patient does not come to surgery due to hiatal hernia symptoms? One must remember that a hiatal hernia is present in up to 15-50% of the patients undergoing bariatric surgery [1]. Thus, what should we do with an accidental finding of a hiatal hernia found during a bariatric procedure? This might be the case in Gastric banding (LGB), in which we have an excellent view of the diaphragm. What should we do in a hiatal hernia accidentally discovered during a LGB? Should we refrain from operating upon it?
We would like to use the current case report to shed some light upon the decision not to close such a hiatal hernia discovered accidentally during a Lap band, and its grave consequences.
Case Presentation
A 36 old female was admitted to the Urology ward due to suspected nephrolithiasis. Urine sample revealed nothing except a moderate erythrocyte count, and US was considered normal.She was 13 weeks pregnant and an OBGYN exam showed no pathology. She complained of LUQ pain, nausea and vomiting, with no fever. Physical exam was considered normal. BMI upon admittance was 27.
Due to the fact she had undergone in the past a Lap Band, a surgical consult was summoned and he decided to open the band (1 cc), evaluation of the CXR done in the ER was evaluated as normal (see Figure 1). The same day she has shown deterioration in her status and worsening of the LUQ pain, which now radiated to the back. It was decided to have her do a gastrografin swallow, and have a chest x-ray to evaluate the position of the band (see Figure 2). Physical exam has shown decreased breathing sounds on the left, and she started to complain of hemoptysis. An internist who was summoned for consult diagnosed pleural effusion on the left (see Figure 3), with a normal ECG, and suspected a pulmonary embolism, and thus the patient was transferred to an internal ward for further evaluation. She now was tachypneic, tachycardic and complained of shortness of breath. She underwent a CT scan, and an insertion of a chest drain under CT. The patient improved somewhat, but 2 days later, due to the large pleural effusion a cardiothoracic surgeon consult was summoned. Meanwhile lab informed the ward of blood cultures containing strep B, and what seems to be intestinal flora. The cardiothoracic surgeon thought the large pleural effusion is masking a tension pneumothorax on the left and thus has used a needle application to aid in diagnosis. After this procedure, which has resulted in a gush of air, it was decided to have a formal chest tube insertion. The tube was inserted under CT. After this, pain was alleviated and the patient stopped being tachycardic. But, in the drain a large amount of puss was seen, and a CXR after the drain has shown that the lung is not recovering as expected. ICU physician was summoned but did not see a need to admit her, and thought she needed a better pain management regime. After another day with pain and no real improvement in her status, she was transferred to the ICU. A day after her admittance she underwent a chest and abdominal CT, due to a large amount of fluid in the drain (1.2 liters). The CT showed a stomach that was in the left hemithorax, with the drain inserted in the upper border of the stomach, with spillage of stomach content into the left chest. The left lung was collapsed and there was a mediastinal shift to the right. The patient was taken immediately to the OR, and there a multidisciplinary team of general and cardiothoracic surgeons operated upon her. In the operation a left thoracotomy was undertaken to enable the reduction of the stomach back to the abdomen, and to enable a thorough drainage of the left chest. After that, in a formal laparotomy a sleeve gastrectomy was done due to necrosis of the greater curvature. An esophagostomy was performed to enable diversion of esophageal content from the stomach. She was returned to the ICU and was covered with Tazocin and fluconazole (due to pleural fluid which showed Candida growth). After a week wound infection was seen, and debridement of the abdominal wound was started with rapid improvement. With this improvement the chest drain was extracted and post pyloric feeding was started.

 A month after the primary operation the esophagostomy was reversed, and she started drinking. She was discharged 36 days after the primary surgery and 44 days after admittance. During this hospitalization she had an abortion. A week after discharge she was in our clinic for a follow-up, and she still suffered from heartburn and a suffocation sensation. These syndromes improved after the administration of PPI’s. She still suffers from a fistulae tract in her chest that drains the pleural cavity. She slowly increased in weight, and her current BMI is 29.
A month after the primary operation the esophagostomy was reversed, and she started drinking. She was discharged 36 days after the primary surgery and 44 days after admittance. During this hospitalization she had an abortion. A week after discharge she was in our clinic for a follow-up, and she still suffered from heartburn and a suffocation sensation. These syndromes improved after the administration of PPI’s. She still suffers from a fistulae tract in her chest that drains the pleural cavity. She slowly increased in weight, and her current BMI is 29.

Figure 1: CXR upon admittance.
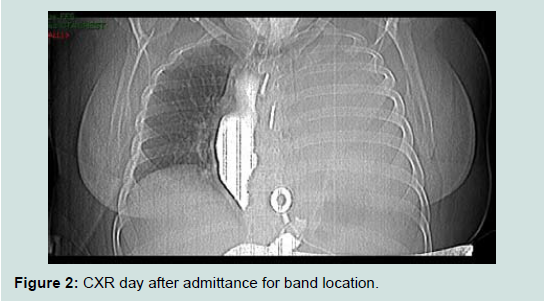
Figure 2: CXR day after admittance for band location.
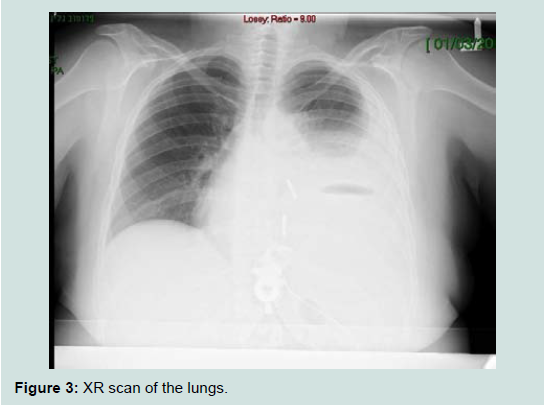
Figure 3: XR scan of the lungs.
When surveying her past medical history, we have found that the LAGB was inserted in 2006 (BMI prior to operation 41), and due to a slippage she had a reposition of the band in 2009. In that operation the hiatus was manipulated and a small hiatal hernia was discerned but not treated.
Discussion
Hiatal hernia is an issue that raises much debate - in Pubmed one can find more than 7000 articles concerning hiatal hernia to date. But when we ask about this same issue concerning bariatric surgery only 1.5% (113 articles) try to answer questions in this field. Of these, only a dozen addressed this issue concerning band patients. In the early 1990’s the presence of a hiatal hernia was generally considered a contraindication to gastric banding in the morbidly obese. In the following years reports indicating favorable outcomes following simultaneous repair of sliding hernias and laparoscopic adjustable gastric banding (LAGB) were seen more and more [1]. Thus, Beitner et al. have found there is no uniform consensus as to the optimal procedure for patients requiring revision after LAGB with a concurrent hiatal hernia [6]. They have found that reoperation for pouch-related (including hiatal hernia repair) problems after LAGB is safe and effective, and that weight loss is maintained after reoperation. Obeid et al. have advocated that hiatal hernia repair (HHR) during LAGB decreases the rate of reoperation [7]. They have shown in their study that the technical aspects of HHR did not appear to be associated with readmission or reoperation, and therefore a standardized approach may not be necessary. Reynoso et al. believed that limited evidence exists regarding the outcomes of patients undergoing LAGB placement with hiatal hernia and concomitant hiatal hernia repair [8]. They studied this group of patients and found that the crural repair is both efficient and safe in patients with hiatal hernia, which is repaired during primary LAGB, and this lowers the need for revisions later. On the other hand, others have seen devastating results not attending to the hiatal hernia during the LAGB procedure, like Faruk et al. which like our surgical team needed to revert a patient to a sleeve gastrectomy due to necrosis of the stomach [9]. A similar occurrence was seen by Bernante et al. who reverted to gastrectomy due to necrosis of the fundus, which resulted in left pleural empyema, just like seen with our patient [10].Reich et al. have addressed the issue of prior evaluation for hiatal hernia and found that preoperative patient evaluation included upper endoscopy to assess the baseline integrity of the stomach and rule out pathology [11]. But, upper endoscopy failed to demonstrate the majority of small hiatal hernias in these patients preoperatively. Bueter et al. also found in their study, that endoscopy and pH monitoring did not predict outcome for gastric banding, and therefore has no relevance in the selection of patients for gastric banding [12]. They declared that hiatal hernias are grossly underappreciated in patients with morbid obesity, due to the presence of a large distal esophageal fat pad. Reich et al. argued that with post-operative internal weight loss, a small crural defect can become relatively large in a short duration of time [11]. Thus, they thought that performing gastric banding without dissecting and repairing the hiatal hernia can lead to incorrect positioning of the gastric band, which is associated with poor weight loss, chronic reflux, and increased complications (like the one our patient has suffered from). Concomitant hiatal hernia repair is felt by Reich et al. to be a necessary component for the correct placement of the gastric band device, which in turn, provides excellent long-term results to these patients [11]. Gulkarov et al. have addressed this and found in their study that adding a Hiatal hernia repair to LAGB where indicated, significantly reduces reoperation rate [13]. They concluded that every effort should be made to detect and repair a hiatal hernia during placement a band, as it will decrease future need for reoperation.
Conclusions
Many changes have occurred in the bariatric field since the 1990’s when hiatal hernia was considered a contraindication for LAGB. Many studies [8,11,13] have shown that hiatal hernia repair during LAGB (be it primary or revisional) is safe and effective. They have also shown a decrease in post-op complication. But, just like our patient has shown, not doing so might be extremely dangerous for the LAGB patient. This has also been seen by others [9,10], and thus is not incidental. From these stems one conclusion - If one encounters a hiatal band during an LAGB procedure, be it a primary or revisional one, one has to fix this defect or else endanger his patient unnecessarily. About the way of fixing it and the management afterwards, it should be evaluated in future research.References
- Landen S (2005) Simultaneous paraesophageal hernia repair and gastric banding. Obes Surg 15: 435-438.
- Tam V, Winger DG, Nason KS (2016) A systematic review and meta-analysis of mesh vs suture cruroplasty in laparoscopic large hiatal hernia repair. Am J Surg 211: 226-238.
- Mittal RK (1993) Hiatal hernia and gastroesophageal reflux: another attempt to resolve the controversy. Gastroenterology 105: 941-943.
- Hendrix TR (1980) Schatzki ring, epithelial junction, and hiatal hernia--an unresolved controversy. Gastroenterology 79: 584-585.
- Beaumont H, Boeckxstaens GE (2009) Does the presence of a hiatal hernia affect the efficacy of the reflux inhibitor baclofen during add-on therapy? Am J Gastroenterol 104: 1764-1771.
- Beitner MM, Ren-Fielding CJ, Kurian MS, Schwack BF, Skandarajah AR, et al. (2014) Sustained weight loss after gastric banding revision for pouch-related problems. Ann Surg 260: 81-86.
- Obeid NR, Deese-Laurent S, Schwack BF, Youn H, Kurian MS, et al. (2014) Location and number of sutures placed for hiatal hernia repair during laparoscopic adjustable gastric banding: does it matter? Surg Endosc 28: 58-64.
- Reynoso JF, Goede MR, Tiwari MM, Tsang AW, Oleynikov D, et al. (2011) Primary and revisional laparoscopic adjustable gastric band placement in patients with hiatal hernia. Surg Obes Relat Dis 7: 290-294.
- Ozturk A, Necati T, Faruk AO (2011) Gastric necrosis due to type II paraesophageal hernia in obese patient with gastric band: rescue sleeve gastrectomy. Surg Obes Relat Dis 7: 330-331.
- Bernante P, Breda C, Zangrandi F, Pomerri F, Pelizzo MR, et al. (2008) Emergency sleeve gastrectomy as rescue treatment for acute gastric necrosis due to type II paraesophageal hernia in an obese woman with gastric banding. Obes Surg 18: 737-741.
- Reich J, Strom K, Pasquariello J, Fresco S, Barbalinardo J (2010) Routine hiatal hernia repair in laparoscopic gastric banding. Surg Technol Int 20: 163-166.
- Bueter M, Thalheimer A, le Roux CW, Wierlemann A, Seyfried F, et al. (2010) Upper gastrointestinal investigations before gastric banding. Surg Endosc 24: 1025-1030.
- Gulkarov I, Wetterau M, Ren CJ, Fielding GA (2008) Hiatal hernia repair at the initial laparoscopic adjustable gastric band operation reduces the need for reoperation. Surg Endosc 22: 1035-1041.