
Research Article
*Address for Correspondence: Sartika RAD, Department of Public Health Nutrition, Faculty of Public Health, Universitas Indonesia, Depok, West Java, Indonesia, Tel: +6221-7863501; E-mail: ratuayu.fkm.ui@gmail.com
Citation: Sartika RAD, Sulistiadi W, Pudjonarti SA, Triyanti, Rustika. Relationship Between Lipoprotein(A) Level and Dietary Intake of Trans and Saturated Fatty Acids in a West Java Province, Indonesia Population. J Nutri Health. 2016;2(2): 4.
Copyright © 2016 Sartika et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Nutrition and Health | ISSN: 2469-4185 | Volume: 2, Issue: 2
Submission: 20 May, 2016 | Accepted: 21 June, 2016 | Published: 01 July, 2016
In this study there was a statistically significant relationship between trans fatty acid intake and Lp(a) level (p< 0.05), but not with saturated fatty acid intake (Table 2). Although not statistically significant, the mean intake of saturated fatty acid tended to be higher in subjects that had Lp(a) levels in the ‘not normal’ category compared to respondents who had normal Lp(a) levels. The small sample size of his study may have been a limiting factor for assessing the relationship between saturated fatty acid and Lp(a) levels.
 In United States diets, animal fats (meat from ruminants and dairy products) are a major source of saturated fatty acids, and, to a lesser extent, trans fatty acids. Meanwhile, the primary sources of trans fatty acids are partially hydrogenated fats that are used to prepare commercially fried and baked products [11]. In Indonesian society, fried food is commonly consumed by both low- and high-income households, and is a main source of trans fatty acid and saturated fatty acid.
In United States diets, animal fats (meat from ruminants and dairy products) are a major source of saturated fatty acids, and, to a lesser extent, trans fatty acids. Meanwhile, the primary sources of trans fatty acids are partially hydrogenated fats that are used to prepare commercially fried and baked products [11]. In Indonesian society, fried food is commonly consumed by both low- and high-income households, and is a main source of trans fatty acid and saturated fatty acid.
Relationship Between Lipoprotein(A) Level and Dietary Intake of Trans and Saturated Fatty Acids in a West Java Province, Indonesia Population
Sartika RAD1*, Sulistiadi W2, Pudjonarti SA1, Triyanti1 and Rustika3
- 1Department of Public Health Nutrition, Faculty of Public Health, Universitas Indonesia, Depok, West Java, Indonesia
- 2Department of Health Services Quality, Faculty of Public Health, Universitas Indonesia, Depok, West Java, Indonesia
- 3National Institute of Health Research and Development, Ministry of Health, Indonesia
*Address for Correspondence: Sartika RAD, Department of Public Health Nutrition, Faculty of Public Health, Universitas Indonesia, Depok, West Java, Indonesia, Tel: +6221-7863501; E-mail: ratuayu.fkm.ui@gmail.com
Citation: Sartika RAD, Sulistiadi W, Pudjonarti SA, Triyanti, Rustika. Relationship Between Lipoprotein(A) Level and Dietary Intake of Trans and Saturated Fatty Acids in a West Java Province, Indonesia Population. J Nutri Health. 2016;2(2): 4.
Copyright © 2016 Sartika et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Nutrition and Health | ISSN: 2469-4185 | Volume: 2, Issue: 2
Submission: 20 May, 2016 | Accepted: 21 June, 2016 | Published: 01 July, 2016
Abstract
In Indonesia, cardiovascular disease (CVD), which can be related to diet, is a major public health problem. Diets high in fat, saturated fatty acids, and trans fatty acids may increase lipoprotein(a) levels. This cross-sectional study examined the mean intake of trans fatty acid and saturated fatty acid in a sample of Indonesian adults, and examined the relationship between fatty acid intake and lipoprotein(a) levels. A total of 149 adults aged 30-55 years living in rural areas (Bogor) and urban areas (Depok) in West Java Province, Indonesia were included. The participants had a mean intake of trans fatty acid and saturated fatty acid that represented 0.37% (rural 0.36% and urban 0.38%) and 14.53% of calories (rural 14.12% and urban 15.21%), respectively. The proportion of subjects showing abnormal lipoprotein(a) levels was 29% (rural 28.6% and urban 30.0%, p>0.05). Moreover, there was a statistically significant association between trans fatty acid intake and lipoprotein(a) levels (p< 0.05), but not for saturated fatty acid intake. In the context of nutrition, diets that are low in trans fatty acid and saturated fatty acid would be beneficial for the prevention of CVD.Keywords
Trans fat; Saturated fat; Lipoprotein(a); Urban; RuralIntroduction
Indonesia is currently facing a double burden in that the threat of infectious disease and rates of non-communicable diseases are both rapidly increasing. For instance, in 2013 Indonesian Basic Health Research showed that the prevalence of stroke in Indonesia was 12.1 per 1,000 in both urban and rural areas, such that stroke is the single most common cause of premature death in Indonesia [1].Lipoprotein(a) or Lp(a) is a low-density lipoprotein-like particle synthesized by the liver that consists of an apolipoprotein B molecule covalently linked to apolipoprotein (a). Lp(a) levels are associated with a risk of future coronary heart disease (CHD) in a broad range of individuals [2]. Although Lp(a) levels can be highly stable throughout the lifespan of an individual, Mensink et al. reported that intake of trans fatty acids elevates serum Lp(a) levels to a greater degree than does saturated fatty acid [3].
The development of several non-communicable diseases can be attributed to dietary factors, including fat intake. Sartika reported that trans fatty acid and saturated fatty acid intake by Indonesian adults represented 0.48% and 14.53%, respectively, of total calories [4]. Meanwhile, fats constitute around 25% of total calories in typical Indonesian diets, and these fats are largely derived from vegetables such that intake of trans fatty acid is only half of the recommended maximum amount. Despite the low intake of animal fats and trans fatty acids, cardiovascular disease (CVD) in Indonesia is increasing and now represents the most common cause of death in Indonesia. Moreover, increasing rates of consumption of atherogenic foods that carry saturated fatty acid and trans fatty acid indicate that the rate of CVD in Indonesia will likely continue to rise. In Indonesia, research on how Lp(a) levels contribute to disease among urban and rural populations has not been done. Thus, the purpose of this study is to determine the mean intake of trans fatty acid and saturated fatty acid and determine the relationship with Lp(a) levels in an Indonesian population.
Materials and Methods
This cross-sectional study was conducted in September 2013 and included adults aged 30-55 years living in selected urban (Depok City) and rural areas (Bogor District) in the West Java province of Indonesia. According to the Central Bureau of Statistics in Indonesia, the proportion of farmers in the urban area was only 25%, whereas the majority of households in rural areas are engaged in farming [5]. Based on study criteria, Mekar Jaya in Depok City (urban area) and the Pabuaran village in the Bogor District (rural area) were selected as the two villages for study. In each area, 50 households were randomly selected from lists of registered residents provided by the Local People’s Committee. To be included in the study, subjects must have lived in the selected area for more than one (1) year. Residents who were pregnant, using hormonal contraceptives or cholesterol lowering drugs, or who were unwilling to follow the study protocol were excluded. Based on the sample size calculations, the required minimum sample was 180 subjects. Of the 180 selected subjects, 149 met the inclusion criteria and were eligible for this study. The study protocol was carefully explained to all subjects before they provided written informed consent. Ethical clearance was obtained from the Ethics Commitee of the Faculty of Public Health, University Indonesia.Data were collected by the researcher and three trained nutritionists. The subjects were interviewed using a standardized questionnaire (general characteristics), 24 hour food recall, and food frequency questionnaire. Blood samples were collected by two laboratory analysts in the morning after 10-12 hr of fasting and analyzed at the Prodia laboratory in Depok City and Bogor City using ISO-15189:2012(E) standards [6]. Lp(a) levels were assessed by an immunoturbidimetric assay (Advia 1800).The independent variables were trans fatty acids and saturated fatty acid intake. The dependent variable was Lp(a) levels, which were classified as: < 20 mg/dl, normal; 20-30 mg/dl, ’risk of stroke’; and >30 mg/dl, ’risk of CHD’ [7]. Dietary intakes were assessed using 2 x 24 hour recall questionnaires to estimate the mean intake of total calories, carbohydrate, protein, and fat, including saturated fatty acid and trans fatty acid. A food frequency questionnaire was used to measure usual dietary intake frequency and how often study subjects ate given foods (e.g., daily, monthly, or never). Nutrient intake was quantified using an extended version of Nutrient Calculation Software as Indonesian Food Composition database. Total trans fatty acid intake was calculated from fried foods, ruminant products, and margarine/hydrogenated vegetable oil (HVO) products. The content of trans fatty acid from each food group was quantified using a listing of trans fatty acid content in different kinds of food [8] and the Food Balance Sheet from the US Department of Agriculture [9].
Descriptive data analysis was undertaken to determine the proportion of categorical data and mean values of continuous data (univariate analysis). Independent sample T-tests with significance level of 0.05% were applied to identify correlations between two variables (bivariate analysis). All analyses were conducted with SPSS for Windows.
Results and Discussion
Dietary saturated fatty acids are derived from animal sources, while trans fatty acids are naturally found in ruminants and dairy products (e.g., milk, butter, cheese). Other sources of trans fatty acids are fried foods and food products containing margarine or hydrogenated vegetable oil (HVO) [10]. Overall, residents of urban areas tended to consume more animal proteins and fried foods that are in higher saturated fatty acid and trans fatty acid than did residents of rural areas. However, the rural and urban populations had similar saturated fat intake, which represented more than 10% of total calories and thus exceeded American Heart Association (AHA) recommendations that saturated fat intake be limited to < 7% of total calories [11]. Notably, each additional one percent increase in saturated fatty acid intake is associated with an increase in trans fatty acid intake that amounts to 0.03% of calories [8].The total fat intake differed between the two study areas. Fat consumption is substantially related to socio-economic status, and residents of urban areas tend to have higher incomes relative to those living in rural areas. In general, middle to high-income households tend to consume higher amounts of ruminant products and margarine that have higher levels of both saturated fat and trans fatty acids.
This study found that trans fatty acid intake was 0.36% (minmax 0.22-0.75%) and 0.38% (min-max 0.24-1.50%) of total calories for residents of rural and urban areas, respectively (p>0.05). Trans fatty acid intake for adults in the European Union was 0.5-1.6% [12], and in the United States, trans fatty acids represented 2-3% of total calories [13]. Total trans fatty acid consumption is highest in North America (3-4 g/d, equivalent to 1.35-1.8% of energy for a 2000-kcal diet), followed by Mediterranean countries (1-3 g/d), while countries in East Asia have the lowest consumption (< 1 g/d, equivalent to < 0.45-1.8% of energy for a 2000-kcal diet) [14].
WHO/FAO guidelines, as well as those developed in Germany, Austria, and Switzerland, indicate that trans fatty acids should constitute less than 1% of total calories, whereas in France and United Kingdom the maximum recommended level is 2% of total calories. The Nordic Nutrition Recommendations (2004) recommend a maximum intake of 10% total calories of saturated fatty acids and trans fatty acids (calculated as fatty acids) [12]. Typically, these recommendations reflect judgments of the maximum level of trans fat intake that is practically achievable within the context of a nutritionally adequate diet and is based on known patterns of food and nutrient intake by specific populations.
Although there are no national recommendations for trans fats intake in Indonesia, and the trans fatty acid intake measured in this study was still relatively low, this value will likely increase in line with the increase in consumption of saturated fat and thus could be a risk factor for CHD in later life.
Lp(a) is a specific class of lipoprotein particles found in human plasma that acts as a cholesterol carrier in blood circulation. In terms of CVD development, Lp(a) is reportedly more atherogenic than LDL. Moreover, Lp(a) is a definite risk marker for atherosclerotic CVD and is largely thought of as a genetically determined factor that is not affected by the environment [15]. Physiologically and clinically, the atherogenic properties of Lp(a) are manifested when levels exceed 20 mg/dl (risk of stroke and CHD) [6]. Here we found that the mean levels of Lp(a) in urban and rural populations were below the range that induces atherogenic effects (Table 1). Although the mean Lp(a) levels were low among the subjects in this study, the proportion of Coronary Heart Disease (CHD) in Indonesia could increase in the future if Indonesians do not limit fat intake, and particularly intake of saturated fat and trans fatty acids. Although a study by Berglund et al. concluded that there is an interaction between Lp(a) and other CVD risk factors, the physio-pathological role of Lp(a) in CVD remains poorly understood [16].
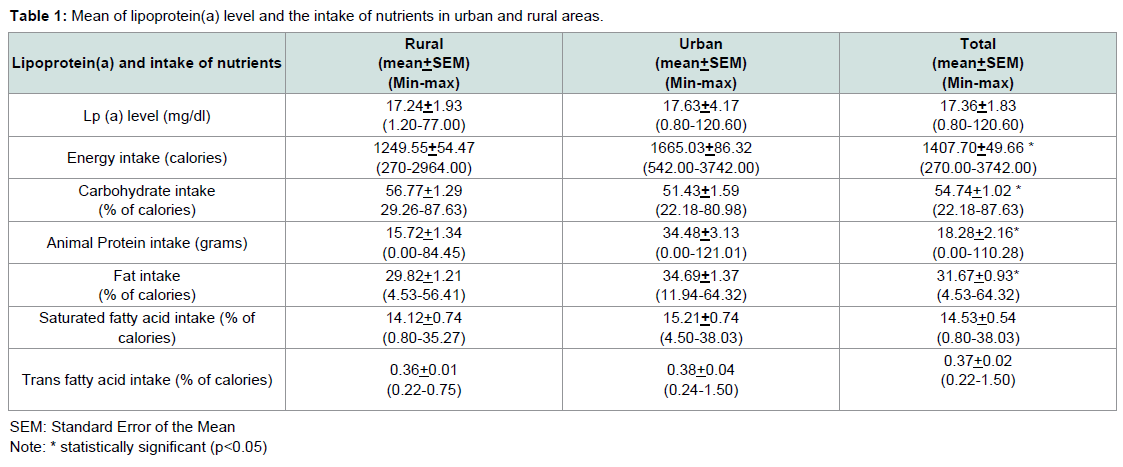
Table 1: Mean of lipoprotein(a) level and the intake of nutrients in urban and rural areas.

Table 2: Association between trans and saturated fatty acid intake and Lp(a) level.
Almost all lipoprotein disorders result from a complex interaction between genetic predisposition and dietary habits. Dietary lipids can play a very important role in development of unfavorable lipoprotein profiles and consequently CHD [17]. Indeed, saturated fatty acids and trans fats are associated with an increased risk of coronary heart disease [11,18]. An excess intake of both saturated fatty acid and trans fatty acid can promote lipotoxicity in several target organs through induction of inflammatory pathway activity that contributes to disease progression in chronic inflammation, atherosclerosis, and heart hypertrophy, as well as other metabolic and degenerative diseases [10].
Research on fatty acids consumed in the diet has focused principally on their role in lipoprotein metabolism, although how trans fatty acids and saturated fatty acids increase Lp(a) is not completely understood at the molecular level. However, evidence that dietary saturated and trans fatty acids generally increase Lp(a) levels forms the basis for recommendations that individuals modify their diets to decrease their intake of saturated and trans fat. Consumption of trans fatty acids can increase levels of Lp(a), which is associated with pro-inflammatory effects and endothelial dysfunction [19,20]. Saturated fatty acids and trans fatty acids are two independent, unrelated fatty acid classes and each exhibits different characteristics and physiological effects as well as metabolic outcomes. As with saturated fatty acid intake, consideration should also be given to the metabolic effect of trans fatty acids and to the synergistic effects of trans fatty acids and saturated fatty acids.
In conclusion, our findings suggest that consumption of trans fatty acids may increase Lp(a) levels. Further research is needed to understand how the consumption of both trans fatty acids and saturated fatty acids increases Lp(a) at the molecular level.
Acknowledgements
This study was financially supported by a grant from the Directorate Research and Public Services-University of Indonesia and all enumerators which supported this studyReferences
- Ministry of Health Indonesia (2013) Basic Health Research (Riskesdas). Jakarta: National Institute Health Research and Development.
- Bennet A, Di Angelantonio E, Erqou S, Eiriksdottir G, Sigurdsson G, et al. (2008) Lipoprotein(a) levels and risk of future coronary heart disease : large-scale prospective data. Arch Intern Med 168: 598-608.
- Mensink RP, Zock PL, Katan MB, Hornstra G (1992) Effect of dietary cis and trans fatty acids on serum lipoprotein(a) levels in humans. J Lipid Res 33: 1493-1501.
- Sartika RA (2011) Dietary trans fatty acids intake and its relation to dyslipidemia in a sample of adults in Depok City, West Java, Indonesia. Malays J Nutri 17: 337-346..
- Central Bureau of Statistics (2007) Statistical year book of Indonesia. Jakarta: BPS - Statistics Indonesia.
- ISO (2012) ISO 15189:2012 - Medical laboratories --requirements for quality and competence.
- Catanzaro JA, Suen R (1996) Clinical laboratory indicators of cardiovascular disease risk. Altern Med Rev 1: 185-194.
- Sartika RA (2011) Effect of trans fatty acids intake on blood lipid profile of workers in East Kalimantan, Indonesia. Mal J Nutr 17: 119-127.
- USDA (2002) USDA Nutrient Database for Standard Reference. US Department of Agriculture Agricultural Research Service.
- Estadella D, da Penha Oller do Nascimento CM, Oyama LM, Ribeiro EB, Damaso AR, et al. (2013) Lipotoxicity: effects of dietary saturated and transfatty acids. Mediators Inflamm 2013: 1-13.
- Lichtenstein AH, Appel LJ, Brands M, Carnethon M, Daniels S, et al. (2006) AHA Scientific Statement - Diet and lifestyle recommendations revision 2006: a scientific statement from the American Heart Association Nutrition Committee. Circulation 114: 82-96.
- EFSA (2010) Scientific opinion of the panel on dietary reference values for fats, including saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids, trans fatty acids, and cholesterol. EFSA J 8: 1461.
- Allison DB, Egan SK, Barraj LM, Caughman C, Infante M, et al. (1999) Estimated intakes of trans fatty and other fatty acids in the US population. J Am Diet Assoc 99: 166-174.
- Craig-Schmidt MC (2006) World-wide consumption of trans fatty acids. Atheroscler Suppl 7: 1-4.
- Jayasinghe R, Craig IH, Mohan RK (2014) Lipoprotein (A) in clinical practice. J Pak Med Assoc 64: 447-450.
- Berglund L, Ramakrishnan R (2004) Lipoprotein(a): an elusive cardiovascular risk factor. Arterioscler Thromb Vasc Biol 24: 2219-2226.
- Ahsan R (2005) Dietary trans fatty acids: impact on serum lipoproteins and coronary heart disease. TAJ: J Teachers Assoc 18: 144-148.
- White B (2009) Dietary fatty acids. Am Fam Physician 80: 345-350.
- Mozaffarian D, Aro A, Willett WC (2009) Health effects of trans-fatty acids: experimental and observational evidence. Eur J Clin Nutr 63 Suppl 2: S5-S21.
- Ramsden CE, Faurot KR, Carrera-Bastos P, Cordain L, De Lorgeril M, et al. (2009) Dietary fat quality and coronary heart disease prevention: a unified theory based on evolutionary, historical, global, and modern perspectives. Curr Treat Options in Cardiovasc Med 11: 289-301.