
Research Article
*Address for Correspondence: Hafizah Che Hassan, Faculty of Nursing, Lincoln University College, Malaysia, E-mail: hafizahche@lincoln.edu.my
Citation: Hassan HC, Poddar S. Effect of Self-Efficacy and Behaviour Changes in Diet on Health Related Quality of Life Among Middle-Aged Women. J Nutri Health. 2017;3(1): 5.
Copyright © 2017 Hassan et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Nutrition and Health | ISSN: 2469-4185 | Volume: 3, Issue: 1
Submission: 13 December, 2016 | Accepted: 18 January, 2017 | Published: 25 January, 2017
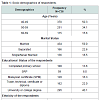 Majority of the participants were Malays (41.3%), followed by Chinese (34.4%), Indians (20.2%) and others (4.1%). The income status of the participant showed that majority (34.9%) had an income of less than 3,000 MYR, followed by 5,001 to 8,000 MYR (26.2%), more than 10,001 MYR (17.9%), and the least income 3,001 to 5000 MYR was received by (8.6%) participant.
Majority of the participants were Malays (41.3%), followed by Chinese (34.4%), Indians (20.2%) and others (4.1%). The income status of the participant showed that majority (34.9%) had an income of less than 3,000 MYR, followed by 5,001 to 8,000 MYR (26.2%), more than 10,001 MYR (17.9%), and the least income 3,001 to 5000 MYR was received by (8.6%) participant.
 Mean scores of health related quality of life (HRQoL) measure by social functioning (SF).
Mean scores of health related quality of life (HRQoL) measure by social functioning (SF).
 The 2 dimension (Physical functional and general health) are above 60% which means the quality of health for the middle aged women is good. Other 6 dimension are below (50%-57%) which means the quality of life is average.
The 2 dimension (Physical functional and general health) are above 60% which means the quality of health for the middle aged women is good. Other 6 dimension are below (50%-57%) which means the quality of life is average.
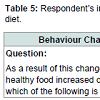
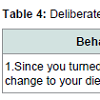 Table 5 shows respondents (76.6%) made small alteration in increasing healthy diet pattern, followed by moderate increase (12.1%) and large increase in their diet pattern was seen among minority of the respondents (10.6%).
Table 5 shows respondents (76.6%) made small alteration in increasing healthy diet pattern, followed by moderate increase (12.1%) and large increase in their diet pattern was seen among minority of the respondents (10.6%).
 Healthy diet consumption
Healthy diet consumption
 Convergent validity
Convergent validity
The second aspect is the composite reliability (CR). It indicates the degree to which a set of items consistently indicate the latent construct [21]. As shown in Table 7 the composite reliability values ranged from 0.88 to 0.98 which exceeds the recommended value of 0.70 [21,23]. Table 7, also presents the Cronbach’s alpha which ranged from 0.81 to 0.98 except General Health (0.57). Even though the Cronbach’s alpha quite low, but the composite reliability of General Health is high and satisfactory (CR=0.82). Thus, in this study composite reliability coefficient was used to determine the internal consistency. This is because, composite reliability is considered to have much less biased estimation as against Cronbach’s alpha coefficient in the sense that Cronbach’s alpha assumes that all items contribute equally to the main construct as against the individual loadings [25] and also, Cronbach’s alpha is considered to be over or under-estimate the scale reliability.
Effect of Self-Efficacy and Behaviour Changes in Diet on Health Related Quality of Life Among Middle-Aged Women
Hafizah Che Hassan* and Sandeep Poddar
- Faculty of Nursing, Lincoln University College, Malaysia
*Address for Correspondence: Hafizah Che Hassan, Faculty of Nursing, Lincoln University College, Malaysia, E-mail: hafizahche@lincoln.edu.my
Citation: Hassan HC, Poddar S. Effect of Self-Efficacy and Behaviour Changes in Diet on Health Related Quality of Life Among Middle-Aged Women. J Nutri Health. 2017;3(1): 5.
Copyright © 2017 Hassan et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Nutrition and Health | ISSN: 2469-4185 | Volume: 3, Issue: 1
Submission: 13 December, 2016 | Accepted: 18 January, 2017 | Published: 25 January, 2017
Introduction
In the present times the main cause of mortality worldwide are diseases that could be prevented with appropriate nutrition, regular physical exercise, and a healthy lifestyle that comprises of leisure time, stress management, and personal and environmental care [1]. Self efficacy is ones belief in his or her abilty to complete a future task or solve a future problem [2]. According to Luszczynska and schwarzer self-efficay is one’s in one’s ability to succeed in specific conditions and also supported [3]. Omrad also define that selfefficacy as the extend or strength of ones belief in one’s own ability to completed task and reach goals [4]. This study has shown an impact to behaviour change. Self-efficacy correlates positively with success in all areas of personal endeavour, and it can help overweight patients become more self-reliant [5]. The tools used for this study was short form health survey questionnaire (SF36). The theory used was Social Cognitive Theory and Self-efficacy by Bandurs [6]. Self-efficacy play a major role in behaviour changes on each individual especially in maintaining healthy diet in approching to goals, tasks and challenges. Therefore choosing the right food and cutting a few hundred calories a day from our diet, can increase the chances to live longer with a more prolific life [7]. Studies on elderly have now created interest among researchers and a lot of attention has been given to studies pertaining to nutrient intake among this special group. Progressive decline in energy, lean body mass and protein intake are also associated with aging [8].There have been numerous nutritional and health status studies in Malaysia among the young adults and the elderly [9,10]. A study has shown that lifestyle changes related to unhealthy eating habits, socio-economic pressure, smoking and decreased physical activity are risk factors of chronic diseases [10]. Being older, significantly being 50 years and above among Malay or Indian descent will increase the risk of mortality and morbidity rate from cardiovascular diseases [11-14]. The NHMS 2 established that 30% of these adults suffered from high blood pressure (140/90), 7% showed glucose levels more than 11. Of the total population 20% had cholesterol above 6.2 mmol/L [15]. Another study carried out by Khor in the early 1990s (1991) indicated that death caused by cardiovascular diseases was twice as much higher among the Indians compared to Malays and Chinese [13].
However, there is still a lack of studies on middle-aged adults, between 40 to 60 years old particularly among women. Although not many surveys on nutrient intake have been carried out in Malaysia, the results obtained from limited studies indicated that cases of deficiencies among elderly do exist in the country [16].
Thus this study was carried out to focus on this age group and to determine the nutritional status of this age group. The present study will provide an idea about the nutritional knowledge and health status among middle-aged women in Malaysia considering the sociodemographic and economic parameter.
Materials and Method
The current study is a mixed method cross sectional survey study conducted in Malaysia on a total of 736 subjects among which 29 were from the urban area, 32 from semi-urban and 39 from the rural area. The majority of the subjects (47%) completed secondary education, 21% had no proper education, and 19% attended school up to primary level while 13% obtained tertiary education. Gender distribution with regard to education attainment was quite skewed towards minimum education among women; in that one-third of the women (33%) never attended school and another one-fifth (21%) attained only primary school education. This study, reflected that education among women in urban and semi urban areas was at least better off than their counterparts in the rural area.This research follows the ethical consideration as led by Declaration of Helsinki [17]. Informed consent was taken from each of the participant to participate in this study. A questionnaire survey methodology was administered by simple random sampling. The inclusion criteria involved middle aged women between the ages of 40-65 years old of Malaysian origin. The targeted sample size was 1,000 respondents in the current research; a simple random sampling technique was used in collecting the data from the population. Before the distribution of questionnaires among the targeted participants, a pilot study was conducted as described by Creswell [18]. The survey questionnaire consists of section A and section B. Section A consisted of consists social-demographic question. Section B consist of 11 question on diet self-efficacy, behaviour changes on diet and consumption of healthy food.
In this research, a pilot study was conducted to validate the instrument before administering the survey to the participants. Internal reliability of SF-36 and Self-efficacy Construct (N=25) was tested for Cronbach’s Alpha majority of the 8 dimension were having: Bodily Pain (0.95) General Health (0.96) Mental Health (0.89) Physical Functioning (0.94) Role Limit due to emotional problem (0.92) Role Limit due to Physical Health (0.97) Vitality (0.89) except for social functioning (0.53).
After the data was collected, this study utilized SMART PLS path modelling [19] and Smart PLS 2.0 M3 software was used to analyse the data [20]. Other statistical package like SPSS (Statistical Package for the Social Sciences) was also employed in the analysis. Thus in this present study mixed research methodology was used to investigate the quality of life among middle aged women. With consideration of data collection and analysis, the present study adopted cross sectional research design and quantitative methods with simple random sampling. The qualitative sampling was by purposeful or non-random selection and selection of the respondents was by willingness to be interviewed.
Results
The findings are divided into two phases. The first phase is on the quantitative analysis and findings and the second phase is on the qualitative interview data analysis and findings.Descriptive analyses of socio-demographic of respondents
A total of 736 respondents completed and replied the questionnaire. Table 1 summaries the data pertaining to respondent’s background information. The data shows respondent’s age, marital status education, race, employment status and monthly income. Table 1 shows that all participants were female, where majority of the female (50.3%) fall in the age group of 40-49 years old, followed by 50 years to 59 years (34.1%), and 60 years to 69 years (15.6%). In terms of marital status of the participants, (59.0%) were married; followed by separated (22.6%) while the number for single and never married was (18.5%). The occupational qualification of the participants, revealed that majority of the participants (40.1%) had a degree from university while (22%) had attained college qualification, technical certificate or diploma, and (13.6%) had completed primary school. The number of participants who had completed lower certificate of education (SRP) was (8.1%).
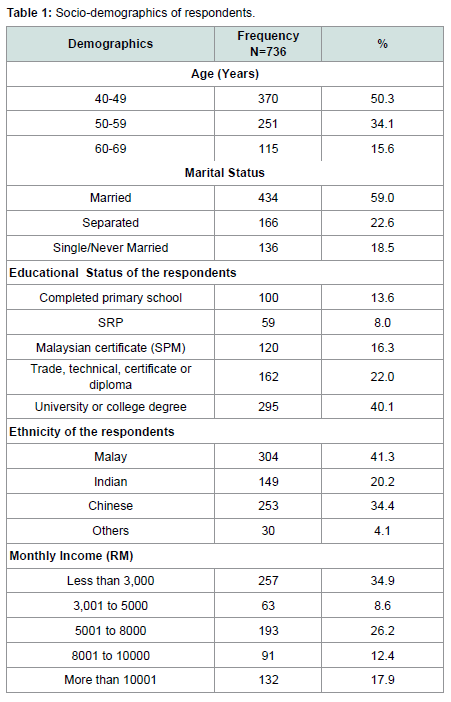
Table 1: Socio-demographics of respondents.
Status of BMI
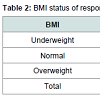
Table 2, illustrates BMI (weight and height) of the respondents. The height and weight is critical in informing the BMI of the respondents. Majority have a normal BMI of (86.4%), underweight was (4.1%) and overweight was only (9.5%). From the data it can be concluded that majority of them had normal body weight and none of them were obese.
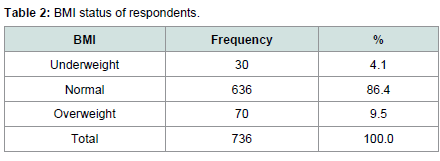
Table 2: BMI status of respondents
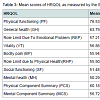
Table 3 shows the general overview of the level of HRQoL of the entire respondent. Mean SF scores for the population (n=736) Physical function (76.53) General health (63.79) Role Limit due to Emotional Problem (57.21) Vitality (56.86) Bodily pain (55.94) Role Limit due to Physical Health (55.50) Social functioning (51.48) Mental health (50.29).
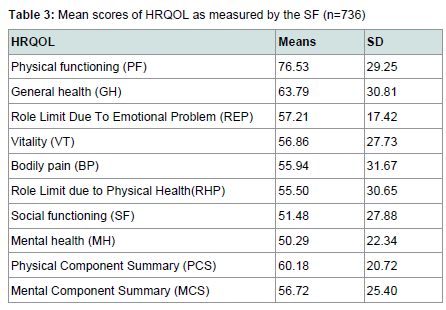
Table 3: Mean scores of HRQOL as measured by the SF (n=736).
Physical Component Summary is (60.18) higher than Mental Component Summary (56.72) which indicates that a middle age women’s mental health problem is lower than physical health problem.
This Table 4 explains health behavioral changes in diet pattern among the respondents. A deliberate change on healthy eating pattern was seen with 37.8%. Majority (62.2%) did not make any changes in their diet pattern.
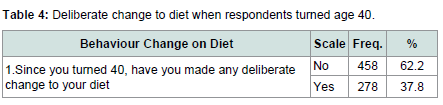
Table 4: Deliberate change to diet when respondents turned age 40.
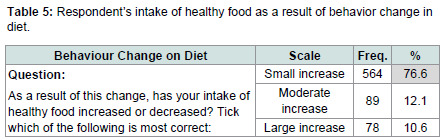
Table 5: Respondent’s intake of healthy food as a result of behavior change in diet.
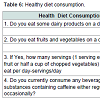
Table 6 also showed the majority of middle aged women consumed dairy product daily (87.1%); 48.5% took 1 fruit serving three times a day, and 43.3% selected a fruit daily. 72.6% of respondents did not consume much beverages containing caffeine.
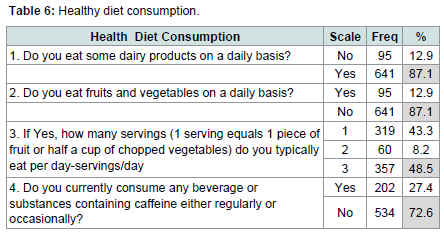
Table 6: Healthy diet consumption.
Hair et al. proposed that in order to establish the convergent validity, it involves the main three aspects namely, factor loadings, Composite Reliability (CR) and Average Variance Extracted (AVE) [21]. The first aspect to achieve the convergent validity is if the items loadings were examined and all the items have loadings more than 0.50 which is the acceptable level suggested in the multivariate analysis literature [21-13]. However, as a general rule of thumb,the item loading is interpreted as poor when it is less than 0.30, fair between 0.31-0.50, moderate between 0.51-0.60, moderately strong between 0.61-0.80 and very strong between 0.81-1.0 [24].
In the present study, the measurement of SF constructs (first, second and third order constructs), self-efficacy on exercise and selfefficacy on diet shows that all the item loadings of the construct and their loadings are all within the threshold of 0.63 and above (Table 7). Therefore it can be concluded that the factor loadings of all the constructs achieved the recommended value of convergent validity.
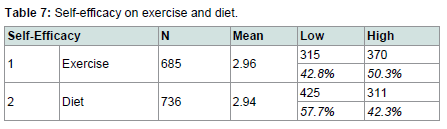
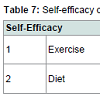
Table 7: Self-efficacy on exercise and diet.
The last aspect to establish the convergent validity is examination of the values of the average variance extracted (AVE). Several scholars suggested that the AVE value more than 0.50. In this study the constructs achieved the values more than 0.50 that performing a good level of construct validity of the measures were used [21,23,26].
Self-efficacy on exercise and diet
The survey tool used to measure self efficacy on exercise and diet was SF36. Table 7 showed self-efficacy for exercise and self-efficacy for diet. In comparison between self-efficacy for exercise and selfefficacy for diet it is divided into two categories comprises of low and high category. In self-efficacy for the high category showed there was an increase in self-efficacy for exercise (50.3%) compared to diet (42.3%) In the lower category, it showed an increase in diet (57.7%) compared to exercise (42.8%).
Cross loadings of SF36, Self-Efficacy on Diet and Exercise constructs. The content validity of the constructs was performed in two modes [24]. First, the items showed high loading on their respective constructs when compared to other constructs. Second, the items loadings were significantly loading on their respective constructs confirming the content validity of the measures used in the present study. Several items were deleted because of low loading in their respective construct.
The current study proposes a theoretical relationship between behavior changes on for diet and health related QOL (which is a formative construct). Hence PLS algorithm was applied to ascertain the nomological validity of the formative construct behavioral change on exercise and behavior change on diet. The results demonstrated that behavioral change on exercise has a strong and highly significant impact on Health Related QOL (Beta=0.460, t=15.648, p< 0.001) and hence, external validity was established. In this Table 7 also shows behavioral change on exercise and behavior change on diet has a significant impact on Health Related QOL (Beta=0.322, t=9.810, p< 0.05).
Discussion
Generally, the demography data of middle aged women affects health related quality of life such as body mass index (BMI), age, marital status, education, income and ethnicity. These demographics can be helpful in achieving a health related QOL. Of the 736 middle aged women respondent, 312 (n) were having normal BMI, majority have normal BMI (86.4%), under the category of underweight was (4.1%) and for overweight was only (9.5%). However, during the interview it was observed and the data collected about (20.8%) were found to be obese. Thus, this showed that the respondents maybe reluctant to give accurate information about their weights as this is a very sensitive issue and the BMI do not reflect their actual BMI. But for qualitative result out of 24 middle aged women who had been interviewed it was found that majority have normal BMI (46.7%) followed by overweight is (37.5%) and obese (20.8%). Observation during interview and data collected showed that some respondents were in the category of obesity.A research in a rural Malay community in Raub also reported a high proportion of the women (72%) as housewives [27,28]. Anthropometry the physical features of the subjects, there was a major difference between the sexes for weight, height and Weight Height Ratio (WHR); though no significant difference was observed for BMI. Mean body mass index (BMI) was 27.2±4.2 kg/m2 for men and 27.0±5.2 kg/m2 for women, and this displays that on average subjects in this study were overweight.
Further analysis of BMI showed 2% of men and women were underweight, while 24% of men and 35% of women had normal body weight. The prevalence of overweight was 51% among men and 35% among women, while obesity was present in 22% of men and 27% of women. However, the prevalence of overweight and obesity was higher than in a Malay community in the rural setting and inthe urban area [27,28]. Although the number of subjects in this study was small and the age of the subjects was older than the study of Ismail et al. and Norimah et al. this study means that overweight and obesity could be a potential health problem among adults in this age group and that this problem should be addressed accordingly [27-29]. Thus adults, especially those within the studied age group, should be more prudent about their nutritional and health care to ensure that the development and progression of chronic diseases is constrained. In this study, this is a clear indication that nutrition and health awareness should be reviewed.
Sharkawi et al. did a study on the factors perceived to be important barriers to healthy eating among Malaysian adults. Findings showed that perceived barriers domain revealed four factors that accounted for variance in perceived barriers to healthy eating, namely: physical; knowledge and social; lack of time; and unavailable healthy choices. The findings of this study implied the needs for provision of wide selection and availability of healthy food to the consumers as well as promoting the nutrition and healthy eating messages effectively [2]. Another study suggested that physical aspects of the healthy food such as price, preparation time of food and sensual appeal of the food including taste, perishability and the ability to satisfy hunger were the perceived barriers in preventing Malaysians from eating healthily. These barriers were in accordance with other findings from previous studies [30].
In this study it was found that middle age women with high selfefficacy for diet are more likely to make a positive modification in their dietary behavior and to have high health related QOL is rejected where 253.5 and p=0.000 is significant. Mostly the reason for the women to change their habit for diet is due to doctor’s advice, medical problems and to be healthy, having better life style, to keep slim.
The influence of education on dietary behavior
Thiele et al., Boynton et al. and Saavedra et al. identified that education play a vital role in relation to exercise and diet. It was confirmed in this current study that woman with higher education levels were more likely to make a positive changes in their diet during midlife [31-33]. Since education was also shown to be linked with BMI and exercise self-efficacy, it seems that women with lower education levels are more likely to be overweight or obese compared to women with more education, as they are less likely to believe that they can eat healthy diet or do regular exercise. The study suggested that when a woman is dealing with a range of variables that could impact self-efficacy (e.g. low education level, a high BMI, and poor mental health) it may be extremely difficult for her to adopt positive health behaviors. The education considering the dietary habits needs to be considered in health promotion programs targeting women. It also implies that overweight and obese girls who leave school at a young age are at risk of moving down a path that could lead to chronic disease later in life [22].
Since most women preferred making dietary changes to exercising more, perhaps lifestyle modification programs need to start with food and encourage women to exercise to support their dietary initiative. The findings from this study suggest that an effective way to encourage women to develop new habits is to develop routines and to make modifications to their existing behaviors. The findings and the discussion look like that the researchers findings are related to the theory that have been discussed by the researcher such as Social Cognitive theory, Bandura learning theory, Health belief model and self-efficacy and many others [34]. The findings are relevant to the culture of people in Malaysia and it can be adapted to any other studies that need to be done in Malaysia.
Acknowledgements
The authors are thankful to the Management of Lincoln University College to provide necessary support for carry out the work and to all respondants who take part in the research study.References
- Rodrigues LP, Roncada MJ (2008) Educação nutricional no Brasil: evolução e descrição de proposta metodológica para escolas. Com Ciências Saúde 19: 315-322.
- Bandura A (1977) Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 84: 191-215.
- Luszczynska A, Schwarzer R (2005) Social cognitive theory. In: Conner M, Norman P (Eds), Predicting health behavior: Research and practice with social cognition models, (2ndedn). Open University Press, Buckingham, England, pp. 127-169.
- Ormrod JE (2006) Educational psychology: Developing learners (5thedn). Pearson/Merrill Prentice Hall.
- Cochrane G (2008) Role for a sense of self-worth in weight-loss treatments: helping patients develop self-efficacy. Can Fam Physician 54: 543-547.
- Bandura A (2001) Social cognitive theory: an agentic perspective. Annu Rev Psychol 52: 1-26.
- Sharkawi I, Mohamed Z, Rezai G (2014) Healthy eating: the preventive factors among Malaysians. J Econ Bus Manag 2: 257-261.
- Ahmed FE (1992) Effect of nutrition on the health of the elderly. J Am Diet Assoc 92: 1102-1184.
- Karim N, Leong SW (2000) Evaluation of nutritional status among a group of young Chinese adults in Kuala Lumpur, Malaysia. Asia Pac Clin Nutr 9: 82-86.
- Shahar S, Earland J, Rahman SA (2000) Food intakes and habits of rural elderly Malays. Asia Pac Clin Nutr 9: 122-129.
- Lam YL, Khor GL (1997) Faktor risiko di kalangan pesakit jantung koronari di Institut Jantung Negara, Kuala Lumpur. Malays J Nutr 3: 103-106.
- Corrao JM, Bcker RC, Ockene IS, Hamilton GA (1990) Coronary heart disease risk factors in women. Cardiology 77: 8-24.
- Jayamalar R (1991) Coronary artery disease in Malaysia: a perspective. Med J Malaysia 46: 1-6.
- Khor GL (1997) Nutrition and cardiovascular disease: an Asia Pacific perspective. Asia Pac J Clin Nutr 6: 122-142.
- Heng DM, Lee J, Chew SK, Tan BY, Hughes K, et al. (2000) Incidence of ischaemic heart disease and stroke in Chinese, Malays and Indians in Singapore: Singapore Cardiovascular Cohort Study. Ann Acad Med Singapore 29: 231-236.
- Lim GC (2002) Overview of cancer in Malaysia. Jpn J Clin Oncol 32 Suppl: S37-S42.
- Suriah AR (1989) Nutrition of the elderly. Sains Malaysiana 18: 1-15.
- General Assembly of the World Medical Association (2013) World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent 81: 14-18.
- Creswell JW (2012) Educational research: planning, conducting, and evaluating quantitative and qualitative research. Pearson Education, Inc.
- Wold H (1985) Partial least squares. In: Kotz S, Johnson NL (Eds), Encyclopedia of statistical sciences. John Wiley & Sons, New York, 6: 581-591.
- Ringle C, Wende S, Will A (2005) Smart PLS 2.0 (Beta). Hamburg.
- Hair JF Jr, Black WC, Babin BJ, Anderson RE (2010) Multivariate data analysis, (7thedn). Englewood Cliffs: Prentice Hall.
- Anderson R, Anderson D, Hurst C (2010) Modeling factors that influence exercise and dietary change among midlife Australian women: results from the Healthy Aging of Women Study. Maturitas 67: 151-158.
- Fornell C, Larcker DF (1981) Evaluating structural equation models with unobservable variables and measurement error. J Mark Res 18: 39-50.
- Chow WS, Chan LS (2008) Social network and shared goals in organizational knowledge sharing. Inf Manag 45: 24-30.
- Gotz O, Liehr-Gobbers K, Krafft M (2010) Evaluation of structural equation models using the partial leastsquares (PLS) approach. In: Esposito Vinzi V, Chin WW, Henseler J, Wang H (Ed), Handbook of partial least squares: Concepts, methods and applications (Springer Handbooks of Computational Statistics Series). Springer, Heidelberg, Dordrecht, London, New York, pp. 691-711.
- Barclay D, Higgins C, Thompson R (1995) The Partial Least Squares (PLS) approach to causal modeling: personal computer adoption and use an illustration. Technol Stud 2: 285-309.
- Normah AK, Lim FA, Ismail MN, Fatimah A, Khalid Y (1999) Anthropometric and food intake status of a Malay community participating in an intervention project. Proc Malaysian Assoc Stud Obes 3: 28-36.
- Karim NA, Mydenkather H (1999) Nutritional status and food habits of middle-aged adults in selected areas of selangor. Malays J Nutr 9: 125-136.
- Ismail MN Jr, Zawiah H, Chee S, Ng K (1995) Prevalence of obesity and chronic energy deficiency (CED) in adult Malaysians. Malays J Nutr 1: 1-9.
- Eikenberry N, Smith C (2000) Healthful eating: perceptions, motivations, barriers, and promoters in low-income Minnesota communities. J Am Diet Assoc 104: 1158-1161.
- Thiele S, Mensink GB, Beitz R (2004) Determinants of diet quality. Public Health Nutr 7: 29-37.
- Boynton A, Neuhouser ML, Sorensen B, McTiernan A, Ulrich CM (2008) Predictors of diet quality among overweight and obese postmenopausal women. J Am Diet Assoc 108: 125-130.
- Saavedra JM, Torres S, Caro B, Escalante Y, De la Cruz E, et al. (2008) Relationship between health-related fitness and educational and income levels in Spanish women. Public Health 122: 794-800.
- Bandura A (2004) Health promotion by social cognitive means. Health Educ Behav 31: 143-164.