
Journal of Neurology and Psychology
Download PDF
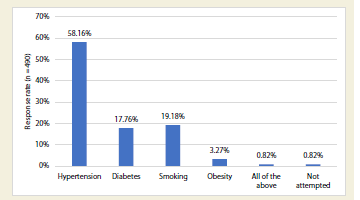 Figure 1:Distribution of responses to common risk factors for stroke among
young Indian patients
Figure 1:Distribution of responses to common risk factors for stroke among
young Indian patients
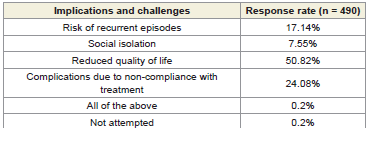 Table 1:Distribution of responses to long-term implications and challenges faced
by young adult stroke patients in daily life
Table 1:Distribution of responses to long-term implications and challenges faced
by young adult stroke patients in daily life
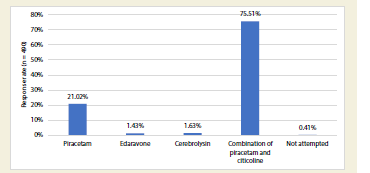 Figure 2:Distribution of response to promising neuroprotective agents for young adult stroke patients in Indian settings
Figure 2:Distribution of response to promising neuroprotective agents for young adult stroke patients in Indian settings
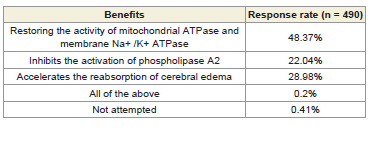 Table 2:Distribution of responses to the benefits of citicoline in stroke patients
Table 2:Distribution of responses to the benefits of citicoline in stroke patients
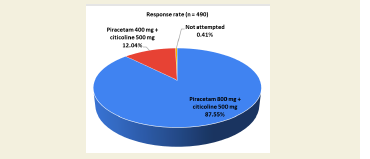 Figure 3:Distribution of responses to the most commonly prescribed
strengths of piracetam and citicoline for acute stroke in young patients
Figure 3:Distribution of responses to the most commonly prescribed
strengths of piracetam and citicoline for acute stroke in young patients
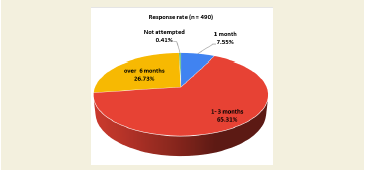 Figure 4:Distribution of responses to the duration of piracetam and citicoline
combination treatment for young adult stroke patients in clinical practice
Figure 4:Distribution of responses to the duration of piracetam and citicoline
combination treatment for young adult stroke patients in clinical practice
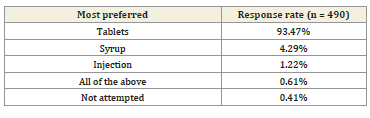 Table 3:Distribution of responses to the most preferred formulation of piracetam
and citicoline combination for young adult stroke patients in clinical practice
Table 3:Distribution of responses to the most preferred formulation of piracetam
and citicoline combination for young adult stroke patients in clinical practice
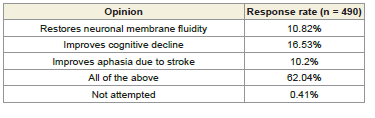 Table 4:Distribution of responses to the opinion regarding the combination of
piracetam and citicoline in post-stroke recovery
Table 4:Distribution of responses to the opinion regarding the combination of
piracetam and citicoline in post-stroke recovery
Research Article
Expert Perspectives on the Clinical Use of Piracetam and Citicoline in Stroke and Piracetam Monotherapy in Treating Vertigo
Manjula S* and Krishna Kumar M
Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India
*Address for Correspondence:Dr Manjula S, Department of Medical Services, Micro Labs Limited,
Bangalore, Karnataka, India. Email Id: drmanjulas@gmail.com
Submission: June 21, 2025
Accepted: July 14, 2025
Published: July 16, 2025
Copyright: © 2025 Manjula S, et al. This is an open access article
distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Keywords: Stroke; Quality of Life; Piracetam; Citicoline; Dosage; Rehabilitation
Abstract
Objective:To gather clinicians’ perspectives on the clinical use
of piracetam and citicoline in stroke and piracetam monotherapy in
treating vertigo in Indian settings.
Methods:This cross-sectional study was conducted among clinicians across Indian settings and focused on the clinical practices, preferences, and experiences on the combination of citicoline and piracetam for stroke, and piracetam alone for vertigo. Participants independently completed the 24-item questionnaire after providing informed consent. Descriptive statistics were used to analyze the data, with categorical variables presented as percentages and visualized through pie and bar charts in Excel.
Result:The study involving 490 participants identified hypertension as the most common risk factor for stroke in young Indian patients (58%). Half of the respondents reported reduced quality of life poststroke, while 76% supported piracetam and citicoline as effective neuroprotective agents. Citicoline’s role in restoring mitochondrial ATPase and membrane Na+/K+ ATPase was emphasized by 48% of experts. Most participants reported common dosages of 800 mg piracetam and 500 mg citicoline (87.55%), with a typical treatment duration of 1-3 months (65%). Tablets were the preferred formulation (93.47%), and 62% highlighted the combination’s role in improving cognitive decline, membrane fluidity, and aphasia recovery.
Conclusion:The study emphasizes the prominence of hypertension as a major risk factor and the widespread use of piracetam and citicoline as neuroprotective agents. The combination therapy is notably linked to improved cognitive function, aphasia recovery, and neuronal membrane restoration. The preference for oral tablet formulations and a treatment duration of 1-3 months reflects current clinical practices in Indian settings.
Methods:This cross-sectional study was conducted among clinicians across Indian settings and focused on the clinical practices, preferences, and experiences on the combination of citicoline and piracetam for stroke, and piracetam alone for vertigo. Participants independently completed the 24-item questionnaire after providing informed consent. Descriptive statistics were used to analyze the data, with categorical variables presented as percentages and visualized through pie and bar charts in Excel.
Result:The study involving 490 participants identified hypertension as the most common risk factor for stroke in young Indian patients (58%). Half of the respondents reported reduced quality of life poststroke, while 76% supported piracetam and citicoline as effective neuroprotective agents. Citicoline’s role in restoring mitochondrial ATPase and membrane Na+/K+ ATPase was emphasized by 48% of experts. Most participants reported common dosages of 800 mg piracetam and 500 mg citicoline (87.55%), with a typical treatment duration of 1-3 months (65%). Tablets were the preferred formulation (93.47%), and 62% highlighted the combination’s role in improving cognitive decline, membrane fluidity, and aphasia recovery.
Conclusion:The study emphasizes the prominence of hypertension as a major risk factor and the widespread use of piracetam and citicoline as neuroprotective agents. The combination therapy is notably linked to improved cognitive function, aphasia recovery, and neuronal membrane restoration. The preference for oral tablet formulations and a treatment duration of 1-3 months reflects current clinical practices in Indian settings.
Introduction
Globally, over 12.2 million individuals experience their first
stroke every year, equating to one stroke every three seconds.[1]
According to the 2025 Global Stroke Fact Sheet, the global burden of
stroke has risen significantly, with a 70% increase in incident strokes,
a 44% rise in stroke-related deaths, and a 32% increase in disability adjusted
life years (DALYs). This burden is particularly pronounced
in lower-income and lower-middle-income countries, which account
for 87% of stroke-related deaths and 89% of DALYs.[2] In India, the
stroke burden is rising steadily, making it the fourth leading cause of
death and the fifth leading cause of disability. The annual incidence of
stroke in India ranges between 105 and 152 per 100,000 individuals.
[3] Vertigo is a common and often debilitating neurological symptom,
affecting approximately one in five individuals at least occasionally.
[4] Its global prevalence is estimated to range between 3% and 10%.
[4] In India, vertigo is reported in 0.71% of the rural population.[5]
Piracetam is beneficial in managing both vertigo and stroke related
complications due to its multifaceted mechanism of
action. In stroke, piracetam enhances neurotransmission in the
glutamatergic and cholinergic systems, contributing to improved
cognitive and motor recovery. It also restores membrane fluidity and
enhances microcirculation by reducing vasospasm and promoting
cerebral blood flow, thereby supporting vascular health in ischemic
conditions.[6] In vertigo, piracetam helps reduce the frequency,
severity, and duration of episodes, along with improving associated
malaise and imbalance.
Citicoline, on the other hand, aids in neuronal recovery by
providing choline and cytidine, essential for phosphatidylcholine
synthesis and acetylcholine production. This facilitates neuronal
membrane repair and regeneration. Furthermore, citicoline reduces
free fatty acid-induced toxicity during ischemic insults, offering
neuroprotection in acute stroke and aiding functional recovery.[7]
The synergistic action of piracetam and citicoline addresses both
vascular and neuronal mechanisms for the effective management of
stroke. This study aims to gather expert opinions on the clinical use
of piracetam and citicoline in stroke recovery, as well as piracetam
monotherapy in treating vertigo.
Methodology
We carried out a cross-sectional study among neuropsychiatry
experts from routine healthcare settings across India from June 2024
to December 2024. The study was conducted after receiving approval
from Bangalore Ethics, an Independent Ethics Committee, which was
recognized by the Indian Regulatory Authority, the Drug Controller
General of India.
A convenient sampling technique was used, and an invitation was
sent to leading clinicians in managing neurological conditions in the
month of March 2024 for participation in this Indian survey. About
490 clinicians from major cities of all Indian states, representing the
geographical distribution, shared their willingness to participate and
provide necessary data. The questionnaire booklet titled TRYGO
(CiTi colineand PiRaceteam molecule in Management of stroke) was
sent to clinicians who were interested in participating in this study.
The TRYGO study questionnaire included 24 questions related to
clinical practices, preferences, and experiences with citicoline and
piracetam for stroke, as well as piracetam monotherapy for vertigo.
Survey questions were developed using the methods designed to
collect perspectives from the practitioners. Reliability as determined
by a split-half test (coefficient alpha) was adequate but should
be improved in future versions of the questionnaire. A study of
criterion validity was undertaken to test the questionnaire and to
develop methods of testing the validity of measures of Physicians’
Perspectives. However, the extraneous variable in this includes the
clinician’s experience, usage of the newer drugs, etc. The two criteria
used were the doctors’ perspectives from the clinical practice and the
assessment of an external assessor and statistician. Participants were
allowed to skip questions and were instructed to complete the survey
independently without consulting colleagues. Informed consent was
obtained from all participants before the study commenced.
Statistical analysis:
The data were analyzed using descriptive statistics, with
categorical variables expressed as percentages to illustrate their
distribution. Frequency and percentage calculations were conducted,
and pie and bar charts were created using Microsoft Excel 2013
(version 16.0.13901.20400).
Results
The study gathered responses from 490 participants. Nearly
42% reported that the 36–45-year age group is the most common
demographic for young adult stroke patients (18 to 50 years) in
clinical practice in India. More than half of the participants (53.27%)
indicated that they encounter young adult stroke patients in clinical
practice 11–20% of the time. Approximately 58% of the experts
identified hypertension as the most common risk factor for stroke
among young Indian patients [Figure 1].
About 44% of participants highlighted limited access to physical
rehabilitation as a significant challenge faced by young adult stroke
patients during recovery in India. Over half of the participants
(58.57%) emphasized the importance of regular counseling sessions
for assessing the psychological and emotional needs of young adult
stroke patients during their recovery.
Approximately 62% of participants identified rehabilitation
centers as the most commonly available and effective resources
for supporting the recovery of young adult stroke patients in
India. Around 40% of clinicians suggested that training healthcare
professionals on early stroke recognition measures could improve
stroke awareness and encourage early intervention for young
Indians. Half of the respondents (50.82%) reported that young adult
stroke patients experience reduced quality of life due to long-term
implications and challenges in daily life [Table 1]. About 34% of
clinicians cited patient compliance with regular medication as one of
the most challenging aspects of managing young adult stroke patients
in clinical practice. According to 40% of participants, 26-50% of
young adult stroke patients are prescribed neuroprotective agents.
Over half of the respondents (56.12%) acknowledged that
neuroprotective agents help improve functional outcomes and
quality of life for young adult stroke patients. A significant 76% of the
clinicians considered the combination of piracetam and citicoline as
promising neuroprotective agents for young adult stroke patients in
India [Figure 2].
Approximately 48% of participants highlighted that citicoline
benefits young adult stroke patients by restoring the activity of
mitochondrial ATPase and membrane Na+/K+ ATPase [Table 2].
The majority (61.22%) of experts reported that 26–50% of young
adult stroke patients are prescribed a combination of piracetam and
citicoline. Most respondents (87.55%) stated that the most commonly
prescribed dosages of piracetam and citicoline for acute stroke in
young patients are 800 mg and 500 mg, respectively[Figure 3].
About 26% of participants reported that the key advantage of fixed-dose combinations of piracetam and citicoline is their synergistic effects. According to 65% of respondents, the typical duration of piracetam and citicoline combination treatment for young adult stroke patients is 1–3 months[Figure 4]. Nearly all participants (93.47%) indicated that tablets are the preferred formulation of piracetam and citicoline for young adult stroke patients in clinical practice [Table 3]. Around 62% of experts noted that the combination of piracetam and citicoline helps restore neuronal membrane fluidity, improve cognitive function, and alleviate aphasia in post-stroke recovery [Table 4].
About 26% of participants reported that the key advantage of fixed-dose combinations of piracetam and citicoline is their synergistic effects. According to 65% of respondents, the typical duration of piracetam and citicoline combination treatment for young adult stroke patients is 1–3 months[Figure 4]. Nearly all participants (93.47%) indicated that tablets are the preferred formulation of piracetam and citicoline for young adult stroke patients in clinical practice [Table 3]. Around 62% of experts noted that the combination of piracetam and citicoline helps restore neuronal membrane fluidity, improve cognitive function, and alleviate aphasia in post-stroke recovery [Table 4].
Nearly half of the participants (47.96%) considered adjuvant
therapy a factor influencing their preference for piracetam in treating
vertigo patients. Approximately 43% identified mixed-origin vertigo
as the most common indication for piracetam prescription. About
49% of experts reported that piracetam treatment reduces the
frequency of vertigo episodes.
Over half of the experts (53.27%) recommended a piracetam
dosage range of 800–1600 mg/day for vertigo treatment. Nearly 42%
indicated that the typical duration of piracetam treatment for vertigo
is 1-4 weeks.
Discussion
The study results underscore the importance of early intervention
and combination therapies in managing neuropsychiatric
disorders. Hypertension emerged as the most common risk factor
for stroke among young Indian patients, as reported by a majority
of participants. Consistent with these findings, Parikshith et al.
identified hypertension as the most prevalent risk factor for stroke,
affecting 18 patients (36%) in their cohort.[8] Similar observations
were made by Dalal et al., who reported an incidence of 46.7%, and
Alvarez et al., who reported 23%, all recognizing hypertension as a
significant contributor to stroke risk.[9,10] This underscores the need
for aggressive blood pressure control as part of preventive strategies.
Respondents also highlighted the long-term impact of stroke on
young patients’ quality of life, emphasizing challenges in daily living
and sustained health concerns.Schneider et al. found that young
ischemic stroke survivors often experience persistent declines in
health-related quality of life (HRQOL), except for those achieving
excellent functional recovery.[11] Similarly, Rohner et al. reported
that self-rated HRQOL, depression, and fatigue levels in adult
paediatric stroke survivors are comparable to those of healthy adult
peers.[12]
Most study participants identified the combination of piracetam
and citicoline as a promising neuroprotective treatment for young
adult stroke patients in India. This aligns with findings from
previous studies, including a cross-sectional survey conducted by
the current authors, which reported this combination as the most
commonly prescribed neuroprotective agent.[13] A prospective
study by Shibu et al. demonstrated that while both citicoline and
citicoline-piracetam combination improved post-stroke recovery,
combination therapy showed superior neuroprotection and quality of
life outcomes, supporting its inclusion in stroke recovery protocols.
[14] Additionally, clinical evidence suggests that citicoline aids in
restoring neuronal membrane integrity and enhancing mitochondrial
function, while piracetam facilitates neuroplasticity, collectively
contributing to improved recovery outcomes in young adult stroke
patients.[15,16]
Many study participants emphasized that citicoline benefits
young adult stroke patients by restoring mitochondrial ATPase
and membrane Na+/K+ ATPase activity. Supporting this, a
pharmacological and clinical review by Secades reported citicoline’s
role in restoring these enzyme activities, inhibiting phospholipase
A2 activation, and accelerating cerebral edema reabsorption in
experimental models.[17] Similarly, Bermejo et al. reported that
citicoline not only restores mitochondrial ATPase and membrane
Na+/K+ ATPase activity but also reduces neuroinflammation
caused by ischemia, limits reactive oxygen species production, and
promotes cerebral edema resolution, underscoring its multifaceted
neuroprotective effects.[18]
Most participants reported that the typical prescribed doses of
piracetam and citicoline for acute stroke in young patients are 800
mg and 500 mg, respectively. Murugesan et al. found that a 500 mg
oral dose of citicoline can be safely taken with minimal adverse effects
and appears to improve both functional and neurological deficits.
[19] Similarly, Doijad et al. highlighted the availability of a fixed-dose
combination tablet containing 500 mg of citicoline and 800 mg of
piracetam, providing a convenient treatment option. [20] A related
cross-sectional study further indicated that 800 mg of piracetam is
frequently prescribed to most stroke patients, reinforcing its common
use in clinical practice.[13]
A significant proportion of current study participants reported
that the typical duration for the combination treatment of piracetam
and citicoline in young adult stroke patients is 1-3 months. Tablets
were identified as the preferred form for administering these agents
in clinical practice.A previous study by the current authors similarly
observed that many physicians recommend this combination therapy
for a 1-3-month duration.[13] Additionally, the authors also noted
that 400 mg tablets are commonly prescribed, with 11% of clinicians
opting for 1200 mg tablets specifically for managing vertigo, reflecting
diverse dosing preferences based on clinical indications.[13]
A majority of respondents emphasized that the combination
of piracetam and citicoline effectively restores neuronal membrane
fluidity, improves cognitive decline, and alleviates aphasia during
post-stroke recovery. A similar cross-sectional study reported
significant improvement in aphasia following stroke, with 18%
of respondents attributing this to restored neuronal membrane
fluidity. Additionally, 93% of clinicians in the study agreed that
piracetam enhances cognitive recovery after surgery.[13] Sharma et
al. further highlighted that piracetam, a nootropic agent, enhances
cerebral blood flow, improves oxygen extraction, restores membrane
fluidity, and modulates neurotransmission, reinforcing its role in
neuroprotection and cognitive enhancement.[21]
The study provides valuable insights into clinical practices
related to young adult stroke patients in India, offering data on
demographics, risk factors, treatment approaches, and recovery
challenges. It highlights the use of piracetam and citicoline in acute
stroke management, particularly their effectiveness in improving
cognitive decline and post-stroke recovery. The large sample size
(490 participants) strengthens the findings and helps identify trends
in treatment practices, such as dosage preferences and rehabilitation
strategies. However, the reliance on self-reported data may introduce
bias or inaccuracies. Additionally, the survey’s cross-sectional design
limits conclusions about long-term outcomes or causality. The
findings are specific to clinical practices in India and may not be
generalizable to regions with different healthcare systems or stroke
management protocols.
Conclusion
The study highlights hypertension as the most common risk
factor in young adult stroke patients in Indian settings, with limited
rehabilitation access and medication non-compliance as key
challenges. The combination of piracetam and citicoline is widely
regarded as having perceived efficacy for cognitive recovery, with oral
tablets preferred for convenience. Improved healthcare training and
enhanced rehabilitation access are crucial for better outcomes.
Disclosure of compliance with ethical principles:
The study was conducted after receiving approval from Bangalore
Ethics, an Independent Ethics Committee, which was recognized by
the Indian Regulatory Authority, Drug Controller General of India.
References
Citation
Manjula S, Krishna Kumar M. Expert Perspectives on the Clinical Use of Piracetam and Citicoline in Stroke and Piracetam Monotherapy in Treating Vertigo. J Neurol Psychol. 2025; 11(1): 01.