
Research Article
*Address for Correspondence: SeAnne Safaii, Associate Professor, Family and Consumer Science Department, University of Idaho, Boise 322 E. Front St Ste 180, Boise, ID, 83702, USA, Tel: 208-364-4567; Fax: 208-364-4035; E-mail: sjsafaii@uidaho.edu
Citation: Wright I, Safaii S, Raidl M, Buck JH, Spencer MR, et al. Effectiveness of the Healthy Diabetes Plate and Social Media Project. J Nutri Health.2015;1(2): 6.
Copyright © 2015 Safaii SeAnne et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Nutrition and Health | ISSN: 2469-4185 | Volume: 1, Issue: 2
Submission: 01 September 2015 | Accepted: 05 November 2015 | Published: 09 November 2015
 In 2014, the HDP curriculum was updated to reflect the changes in the American Diabetes Association (ADA) diabetes “plate” and their recommendation that more information was needed on the effectiveness of the “plate” method [5]. In addition, two social media platforms, the Healthy Diabetes Plate Facebook and Pinterest pages, were designed and incorporated into the program to determine if they would provide support and help individuals with their diabetes meal planning skills. The new curriculum was called The Healthy Diabetes Plate & Social Media (HDP & SM) program.
In 2014, the HDP curriculum was updated to reflect the changes in the American Diabetes Association (ADA) diabetes “plate” and their recommendation that more information was needed on the effectiveness of the “plate” method [5]. In addition, two social media platforms, the Healthy Diabetes Plate Facebook and Pinterest pages, were designed and incorporated into the program to determine if they would provide support and help individuals with their diabetes meal planning skills. The new curriculum was called The Healthy Diabetes Plate & Social Media (HDP & SM) program.
The HDP & SM project was approved by the University of Idaho (UI) Institutional Review Board (IRB) in January 2015. Six University of Idaho extension faculties and one Certified Diabetes Educator (in Oregon) were trained on the research protocol and conducted the program in a community or hospital setting from February - June 2015.

Changes in behaviors: Participants completed a pre-survey in week 1 and post-survey in week 7 that measured changes in eating behaviors, self-efficacy, and social media use.

 Statistical analysis
Statistical analysis

 Ability to plan meals
Ability to plan meals
 Changes in diabetes signs and symptoms
Changes in diabetes signs and symptoms
Effectiveness of the Healthy Diabetes Plate and Social Media Project
Isaac Wright1, SeAnne Safaii1*, Martha Raidl1, Julie Harker Buck1, Marnie R. Spencer1, Laura L. Sant1, Rhea Lanting1, Surine Greenway1, Ellie Nagel1, Joey Peutz1 and Nancy C. Deringer2,3*
- 1Family and Consumer Science Department, University of Idaho, USA
- 2St. Alphonsus Hospital, Ontario, USA
*Address for Correspondence: SeAnne Safaii, Associate Professor, Family and Consumer Science Department, University of Idaho, Boise 322 E. Front St Ste 180, Boise, ID, 83702, USA, Tel: 208-364-4567; Fax: 208-364-4035; E-mail: sjsafaii@uidaho.edu
Citation: Wright I, Safaii S, Raidl M, Buck JH, Spencer MR, et al. Effectiveness of the Healthy Diabetes Plate and Social Media Project. J Nutri Health.2015;1(2): 6.
Copyright © 2015 Safaii SeAnne et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Nutrition and Health | ISSN: 2469-4185 | Volume: 1, Issue: 2
Submission: 01 September 2015 | Accepted: 05 November 2015 | Published: 09 November 2015
Abstract
Twenty-eight men and women completed an eight week diabetes meal planning program called the Healthy Diabetes Plate (HDP) and Social Media (SM) Project. It focused on (1) ability to plan meals, (2) eating behaviors and self-efficacy, (3) diabetes signs and symptoms and (4) Facebook and Pinterest. Mixed methods-quantitative and qualitative analyses -were used to analyze the data. Quantitative analysis included frequencies and Pearson’s chi-square analyses. Qualitative analysis included identifying themes from posts on the Healthy Diabetes Plate (HDP) Facebook and Pinterest pages that were created. Participant’s knowledge or ability to plan diabetes meals increased from lesson 1 (79%) to lesson 3 (93%). From pre- to post-study, there was a significant increase in the number of participants who found diabetes meal planning to be easy, and a significant increase in their self-efficacy scores and their ability to eat out at restaurants and purchase foods while still following their diabetes meal plan. Fifty percent of participants participated in the Facebook and Pinterest social media activities. They used it to help them in meal planning (46.4%), finding recipes (28.6%), and (3) assist when dining out (21.4%).Introduction
Type 2 diabetes is a major threat to the public’s health in the United States [1]. According to the 2014 National Diabetes Statistics Report, it is estimated that a total of 29.1 million people in the United States have diabetes or 9.3% of the population [1]. Diabetes self-management (DSM) is multifaceted and requires many lifestyle changes [2] such as weight loss [3], dietary habits and regular exercise [4] to obtain and maintain optimal glycemic control [2]. Diabetes control, achieved through changes in management practices can improve health outcomes and keep people with diabetes healthy [1].Improving an individual’s DSM through education can help them control their blood glucose levels by teaching them about the benefits of exercise, losing weight, if necessary medication use and following a meal plan [1]. Meal planning is one of the most challenging components of diabetes management [5] and out of the many diabetes meal planning tools that do exist such as carbohydrate counting [6], glycemic index [7] and exchange method [8], few target low literacy populations [9]. Understanding basic health information which includes diabetes management is a common problem in the United States where only 12% of the population can obtain, comprehend and process basic health information to make proper health decisions [10].
The Plate Method targets low literacy populations by providing a simple visual approach to learning about diabetes meal planning [11] that enhances understanding [12]. It teaches people the types and amount of foods they should be eating by dividing a plate into the various food groups [13] and has been promoted widely across the country by nutrition educators [14]. It was created for nutrition education purposes and designed to be incorporated into health curriculum resources for a variety of learning styles [14].
For patients with diabetes, social media has been used to improve diabetes control [15] by reducing hemoglobin A1c levels [16]. Social media may also provide support and serve as a venue for individuals to share information, knowledge, connect with others and obtain information [17]. When social media is incorporated into the classroom, individuals use it as a way to remain connected with their instructors and enhance their learning [18].
Therefore the purpose of this study was twofold: (1) to test a plate method curriculum called the Healthy Diabetes Plate on a diabetes population, and (2) to determine if social media is an effective educational tool.
Materials and Methods
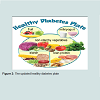
Healthy diabetes plate programThe Healthy Diabetes Plate (HDP), a four-lesson peer-reviewed, evidence based curriculum, targets individuals with type 2 diabetes. It teaches diabetes meal planning skills and was originally published in 2003. Participants attending these classes learned about the diabetes “plate” method, i.e. how five diabetes food groups - vegetables, starches, protein, fruit, and dairy-fit on a plate ( Figure 1). When tested, between 85-99% of participants correctly used this “plate” method to plan their meals in a variety of settings home, grocery store, and eating out [19].
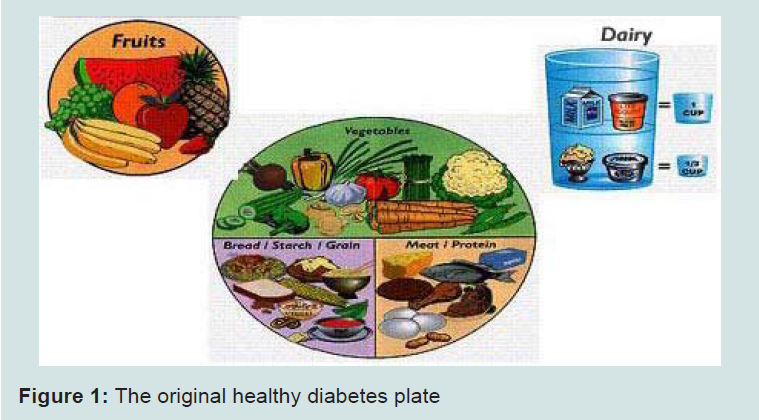
Figure 1: The original healthy diabetes plate
The new HDP & SM program was taught over an eight week period. Participants attended face-to-face classes during weeks 1, 3, 5, and 7 and completed Facebook or Pinterest activities during weeks 2, 4, 6, 8. During the face-to-face classes, participants learned about the signs and symptoms of diabetes, the updated Healthy Diabetes Plate ( Figure 2) which consisted of five food groups-non starchy vegetables, starches, lean protein, fruit, milk/yogurt, how to select foods in the supermarket, cooking tips, and eating out. At each faceto-face class, participants completed meal planning activities. During the social media sessions (weeks 2, 4, 6 and 8) participants completed Facebook and Pinterest activities that reinforced the concepts covered in lessons 1, 3, 5, 7, and posted pictures of meals they consumed.
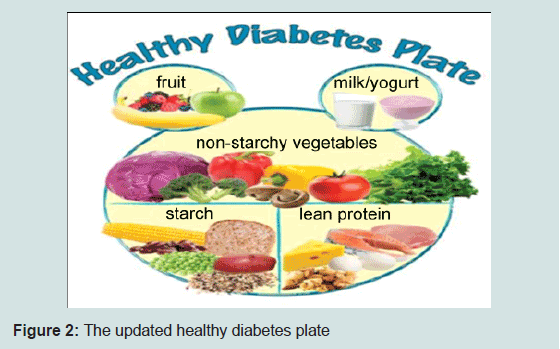
Figure 2: The updated healthy diabetes plate
Participants: A convenience sample of (N=54) adults enrolled in the study and (N=28) completed the study. They were recruited through the University of Idaho extension offices, diabetes support groups, and health care agencies using flyers, radio advertisements and Facebook. Eligibility criteria included being 18 years of age or older, being diagnosed with type 2 diabetes or having a caregiver or friend with diabetes or interest in diabetes meal planning. Classes were offered for free or at minimal cost. All subjects signed a Subject Consent Form at the first class.
Data collection
The HDP & SM program was evaluated using pre- and postsurveys, questionnaires, in-class meal-planning activities, and social media (Facebook and Pinterest) postings. The following types of data were collected:
Demographic and diabetes characteristics: At week 1, participants provided information on age, gender, race and ethnicity, and their diabetes characteristics.
Ability to plan meals: In the four face-to-face classes, participants completed breakfast, lunch, and dinner meal planning “plate” sheets using the five diabetes food groups ( Figure 3).
Figure 3: Example of a breakfast meal planning sheet
Changes in diabetes signs, symptoms: Participants completed a diabetes signs and symptoms questionnaire pre- and post-study which measured change in their diabetes signs and symptoms (Figure 4).
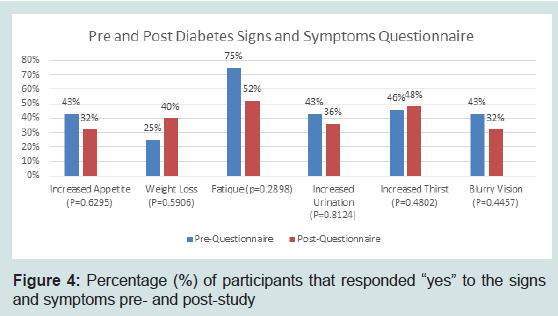
Figure 4: Percentage (%) of participants that responded “yes” to the signs and symptoms pre- and post-study
Facebook and pinterest:Participants’ responses on the HDP Facebook page were organized by themes and analyzed by frequency. For Pinterest, the number of participants were identified that posted recipes to four Pinterest boards; breakfast, lunch, dinner and snacks Figure 5).
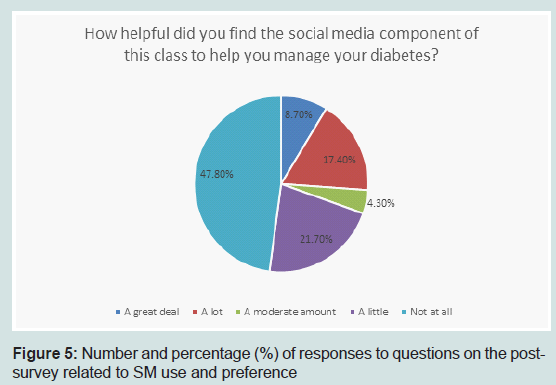
Figure 5: Number and percentage (%) of responses to questions on the postsurvey related to SM use and preference
Mixed methods - quantitative and qualitative analyses-were used to analyze the data. Quantitative analyses included frequencies and Pearson’s chi-square analyses. Frequencies were conducted on demographics and diabetes characteristics of participants, ability to plan meals and diabetes signs and symptoms. Pearson’s chi-square (χ²) analysis was used on questions that had categorical responses which included eating behaviors and self-efficacy; significance was set at an alpha level of ≤ 0.05. Qualitative data was obtained by analyzing the participant themes from the HDP Facebook and Pinterest pages ( Figure 6).
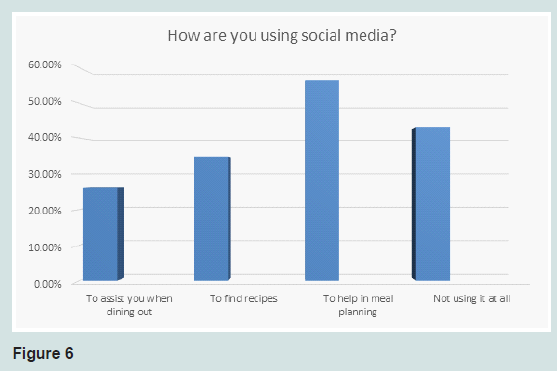
Figure 6: How are you using social media?
Results
Demographic and diabetes characteristics of participants Table 1 shows participants’ age, sex, race, ethnicity diabetes type, length of time with diabetes and diabetes history. Fifty-four individuals started the project, and 28 (52.7%) completed all four lessons. Ages ranged from 21 to 71, however most of the participants (82%) were over 40. From the 28 participants that completed the lessons, 93% were female, 96% were Caucasian and non-Hispanic. Fifty percent of participants had type 2 diabetes, of these, 17.8 % were newly diagnosed (less than one year) and the rest had diabetes from 1-20+ years. The remainders of the participants were either caregivers or friends (14.3%) and 21.4% didn’t have diabetes but were interested in learning about diabetes meal planning. Those who were not diagnosed with diabetes may have had a history of this in their family and wanted to prevent it.
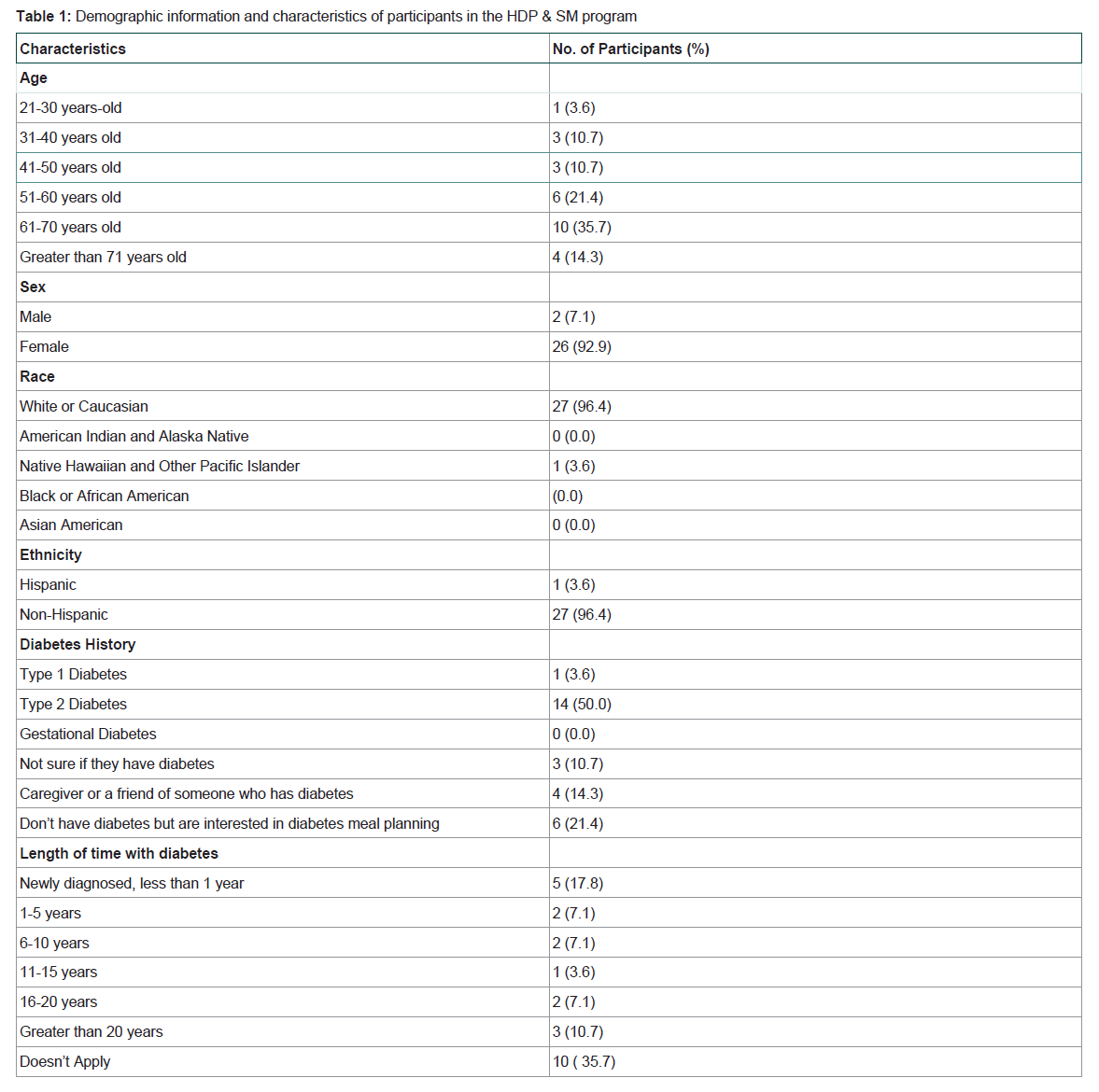
Table 1: Demographic information and characteristics of participants in the HDP & SM program
In lessons 1, 2 and 3, participants completed a Healthy Diabetes Plate meal planning activity that measured their ability to correctly plan meals in three settings - home, grocery store, and eating out. For each setting, participants had to place foods using correct portion sizes into the correct food groups on the plate. The percentage of correct responses for each of the five food groups was then calculated. There was an increase in participants’ knowledge or ability to plan meals from lesson 1 (79%) to lesson 2 (92%) and this knowledge was maintained in lesson 3 (93%). In lesson 1, the percentage of correct responses for the five food groups ranged from approximately 70% (for milk/yogurt, non-starchy vegetables, starch) to 80% (lean protein) and to 91% (fruit). In lesson 2 and 3, for each of the five food groups, approximately 90% of the responses were correct.  Changes in behavior
Changes in behavior
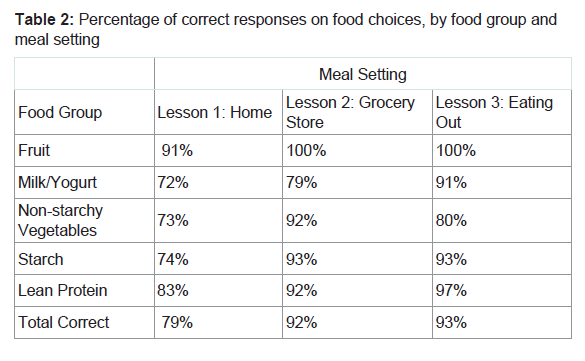
Table 2: Percentage of correct responses on food choices, by food group and meal setting
Table 3 shows the percentage of participants’ pre- and poststudy responses on questions covering eating behaviors and selfefficacy. With an alpha level set at (≤ 0.05) questions 1, 4 and 5 were statistically significant and showed an improvement in scores from pre- to post-test. Question 1 asked participants how difficult it was to follow their diabetes meal plan. It was difficult to interpret this result since 43% of the participants initially did not answer this question. This may have been due to not using a diabetes meal planning tool before the study began. Generally, from pre- to post-, there was a decrease in the number of people who found their diabetes meal planning tool to be difficult and an increase in the number who found it to be easy, which may explain why this was significant (p< 0.03). For question 4 there was a significant improvement (p< . 044) in the number of people that reported being somewhat confident in their ability to eat out at restaurants and following their diabetes meal plan, from 32% to 47%. For question 5 there was a significant (p< 0.03) improvement in the number of people that reported being very confident in their ability to follow a diabetes meal plan, from 21% to 36% and somewhat confident, from 29% to 50 %. Questions 2, 3 and 6 showed an improvement in scores as well, but were not statistically significant. There was no significant change in the number of meals or snacks that they ate or in their level of confidence in preparing recipes and following their diabetes meal plan.
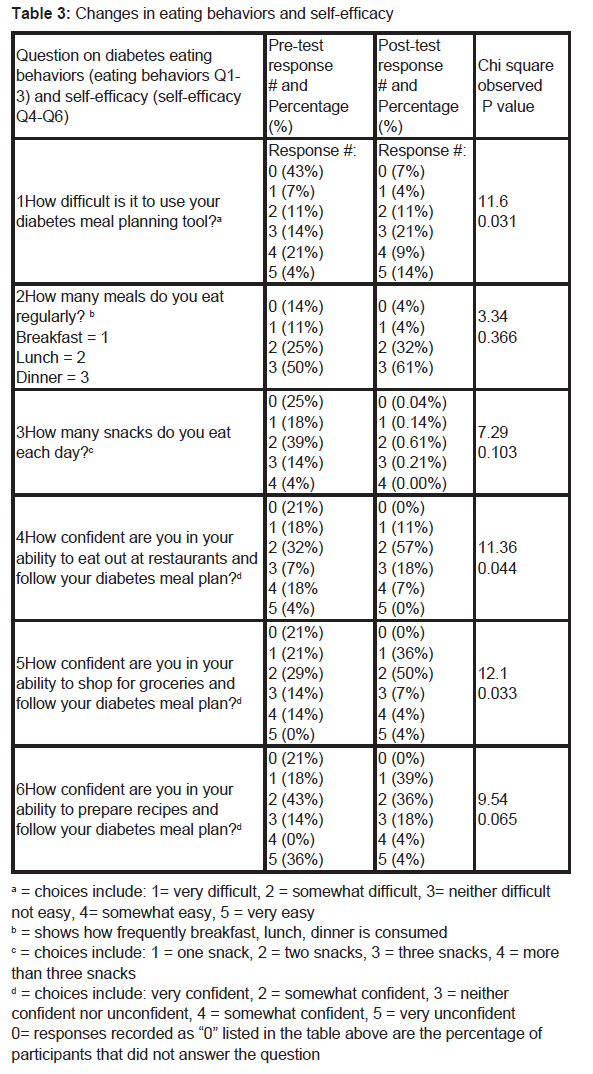
Table 3: Changes in eating behaviors and self-efficacy
The diabetes signs and symptoms that participants were asked to report at week 1 (pre) and week 7 (post) include: increased appetite, weight loss, fatigue, increased urination, increased thirst, and blurry vision. Although participants experiences no significant changes in the aforementioned symptoms from pre-to post-, there was a positive trend towards improvements in appetite, weight loss, fatigue, urination and blurry vision.
Facebook and pinterest results
From the Facebook and Pinterest activities that were offered, 14 individuals (47.8%) chose not to use SM for diabetes meal planning. For those participants that did use SM, they used it to (1) help in meal planning (56.5%), (2) find recipes (34.8%) and (3) assist when dining out (26.1%).
Social media
When considering the amount of participants that began the class (N=54), few (21 total responses) chose to participate in Facebook and Pinterest activities which included questions and activities related to each lesson. For those who did participate, common themes on the Facebook page were identified and related to preparing meals at home (57.1%), followed by diabetes management (19.0%), supermarket activities (14.3%), and signs and symptoms of diabetes (4.8%). Participation in the Pinterest activity was also low where fourteen posted or modified a recipe. However, Pinterest was a positive venue or posting recipes, with 67 breakfasts, 51 lunches, 22 dinners and 1 snack recipe posted.
Discussion
The three components of diabetes self-management are diet (i.e. following a healthful eating pattern), regular physical activity, and often medications [5]. The eight week Healthy Diabetes Plate (HDP) and Social Media (SM) program focused on diet, the most challenging component of diabetes self-management [5]. Overall, it was successful in teaching participants how to plan meals and increase their level of self-efficacy. It was less successful in keeping participants enrolled in the program, having them use social media (Facebook and Pinterest). Although they weren’t statistically significant, slight decreases in diabetes signs and symptoms were noted as observed by participants.The classroom and social media components taught participants how to plan meals in three settings. Results from the classroom meal planning activity showed that 79% to 93% were able to correctly plan breakfast, lunch, and dinner meals based on foods they had at home, foods in the supermarket, and when eating out in a restaurant. These results were similar to other researchers [19] that used the Plate Method for diabetes meal planning activities. Being able to plan meals in a variety of settings indicates that the HDP program is flexible which meets the American Diabetes Association recommendation that diabetes meal plans should not be “one size fits all [20]".
The social media component of the Healthy Diabetes Plate program was designed to reinforce principles covered in the classes. Fifty percent of subjects participated in the social media activities. This low participation rate may be due to the majority of participants being 51 years or older (51%) and most of them not using social media. The corresponds to statistics gathered by the Pew Research Center which found that approximately 46% of Internet users 65 years and older use social networking sites [21]. For those who participated in the social media activities, approximately 60% found them useful and used Facebook and Pinterest mainly to post pictures of HDP meals and share recipes which may have helped them in their classroom meal planning activities.
There was an improvement in participants’ self-efficacy or level of confidence in their ability to eat out at restaurants, shop for groceries and prepare recipes while still following their diabetes meal plan level. Higher self-efficacy has been found to improve diabetes selfmanagement behaviors in diet, exercise, blood sugar testing, and taking medication [22,23].
There were no significant changes in participants’ diabetes signs and symptoms. This is not unexpected since many individuals with type 2 experience very mild signs and symptoms [24].
Limitations
There were several limitations of this study. The first limitation is the composition of the sample. It was small (n=28), a convenience sample, and most of the participants were female and Caucasian. Therefore, it may have not been representative of the type 2 diabetes population and the results may not generalize to them. A second limitation was that attrition rate was high (48%), where several people didn’t finish the ending lessons. A third limitation was low participation in the social media component of the project.Acknowledgements
This material is based upon work that is supported by the National Institute of Food and Agriculture, U.S. Department of Agriculture [Hatch project] under [IDA01430].A special thank you to St. Luke’s Health System in Boise, ID for partially funding this project.References
- CDC (2012) Diabetes report card 2012. Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Atlanta, GA.
- Beverly EA, Wray LA (2010) The role of collective efficacy in exercise adherence: a qualitative study of spousal support and type 2 diabetes management. Health Educ Res 25: 211-223.
- Rejeski WJ, Ip EH, Bertoni AG, Bray GA, Evans G, et al. (2012) Lifestyle change and mobility in obese adults with type 2 diabetes. N Engl J Med 366: 1209-1217.
- Saito T, Watanabe M, Nishida J, Izumi T, Omura M, et al. (2011) Lifestyle modification and prevention of type 2 diabetes in overweight Japanese with impaired fasting glucose levels: a randomized controlled trial. Arch Intern Med 171: 1352-1360.
- Evert AB, Boucher JL, Cypress M, Dunbar SA, Franz MJ, et al. (2014) Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care 6: 3821-3842.
- Laurenzi A, Bolla AM, Panigoni G, Doria V, Uccellatore A, et al. (2011) Effects of carbohydrate counting on glucose control and quality of life over 24 weeks in adult patients with type 1 diabetes on continuous subcutaneous insulin infusion: a randomized, prospective clinical trial (GIOCAR). Diabetes Care 34: 823-827.
- Amano Y, Sugiyama M, Lee JS, Kawakubo K, Mori K, et al. (2007) Glycemic index-based nutritional education improves blood glucose control in Japanese adults: a randomized controlled trial. Diabetes Care 30: 1874-1876.
- Smart C, Aslander-van Vliet E, Waldron S (2009) Nutritional management in children and adolescents with diabetes. Pediatr Diabetes 12: 100-117.
- Kandula NR, Nsiah-Kumi PA, Makoul G, Sager J, Zei CP, et al. (2009) The relationship between health literacy and knowledge improvement after a multimedia type 2 diabetes education program. Patient Educ Couns 75: 321-327.
- Koh HK, Rudd RE (2015) The arc of health literacy. JAMA 314: 1225-1226.
- Proscia A (2014) Patient education. MyPlate for healthy eating with chronic kidney disease (MyPlate education for patients with chronic kidney disease receiving hemodialysis and peritoneal dialysis treatment). J Ren Nutr 24: e23-e25.
- Hersh L, Salzman B, Snyderman D (2015) Health literacy in primary care practice. Am Fam Physician 92: 118-124.
- Camelon KM, Hådell K, Jämsén PT, Ketonen KJ, Kohtamäki HM, et al. (1998) The plate model: a visual method of teaching meal planning. DAIS Project Group. Diabetes Atherosclerosis Intervention Study. J Am Diet Assoc 98: 1155-1158.
- Levine E, Abbatangelo-Gray J, Mobley AR, McLaughlin GR, Herzog J (2012) Evaluating MyPlate: an expanded framework using traditional and nontraditional metrics for assessing health communication campaigns. J Nutr Educ Behav 44: S2-S12.
- Petrovski G, Zivkovic M, Stratrova SS (2015) Social media and diabetes: can Facebook and Skype improve glucose control in patients with type 1 diabetes on pump therapy? One-year experience. Diabetes Care 38: e51-e52.
- Toma T, Athanasiou T, Harling L, Darzi A, Ashrafian H (2014) Online social networking services in the management of patients with diabetes mellitus: systematic review and meta-analysis of randomised controlled trials. Diabetes Res Clin Pract 106: 200-211.
- Cooper A, Kar P (2014) A new dawn: The role of social media in diabetes education. J Diabetes Nurs 18: 68-71.
- Orsini C, Evans P (2015) Social media as a teaching strategy: Opportunities and barriers. Adv Health Professions Educ 1: 44-46.
- Raidl M, Spain K, Hartman-Cunningham M, Lanting R, Lockard M, et al. (2007) The healthy diabetes plate. Prev Chronic Dis 4: A12.
- Brown-Riggs C (2014) Evaluating the new ADA guidelines - There's no one-size-fits-all diet plan. Today’s Dietitian 16: 10.
- (2013) Social Networking Fact Sheet.
- Al-Khawaldeh OA, Al-Hassan MA, Froelicher ES (2012) Self-efficacy, self-management, and glycemic control in adults with type 2 diabetes mellitus. J Diabetes Complications 26: 10-16.
- Mishali M, Omer H, Heymann AD (2010) The importance of measuring self-efficacy in patients with diabetes. Fam Pract 28: 82-87.
- NIDDK (2012) Am I at risk for type 2 diabetes? Taking steps to lower your risk of getting diabetes.