
Journal of Neurology and Psychology
Download PDF
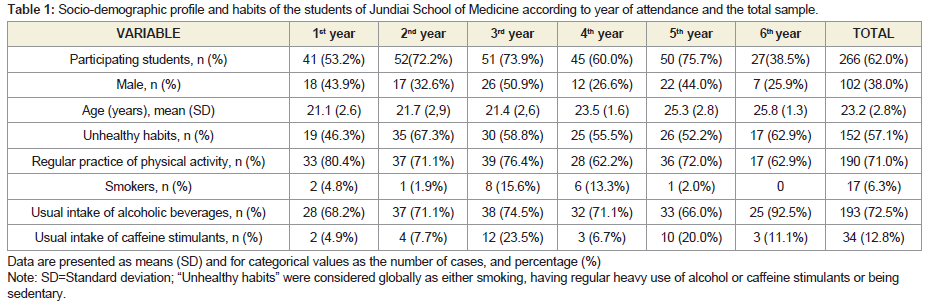 Table 1: Socio-demographic profile and habits of the students of Jundiai School of Medicine according to year of attendance and the total sample.
Table 1: Socio-demographic profile and habits of the students of Jundiai School of Medicine according to year of attendance and the total sample.
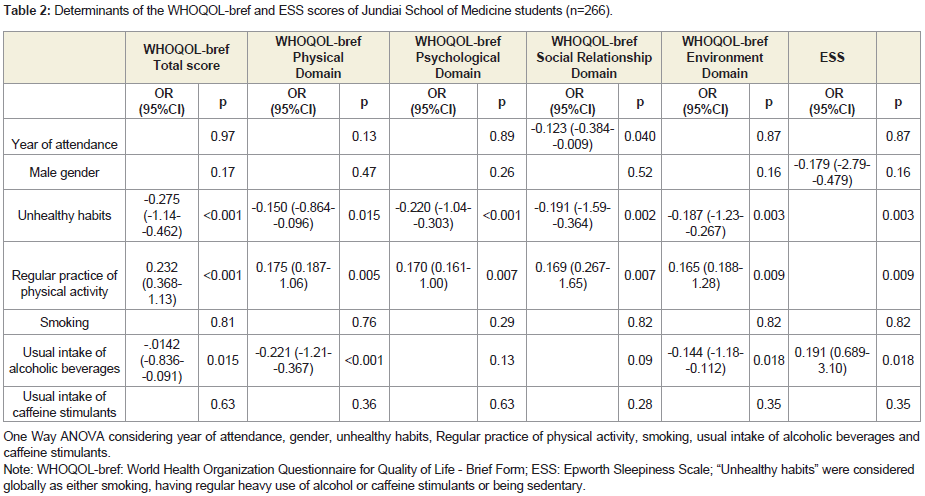 Table 2: Determinants of the WHOQOL-bref and ESS scores of Jundiai School of Medicine students (n=266).
Table 2: Determinants of the WHOQOL-bref and ESS scores of Jundiai School of Medicine students (n=266).
Research Article
High Levels of Excessive Daytime Sleepiness among Medical Students is Associated with Worst Quality of Life, and it is Higher among Female Students
Lima RP, Brenelli LM, Viana Miguel MA, Dias Pinto CC, Aprahamian I and Nunes PV*
Jundiai School of Medicine, Jundiai, Sao Paulo, Brazil
*Address for Correspondence: Nunes PV, Jundiai School of Medicine, rua Francisco Telles, 250, Jundiai, Sao Paulo, Brazil, Tel: +55 11 33952100; E-mail: paula@formato.com.br
Submission: December 14, 2019;
Accepted: January 30, 2020;
Published: February 04, 2020
Copyright: © 2020 Lima RP, et al. This is an open access article
distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Abstract
Objective:
This study aimed to analyze quality of life and excessive
daytime sleepiness of medical students and to correlate it with possible
conditioning factors such as gender, habits and year of attendance at
the Medical School.
Methods:
The study was cross-sectional, using self-administered
questionnaires to all medical students. Questionnaires included
sample profile, the World Health Organization Quality of Life
assessment (WHOQOL-bref) and the Epworth Sleepiness Scale (ESS).
1.3. Results: The sample covered 266 students, 62% of which were
female. Excessive daytime sleepiness according to the ESS was found
in 66% of the sample. An inverse correlation of sleepiness and quality
of life was found (r=-0.338; p<0.001). Sleepiness was greater among
women (p=0.011), but had no correlation to the year of attendance
of the students. No differences were found in WHOQOL-bref total
score regarding gender or year of attendance. Students with healthier
habits, more specifically with regular physical activity and without
regular use of alcohol had higher scores on WHOQOL-bref total score
(p<0.001 and 0.015, respectively).
Conclusion:
Excessive daytime sleepiness was present in a
considerable part of the medical students, especially amongst
women. Healthier habits and regular physical activity were associated
with greater quality of life. Future studies, prospectively collecting
information, could bring greater reliability concerning the impact
of the course would on quality of life and sleepiness, with special
emphasis on gender differences.
Keywords
Quality of life; Students; Medical; Education; Medical; Sleep deprivation; Stress; Psychological; Burnout
Introduction
During their course, undergraduate students of Medicine face
countless stress factors which can have serious consequences on
their health [1]. From the second half of the 20th century on, major
advances have occurred in different areas of Medicine, and each year
thousands of new publications are released. This makes university
courses complex, curricular contents extensive, and related workload
demanding. In search of good professional qualifications, students are
urged to tackle a series of supplementary activities such as research,
academic monitoring, internships, and other strenuous activities
they are subjected to, in terms of work hours and performance. In
addition, behaviors, skills, and mature attitudes are required from
students throughout their learning processes. Therefore, medical
career studies require impressive levels of dedication, from the highly
competitive entrance exams, through the graduation challenges,
to medical specialization which requires lengthy shifts, study and working hours [1]. Therefore, the academic overload faced by
medical student routines directly influences their quality of life.
The concept of quality of life is not new: Aristotle (384-322 BC)
described happiness as a virtuous activity of the soul, a final goal
that encompasses the totality of one´s life. Hippocrates (460-377
BC) asserted that balance provides a healthy body, which is directly
connected with the environment [2]. The idea also appears in ancient
Chinese philosophy, which defines that quality of life can be achieved
when the positive and negative forces, represented by the concepts
of Yin and Yang, are in balance. Thus, the concept has roots in both
Western and Eastern culture [2]. The term quality of life was used in
the United States after World War II for describing the acquisition
of goods. Later, this notion was extended in order to measure the
economic development of a society, comparing different regions
through economic indicators such as per capita income and gross
domestic product. Subsequently, the concept began to denote social
development through education, health, housing and transportation,
among other parameters [3]. Given the inherent complexity of the
definition of quality of life, in 1995 the World Health Organization
brought together experts from around the world and identified
quality of life as: “the individual’s perception of their position in life
in the context of culture and value systems in which they live and
in relation to their goals, expectations, standards and concerns” [4],
and six domains were identified: physical, psychological, level of
independence, social relations, environment and religious beliefs [4-6]. Quality of life has emerged as a new goal to be achieved, beyond
cure, control of diseases or the extension of life [7]. Too many activities
and requirements in Medicine courses prevent students from having
time to exercise, to take care of their health, to enjoy time with their
family and friends or to develop other interests, with impacts on their
quality of life. Stressful factors, such as great demands on learning, a
large amount of new information, lack of time for social activities and
coping with patients’ illnesses and sometimes deaths, may contribute
to the onset of depressive symptoms in students [8]. Some studies
have shown that medical students present average anxiety levels
above the overall population levels, and their depression scores can
increase during the first year of medical school [9,10]. Problems such
as substance abuse, self-mutilation and suicide were also reported
to be possible consequences of the routine of university students [11]. In this context, among the deleterious effects of the routine of
medical students, poor quality of sleep stands out. Medical students
constitute a group susceptible to sleep deprivation [12], a condition
that can directly affect their learning capacities, their health and their
quality of life. Students inserted in such an academic lifestyle often
end up altering their patterns of sleep-wake cycles [13], and they
hardly have any good sleep hygiene due to their habit of studying
or having leisure time at night, among other factors [14]. Attention
should be drawn to the fact that students, during the process of
learning the medical profession, often neglect themselves. The type
of medical learning process that leaves no room for reflection about
the human being inside the doctor undermines that professional’s
future [15]. Therefore, it is important to learn about quality of life of
these students in order to reduce stress levels and contribute to the
formation of better professionals, with impacts on the doctor-patient
relationship and with greater effectiveness and competence when
serving the population [16].
Hence, the present study aimed to analyze the quality of life and
excessive daytime sleepiness of undergraduate students from Jundiai
School of Medicine This study also aimed to correlate these variables
with possible conditioning factors such as gender, habits and year of
attendance.
Materials and Methods
Subjects:
All Jundiai School of Medicine students were eligible to
participate. The Local Ethics Committee approved all procedures
before enrollment in the study.
Design:
Cross-sectional descriptive study. The study sample consisted of
all undergraduate students of Jundiai School of Medicine, regularly
enrolled from the first to the last year of the medical course (6 years
total), who voluntarily wished to participate in the study and signed the informed consent form. Data collection was carried out during
regular academic activities, always in the beginning of the class period
in the same month. Students who refused to participate in the survey
were excluded from the study, as well as students who were absent on
the days of data collection.
Measurements:
A self-administered questionnaire was provided by the same
applicants M.A.M and C.C.P., with information regarding: gender,
age, year of attendance and questions related to habits, physical
activity and eating patterns. To evaluate quality of life, the World
Health Organization Questionnaire for Quality of Life - Brief Form
(WHOQOL-bref), was used [6]. This questionnaire contains 26
questions, distributed in four domains: physical, psychological,
social and environmental relations. For the evaluation of daytime
sleepiness, the Epworth Sleepiness Scale (ESS) was used [17]. The
ESS is a widely used scale and assesses excessive daytime sleepiness;
it contains eight situations such as the chance of napping while
sitting or reading, and napping while watching television, among
others. The score is marked by the student according to the following
instructions: 0 corresponds to “do not ever doze”; 1 corresponds
to “small chance of dozing”; 2 corresponds to “moderate chance of
dozing”; and 3 corresponds to “high chance of dozing”. The score
indicated by the student in all situations investigated is summed up.
Overall scores from zero to nine points indicate absence of sleepiness;
scores from 10 and 16 points indicate mild sleepiness; scores from 17
to 20 points indicate moderate sleepiness; scores from 21 to 24 points
indicate severe somnolence [17]. For all instruments, language used
was Brazilian Portuguese.
Statistical analysis:
For continuous variables normality was tested using the
Kolmogorov-Smirnov test. To compare participants among
the groups, we used independent samples Student’s T-test for
quantitative variables (as normality was attended), and chi-square test
for categorical variables followed by One Way ANOVA to evaluate
potential influence of year of attendance, sex, healthy habits, physical
activity, alcohol and stimulants use. For correlations, the Sperman’s
correlation test was used. The level of significance was set at 0.05. The
software Statistical Package for the Social Sciences (SPSS) version
20.0 was used to perform statistical analyses.
Results
The sample included 266 medical students (62.0% of attending
students).Their average age was 23.2±2.8 years old, and 62% were
female. Among these students, 71% declared themselves to be regular
practitioners of physical activity, 6.3% were smokers, 72.5% made
regular use of alcoholic beverages, 57% considered their health habits
unhealthy and 12.8% referred using caffeine stimulants regularly
(Table 1).
According to the ESS, excessive daytime sleepiness (scores above
9) was found in 66% of the students, and 14% of the students had
moderate to severe sleepiness (scores above 16). There was a negative
correlation of ESS and WHOQOL-bref total (r=-0.338; p<0.001), that
is, the greatest the daytime sleepiness, the worst the quality of life.
Similar results were found for each of the WHOQOL-bref domains: physical (r=-0.395; p<0.001), psychological (r=-0.179; p=0.003),
social relationships (r=-0.129; p=0.035), and environment (r=-0.247;
p<0.001). ESS scores were greater among women (p=0.006)and
amongst those that stated having regular use of alcoholic beverages
(p=0.002) (Table 2). No difference was found according to year of
attendance and other habits for the ESS scores. No difference was
found in WHOQOL-bref total score regarding year of attendance
and gender. WHOQOL-breftotal score was lower in students that
considered themselves as having unhealthy habits (considered
globally as either smoking, having regular heavy use of alcohol or
caffeine stimulants or being sedentary)(p<0.001). More specifically,
WHOQOL-breftotal score was lower in those having regular use of
alcohol (0.015) and greater in those who practiced regular physical
activity (p<0.001). Similar results were found for the relationship
of the WHOQOL-bref domains (physical, psychological, social
relationships and environment) with gender, unhealthy habits,
practice of physical activity, smoking, and for usual intake of
caffeine stimulants. No relationship was found for WHOQOL-bref
psychological and social relationships domains and usual intake
of alcoholic beverages, but it was found for the physical domain
(p<0.001) - an inverse relationship, similarly to the total score. Finally,
in the social relationships domain there was a difference according to
the attending year (p=0.004), with decreasing values from the first
year to the last year. Students that considered that their eating habits
got worse after they started attending medical school had lower scores
on WHOQOL-bref total score (p=0.018), but no difference was found
in ESS scores.
Discussion
Students of Jundiai School of Medicine had high prevalence of
inappropriate sleepiness, reported by 66% of the sample. There was a
significant difference between genders, with higher sleepiness scores
among women. No differences were found according to year of
attendance. There was an inverse correlation between inappropriate
daytime sleepiness and quality of life specially its physical and
environment domains. On the other hand, students with healthier
habits and with regular physical activity had better quality of life.
Finally, there were a few differences in WHOQOL-bref social
relationships domain among the years, with decreasing values from
the first to the last years. The WHOQOL is a widely used instrument in
scientific research. In a 2010 cross-sectional study carried out with 370
medical students from the city of Recife in Brazil, there was a decrease
in the WHOQOL-bref psychological domain among students closer
to concluding their medical course, when compared to students
beginning it [10]. In the present study, however, a trend was found only
in the social relationships domain. In this sample of medical students,
71%reported to practice regular physical activity. The inclusion of
physical activity in the curriculum of Jundiai School of Medicine in
the first two years of the course, as well as related facilities provided,
allowing training of various modalities, might have had an impact on
that percentage. Since regular physical activity was related to higher
WHOQOL-bref scores (p<0.001), the habit of regularly practicing
physical activities could contribute to maintaining WHOQOL-bref
scores even in those difficult last years of the course. However, this
hypothesis was not tested due to the cross-sectional design of the
present study. The correlation of physical activities with quality of
life in our study is in agreement with the literature. In a systematic review, higher levels of physical activity were associated with better
perception of quality of life both in healthy adults and in individuals
with different health conditions [18]. Similarly, in a study in Brazil,
active individuals had higher WHOQOL-bref scores in the physical,
psychological and environmental domains [19]. Intervention studies
with a high number of participants (n=1089) during 12 months and
extended for 12 more months also pointed to similar results, with
improvement in quality of life in the intervention group [20]. When
considering the several factors potentially associated with quality of
life, it was also verified that students who stated more healthy habits
presented higher scores in the WHOQOL-bref scores compared to
those who affirmed inappropriate habits (p<0.001). Based on the
definition of the World Health Organization, that quality of life is
“the individual’s perception of their position in life, in the context
of the culture and value systems in which they live and in relation
to their goals, expectations, standards and concerns” [5], this data
could be considered one possible evidence of the reliability of the
instrument used to measure quality of life among medical students,
as it uses the individuals own perception on their reality.
The present study shows, through ESS, inappropriate daytime
sleepiness in 66% the students of Jundiai School of Medicine, far above
the average of epidemiological studies in Brazilians. As an illustration,
studies in adult populations the prevalence of inappropriate daytime
sleepiness was 22% [21], and 19% [22]. Our results of high prevalence of inappropriate daytime sleepiness are in accordance with other studies with medical students. Excessive daytime sleepiness in was found in 52% of 276 students (academics and residents) and
the average scores in the ESS were 11 [12]. In all attendance years
the levels of sleepiness were high, on average above the cutoff of 9,
without differences amongst the years. One possible explanation for
that could be that different factors contributed to sleepiness across the
years. Concerning the genders, in our study women presented higher
levels of daytime sleepiness (p=0.011).
Once our population of students is young (23 years, on average) it
could be hypothesized that the high rates of excessive daytime sleepiness
observed could be due to be sleep deprivation. As contributing factor
for that, we can mention extensive workload of the medical course,
with full-time activities and night shifts, extracurricular activities, a
high requirement for study, preference of night hours for leisure time
and others. It is also noted that sleep deprivation in medical students,
internship students and even physicians is often seen as inherent in the
profession itself, or even as a symbol of dedication to the profession.
It is known, however, that sleep is a fundamental biological function
in the consolidation of memory and learning, binocular vision,
thermoregulation, conservation and restoration of energy and of the
energy metabolism [23]. For such processes to occur, however, there
must be a good sleep quality [24]. People who sleep poorly tend to
have more morbidities, shorter life expectancy and premature aging
[25]. In addition, in sleep deprivation, symptoms such as malaise,
irritation, fatigue, impaired agility and mental efficiency can be
observed. Excessive daytime sleepiness can affect the performance
of most of the individual’s cognitive domains in the long or short
term, resulting in impairment of attention, concentration and
operational memory [26]. Sleep deprivation in medical students, may
momentarily increase productivity in both studies and care. However,
it can lead to decreased productivity, cognitive deficits, as well as to precipitate some psychiatric disorders. Therefore, sleep deprivation
can compromise general health and quality of life [24]. Among
the implications on cognitive performance is the increase in errors
in activities that demand attention [27], which can translate into a
risk imposed on the medical students themselves, the individuals in
their immediate learning environment, and the patients cared for.
Therefore, the present study reaffirms the possible impact of sleep
impairment on quality of life through the inverse correlation between
scores obtained through the WHOQOL-bref and ESS(r = -0.338).
As complementary observations, a minority of the students
(6.3%) reported the use of tobacco, but a considerable portion
(72.5%) made customary use of alcoholic beverages. These data are
in line with other studies that evidence alcohol abuse among health
students [28-30].
The present study has several limitations that should be taken into
account. Some students did not participate, especially in the last years
of the course. This was due to difficulties in data collection, especially
with regards to students in the last two years of the course that have
activities at different times and places. Another important limitation
is the cross-sectional nature of the study. We used a validated
Brazilian Portuguese version of the questionnaires the World Health
Organization Quality of Life assessment (WHOQOL-bref) and the
Epworth Sleepiness Scale (ESS). For other variables such as gender,
year of attendance, regular physical activities, smoking, regular use of
alcoholic beverages or stimulants and “unhealthy habits” we did not
use a validated scale and therefore the results of these variables should
be interpreted taking into consideration these limitations. Future
studies, prospectively collecting information, could bring greater
reliability concerning the impact of the course would on quality of
life and sleepiness, with special emphasis on gender differences for
sleepiness that was evidenced in our study. Other variables that could
influence quality of life and sleepiness, such as affective disorders and
cognitive deficits, as well as sleeping and food habits could be also
more thoroughly explored in future studies.
Finally, continuing studies which may contribute with data
on the reality of medical students should be granted. Such studies
may direct faculties to seek strategies for both curricular reforms
and intervention programs in the physical, mental health and sleep
hygiene of students, as well as to opening space for discussion on
the subject as well as raising students’ awareness of the subject.
Such measures can minimize the wear and tear suffered before the
diploma. It is worth highlighting intervention studies with positive
results on psychological distress and quality of life [31]. Among
coping strategies, valuing interpersonal relationships and everyday
phenomena, balancing between study and leisure, organizing time,
health care, s and sleep, practicing physical activity, religiosity,
working the personality itself to deal with adverse situations and
seeking psychological assistance should be investigated as potential
sources for improvements in quality of life [16].
The earlier the medical student reflects on his own life and quality
of life, the better the student can contribute to the quality of life of
patients. Furthermore, the medical school must have this concern,
both in the elaboration of its curricular plan and in promoting
psychological and pedagogical support for the student to deal with
needs in academic and professional life.
References
Citation
Lima RP, Brenelli LM, Viana Miguel MA, Dias Pinto CC, Aprahamian I, et al. High Levels of Excessive Daytime Sleepiness among Medical Students is Associated with Worst Quality of Life, and it is Higher among Female Students. J Neurol Psychol. 2020; 8(1): 05.