
Case Report
*Address for Correspondence: Dr Emmanuel A. Agaba, MD, Department of Surgery, Montefiore Medical Center, Bronx, New York 10467, USA, Tel: 718-920-4800; E-mail: eagaba@gmail.com
Citation: Agaba EA, Ikedilo O, Vemulapalli P. Small Intestinal Bezoar after Gastric Bypass: An Unusual Cause of Acute Intestinal Obstruction at the Jejunojejunal Anastomosis. J Obes Bariatrics. 2015;2(1): 4.
Copyright © 2015 Agaba EA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Obesity and Bariatrics | Volume: 2, Issue: 1
Submission: 29 December 2014| Accepted: 23 February 2015 | Published: 27 February 2015

The patient tolerated the procedure well and was commenced on bariatric stage 1 diet (non caloric, non carbonated liquid diet) within 6 hours of completion of operation. She made an unremarkable postoperative course and was discharged on the 3rd postoperative day. She was recently seen in the clinic and was doing well.
Case 2
A 35 year old female Nurse with a prior history of laparoscopic Roux-Y-gastric bypass presented acutely to the emergency room with abdominal pain and intolerance of oral intake. Since her surgery 5 years earlier, patient had lost 80 Ib. Psychological evaluation was unremarkable. Clinically, she was acutely ill looking, moderately dehydrated but hemodynamically stable. Abdominal examination revealed a minimally tender central abdomen with no guarding or rebound tenderness.
Basic metabolic panel revealed mild hypokalaemia otherwise the results of the laboratory studies were within normal limits.
Abdominal series revealed small bowel obstruction with multiple air-fluid levels. Computed axial tomogram of the abdomen confirmed small bowel obstruction with proximal dilation of the small intestine and a mottled intraluminal mass in the Roux limb (Figure 3 and 4). Following fluid and electrolytes resuscitation, patient underwent diagnostic laparoscopy, enterotomy of the common channel and removal of the ball of hair within the lumen of the jejunojejunal anastomosis (The operative procedure was similar to the case described above). The enterotomy was repaired in two layers using absorbable sutures. Postoperative recovery was unremarkable.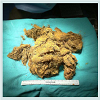
Small Intestinal Bezoar after Gastric Bypass: An Unusual Cause of Acute Intestinal Obstruction at the Jejunojejunal Anastomosis
Emmanuel A. Agaba*, Ojinika Ikedilo and Prathiba Vemulapalli
- Department of Surgery, Montefiore Medical Center at Albert Einstein College of Medicine, Bronx, New York, USA
*Address for Correspondence: Dr Emmanuel A. Agaba, MD, Department of Surgery, Montefiore Medical Center, Bronx, New York 10467, USA, Tel: 718-920-4800; E-mail: eagaba@gmail.com
Citation: Agaba EA, Ikedilo O, Vemulapalli P. Small Intestinal Bezoar after Gastric Bypass: An Unusual Cause of Acute Intestinal Obstruction at the Jejunojejunal Anastomosis. J Obes Bariatrics. 2015;2(1): 4.
Copyright © 2015 Agaba EA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Obesity and Bariatrics | Volume: 2, Issue: 1
Submission: 29 December 2014| Accepted: 23 February 2015 | Published: 27 February 2015
Abstract
Phytobezoars are an uncommon cause of small bowel obstruction and accounts for <6% of all admissions for mechanical small bowel obstruction. Because most bezoars originated from the stomach and may break off, producing small bowel obstruction, it is advisable to examine the entire bowel for these cast-offs especially when removing gastric bezoars. Because the symptoms of bezoars are non-specific and mimic those of other gastrointestinal diseases, delay in diagnosis and treatment is sometimes inevitable. With improved diagnostic aids and advanced skills in laparoscopy, laparoscopic approach offers a suitable alternative that is robust, effective and safe.Keywords
Phytobezoars; Gastric bypass; Jejunojenuostomy; Small bowel obstruction; Laparoscopic treatmentIntroduction
Although the presence of bezoar in the stomach and intestine of herbivorous animals has been known for centuries, the first reference to a human bezoar was in 1779 during an autopsy of a patient who died from gastric perforation and peritonitis [1]. Since then, the number of cases of bezoar in adults has increased due to an increased in the number of operative procedures performed on the gastrointestinal tract. In humans, bezoar-induced small bowel obstruction occurs due to fragmentation and migration of gastric bezoars. Primary small intestinal bezoars are uncommon and are associated with underlying pathology such as stricture, diverticulum or tumor. Only a few cases of mechanical small intestinal obstruction due to bezoars in patients who had previously undergone laparoscopic Roux-en-Y gastric bypass have been described in the literature so far.The presence of phytobezoar induced small bowel obstruction at the site of jejunojejunostomy is rare. The associated mortality for delay in treatment remains high. We present two cases of this unusual cause of small bowel obstruction and reviewed the literature for its diagnosis and management.Case Report
Case 1A 33-years-old female presented acutely to the emergency room with a 48-hours history of colicky central abdominal pain, nonprojectile vomiting and constipation.
Eighteen months earlier, she had undergone routine laparoscopic Roux-en-Y gastric bypass for class 3 morbid obesity and had lost over 70 Ib in weight (Current BMI 38).
She was acutely in painful distress and moderately dehydrated with a tender, non-distended abdomen. No evidence of rebound tenderness.
The results of the laboratory studies were within normal limits.
Abdominal series revealed small bowel obstruction with multiple air-fluid levels. Computed axial tomogram of the abdomen confirmed small bowel obstruction with proximal dilation of the small intestine and a mottled intraluminal mass in the Roux limb (Figure 1 and 2).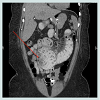
 Following rehydration and placement of indwelling urethral catheter, she was taken to the operating room for diagnostic laparoscopy.
Following rehydration and placement of indwelling urethral catheter, she was taken to the operating room for diagnostic laparoscopy.
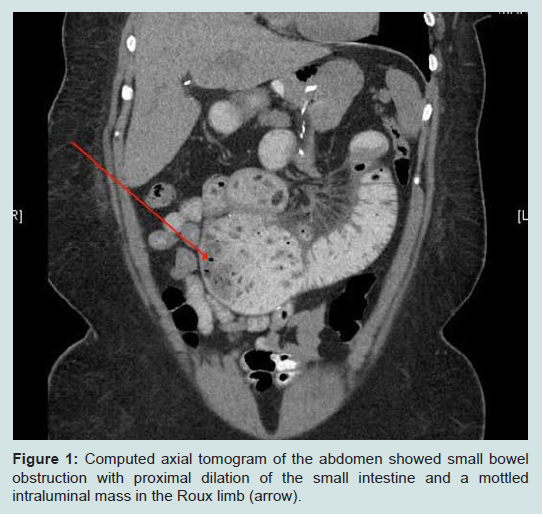
Figure 1: Computed axial tomogram of the abdomen showed small bowelobstruction with proximal dilation of the small intestine and a mottled intraluminal mass in the Roux limb (arrow).
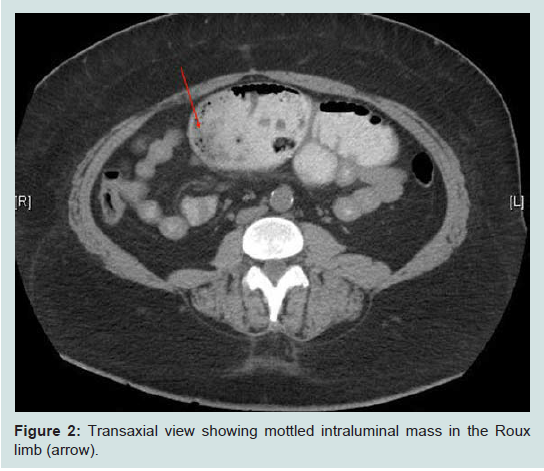
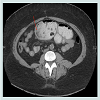
Figure 2: Transaxial view showing mottled intraluminal mass in the Rouxlimb (arrow).
Operation: With the patient placed in supine position, access to the peritoneal cavity was established using a 5 mm optiview trocar placed in the left upper quadrant. Two further 5 mm ports were placed under videoscopic vision in the umbilical region and right mid-clavicular line.
Beginning from the ileocecal junction, the small bowel was run proximally to the duodenojejunal flexure using atraumatic forceps. Intraoperative findings consist of complete intraluminal obstruction and proximally dilated small intestine at the level of jejunojejunostomy with collapse of the distal small bowel. Also, no bezoar was found in the gastric pouch and proximal Roux limb during intraoperative Endoscopy. The gastric remnant and the entire small bowel were examined for potential bezoars but no other bezoar was found. With the phytobezoar identified, a search for internal hernias, adhesions and other synchronous lesions in the stomach was made and excluded. Attempts at milking the bezoar distally was unsuccessful hence a longitudinal enterotomy was made on the antimesenteric border of a healthy portion of the jejunojejunostomy (Figure 3) and the phytobezoar was milked and evacuated in a retrograde manner. To minimize spillage during evacuation of the bezoars, 2 pieces of swabs were placed at the site of the enterotomy. The bezoars were then placed in endocatch bags and retrieved via the 12 mm trocar site. Once evacuated, we reexamined the entire small bowel to ensure complete resolution of the obstruction. The enterotomy was then repaired transversely.
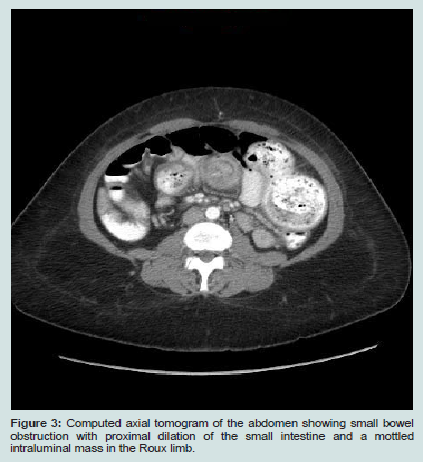
Figure 3: Computed axial tomogram of the abdomen showing small bowelobstruction with proximal dilation of the small intestine and a mottledintraluminal mass in the Roux limb.
The patient tolerated the procedure well and was commenced on bariatric stage 1 diet (non caloric, non carbonated liquid diet) within 6 hours of completion of operation. She made an unremarkable postoperative course and was discharged on the 3rd postoperative day. She was recently seen in the clinic and was doing well.
Case 2
A 35 year old female Nurse with a prior history of laparoscopic Roux-Y-gastric bypass presented acutely to the emergency room with abdominal pain and intolerance of oral intake. Since her surgery 5 years earlier, patient had lost 80 Ib. Psychological evaluation was unremarkable. Clinically, she was acutely ill looking, moderately dehydrated but hemodynamically stable. Abdominal examination revealed a minimally tender central abdomen with no guarding or rebound tenderness.
Basic metabolic panel revealed mild hypokalaemia otherwise the results of the laboratory studies were within normal limits.
Abdominal series revealed small bowel obstruction with multiple air-fluid levels. Computed axial tomogram of the abdomen confirmed small bowel obstruction with proximal dilation of the small intestine and a mottled intraluminal mass in the Roux limb (Figure 3 and 4). Following fluid and electrolytes resuscitation, patient underwent diagnostic laparoscopy, enterotomy of the common channel and removal of the ball of hair within the lumen of the jejunojejunal anastomosis (The operative procedure was similar to the case described above). The enterotomy was repaired in two layers using absorbable sutures. Postoperative recovery was unremarkable.

Figure 4: Intraoperative findings of trichobezoar in Case 2.
Discussion
Bezoars represent a conglomerate of partially digested contents of the gastrointestinal tract such as vegetables (phytobezoar), swallowed hair (trichobezoars) or medicine (pharmacobezoar).Although phytobezoar predominates, most bezoars are seen in the stomach but may occur anywhere from the esophagus to the rectum.
Mechanical small bowel obstruction due (SBO) to bezoars is rare, accounting for < 6% of all causes of small bowel obstruction [2,3]. Although it is unclear how long it takes for phytobezoars to develop, Sarhan et al. described two cases of phytobezoars induced small bowel obstruction occurring within 3 years of RYGB [4]. Typically, small bowel bezoars are found at sites of anatomical narrowing, strictures and diverticulum. This case was unusual, as the jejunojejunostomy had no evidence of stricture. Also, there were no other bezoars elsewhere to suggest fragmentation and migration from other sites. We believe this was a primary jejuunal bezoar.
Among bariatric patients, several studies have shown that phytobezoars may occur in the gastric pouch following Roux-en-Ygastric bypass, vertical banded gastroplasty or placement of adjustable gastric band [5,6].
While the pathogenesis of bezoars remains unclear and appears to be multifactorial, in the adult population, it appears that alteration in gastric anatomy and physiology as well as overindulgence in high fiber diets; abnormal mastication, psychiatric disorders and hypothyroidism may play an important role. Certain medications that alter gastrointestinal function may also play an important role in the pathogenesis of bezoar [7].
Large blood clot (blood phytobezoar) within the lumen of the bowel may cause bowel obstruction in the early postoperative period. It is unclear if this may persist indefinitely. It is unlikely that this was the initiating factor in our series.
In most cases, delayed gastric emptying due to previous gastric surgery appears to be the most common functional abnormality seen in patients with bezoars. Some studies however, have shown that bezoars may occur in some patients with normal gastric anatomy and function [8-10]. Recent studies by Yau et al. and Dirican et al. have shown in two separate studies, that 38% and 17% of patients with bezoars have no prior gastric surgery [10,11]. These findings suggest that other factors beside abnormal gastrointestinal motility maybe involved in the pathogenesis of bezoars. As suggested by Lee [8], factors that may be involved in bezoar formation include changes in the production of acid, pepsin and mucus as well as abnormality in the grinding mechanism and interdigestive migratory motor complex [8].
The clinical presentation of bezoars varies (depending on their sizes and the site) from an innocuous finding during endoscopy in a post gastrectomy patient to complete small bowel obstruction. Affected patients may remain asymptomatic for many years until the bezoar attains a certain size. In up to 20% of patients, the symptoms may persist after removal of the bezoar [12]. The presenting symptoms may also provide some insight into the anatomic location of the bezoar. Gastric bezoars may present with epigastric pain, anorexia, early satiety, post-prandial fullness, nausea, vomiting, halitosis, constipation or gastric ulceration due to pressure necrosis and subsequent bleeding. Rarely, it may present with gastric outlet obstruction.
Small bowel bezoars typically present with signs and symptoms of partial or complete intestinal obstruction or may presents with perforation requiring urgent surgical intervention.
Bezoars have been reported in all age groups. Doo et al. reported a case of mechanical SBO due to bezoar in an infant while Seenu and colleagues described a case of phytobezoar induced small bowel obstruction in an edentulous 70-years-old man [13,14].
As often seen in most cases, physical findings are lacking. As shown in the present case, small bowel bezoars usually present acutely with features of intestinal obstruction or perforation.
The advert of multi-slide computed axial tomogram has herald a new era of diagnostic capability for small bowel bezoars as it has significantly improved preoperative diagnosis. Currently, abdominal CT scan is the diagnostic modality of choice for detecting small bowel bezoars as it can also detect additional bezoars within the gastrointestinal tract. Traditionally, oral contrast is administered during such study. Care should be taken to ensure that the patient does not aspirate the contrast. Characteristic radiologic findings consist of intraluminal mass with a mottled appearance due to the presence of air within the interstices [15]. These findings may mimic small bowel fecalization or many other clinical entities such as intraluminal tumors. CT findings in conjunction with findings on exploration namely hard junks of particulate matter often near the ileocecal valve should be considered pathognomonic for small bowel bezoars. It warrants a mandatory search for the site of the bezoar, which can include an intra-operative Endoscopy to exclude gastric bezoar showering to the small bowel.
Several medical options have been proposed for the treatment of gastric bezoars [15,16]. Because the data on the prevalence of mechanical small bowel obstruction due to bezoars and medical treatment are scant, medical treatment is currently not recommended.
Traditional definitive surgical management consists of exploratory laparotomy with milking of contents into the cecum, or performing enterotomy with retrieval of the contents. Because synchronous bezoars are found in the stomach or other areas of the gastrointestinal tract, it is mandatory to carry out a thorough exploration of the small intestine and colon to avoid recurrence of intestinal obstruction due to a retained bezoar.
As others have documented, successful treatment with laparoscopic enterotomy is feasible [10]. Our clinical report adds further information about laparoscopic enterotomy as an effective, less invasive treatment for mechanical small bowel obstruction due to bezoars and is associated with shorter hospital stay, early return of gastrointestinal function as well as recovery time.
Conclusion
Mechanical SBO due to bezoar is uncommon and it remains a diagnostic challenge even to the seasoned clinician. The potential for complications due to delay in diagnosis and treatment remains high. Surgical treatment is advised, as the available medical treatments are ineffective. Where available laparoscopic approach is recommended, as it is associated with early return of gastrointestinal function as well recovery.References
- Naik S, Gupta V, Naik S, Rangole A, Chaudhary AK, et al. (2007) Rapunzel syndrome reviewed and redefined. Dig Surg 24: 157-161.
- Singh N, Digray NN, Parihar S, Langer R (2006) Phytobezoar induced ileal obstruction in children: report of two cases. JK Sci 8: 103-105.
- Teng HC, Nawawi O, Ng KL, Yik Y (2005) Phytobezoar: an unusual cause of intestinal obstruction. Biomed Imaging Interv J 1: e4.
- Sarhan M, Shyamali B, Fakulujo A, Ahmed L (2010) Jejunal bezoar causing obstruction after laparoscopic Roux-en-Y gastric bypass. JSLS 14: 592-595.
- Pinto D, Carrodeguas L, Soto F, Lascano C, Cho M, et al. (2006) Gastric bezoar after laparoscopic Roux-en-Y gastric bypass. Obes Surg 16: 365-368.
- Lung D, Cuevas C, Zaid U, Ancock B (2011) Venlafaxine pharmacobezoar causing intestinal ischemia requiring emergent hemicolectomy. J Med Toxicol 7: 232-235.
- Lee J (1996) Bezoars and foreign bodies of the stomach. Gastrointest Endosc Clin N Am 6: 605-619.
- Calabuig R, Navarro S, Carrió I, Artigas V, Monés J, et al. (1989) Gastric emptying and bezoars. Am J Surg 157: 287-290.
- Yau KK, Siu WT, Law BK, Cheung HY, Ha JP, et al. (2005) Laparoscopic approach compared with conventional open approach for bezoar-induced small-bowel obstruction. Arch Surg 140: 972-975.
- Dirican A, Unal B, Tatli F, Sofotli I, Ozgor D, et al. (2009) Surgical treatment of phytobezoars causes acute small intestinal obstruction. Bratisl Lek Listy 110: 158-161.
- Zarling EJ, Thompson LE (1984) Nonpersimmon gastric phytobezoar. A benign recurrent condition. Arch Intern Med 144: 959-961.
- Duman L, Savas C, Ceyhan L (2011) An unusual cause of intestinal obstruction in an Infant: phytobezoar within a Meckel diverticulum. J Pediatr Surg 46: 1678-1679.
- Seenu V, Iyer G, Rao CS (2010) The lemon story-an unusual phytobezoar causing acute small bowel obstruction. Oman Med J 25.
- Boudiaf M, Soyer P, Terem C, Pelage JP, Maissiat E, et al. (2001) CT evaluation of small bowel obstruction. Radiographics 21: 613-624.
- Ha SS, Lee HS, Jung MK, Jeon SW, Cho CM, et al. (2007) Acute intestinal obstruction caused by a persimmon phytobezoar after dissolution therapy with Coca Cola. Korean J Intern Med 22: 300-303.
- Ladas SD, Triantafyllou K, Tzathas C, Tassios P, Rokkas T, et al. (2002) Gastric phytobezoars may be treated by nasogastric Coca-Cola lavage. Eur J Gastroenterol Hepatol 14: 801-803.