
Case Report
*Address for Correspondence: Laura K. Klug, Department of Pharmacy Practice and Department of Family Medicine, Creighton University School of Medicine 2500 California Plaza, Omaha, NE 68178, USA, E-mail: lauraklug@creighton.edu
Citation: Saxena SK, Spangler ML, Klug LK, Sharma SK. Multiple Sclerosis: A Family Practice Perspective. J Integrative Med Ther. 2014;1(1): 5.
Copyright © 2014 Saxena SK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.Journal of Integrative Medicine & Therapy | ISSN 2378-1343 | Volume: 1, Issue: 1
Submission: 20 February 2014| Accepted: 21 March 2014 | Published: 25 March 2014
Reviewed & Approved by: Dr. Joel G. Anderson, Assistant Professor, School of Nursing, University of Virginia, USA

Etiology
Multiple Sclerosis: A Family Practice Perspective
Shailendra K Saxena1*, Mikayla L Spangler2, Laura K Klug2* and Sanjeev K Sharma1
- 1Department of Family Medicine, Creighton University School of Medicine, 2500 California Plaza Omaha, NE 68178, USA
- 2Department of Pharmacy Practice and Department of Family Medicine Creighton University School of Medicine 2500 California Plaza Omaha, NE 68178, USA
*Address for Correspondence: Laura K. Klug, Department of Pharmacy Practice and Department of Family Medicine, Creighton University School of Medicine 2500 California Plaza, Omaha, NE 68178, USA, E-mail: lauraklug@creighton.edu
Citation: Saxena SK, Spangler ML, Klug LK, Sharma SK. Multiple Sclerosis: A Family Practice Perspective. J Integrative Med Ther. 2014;1(1): 5.
Copyright © 2014 Saxena SK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.Journal of Integrative Medicine & Therapy | ISSN 2378-1343 | Volume: 1, Issue: 1
Submission: 20 February 2014| Accepted: 21 March 2014 | Published: 25 March 2014
Reviewed & Approved by: Dr. Joel G. Anderson, Assistant Professor, School of Nursing, University of Virginia, USA
Abstract
Multiple sclerosis (MS) is a chronic disease that predominately attacks the myelin sheath of the central nervous system. Demyelination occurs often along with scarring at multiple sites throughout the central nervous system. Multiple sclerosis may produce mild symptoms such as numbness, tingling, or changes in writing patterns or other times with severe symptoms such as loss of vision or paralysis. Patients with MS are often seen first by primary care physicians and may have only a few subtle symptoms. The diagnosis of MS made by the primary care physician is done with a high index of suspicion and managed with the aid of neurology consultation. A diagnosis of MS is frightening news to the patient and their loved ones and often provokes a variety of emotional responses. An understanding of these responses can be of tremendous benefit to primary care physicians who are often first to break the news to the patient about the diagnosis. Patient’s thoughts are blocked after hearing this sad news. It becomes the duty of the primary care physician to discuss plans for long term care of the patient considering an integrative and bio-psycho-social approach to care for the individual. Patients and family members should be encouraged to document concerns and instructions to prepare for each medical appointment with any member of their healthcare team.This manuscript discusses MS from a family practice perspective with the case history of a patient who presented with only complaints of difficulty writing and typing with the right hand. An extensive workup proved a diagnosis of MS. The patient was managed in consultation with a neurologist. Care from the primary physician provided the patient not only neurological management but also general medical, psychological, and social needs as well.
Keywords
Multiple sclerosis; Demyelination; Bio-psycho-social model; Family medicine perspectiveAbbreviations
HPI: History of the present illness; ACTH: Adrenocorticotropic hormone; CBC: Complete Blood Count; CMP: Comprehensive Metabolic Profile; CNS: Central Nervous System; CSF: Cerebrospinal Fluid; CT: Computed Tomography; DIS: Dissemination in Space; DIT: Dissemination in Time; EKG: Electrocardiogram; ESR: Erythrocyte Sedimentation rate; HIV: Human Immunodeficiency Virus; IV: Intravenous; MRI: Magnetic Resonance Imaging; OCB: Oligoclonal bands; PSA: Prostate Specific Antigen; TSH: Thyroid Stimulating Hormone; VDRL: Venereal Disease Research Laboratory; PP: Primary Progressive; PR: Progressive Relapsing; RR: Relapsing Remitting; SP: Secondary ProgressiveIntroduction
Multiple Sclerosis (MS) is an autoimmune, inflammatory disease that attacks the myelin of the central nervous system. Pathologically, MS presents with multi-focal areas of demyelination with relative preservation of axons, loss of oligodendrocytes, and astroglial scarring. Here we will review a patient case along with discussion regarding the etiology, presentation, diagnosis and treatment of MS [1].HPI
The patient is a 41 year old white male who presented to his family physician with complaints of difficulty writing and typing with his right hand. He denied any obvious motor or sensory deficits and claimed to have raked his yard fine the day before. However, for the previous week, the patient’s wife had noticed that he had begun to mumble his speech, respond slower to questions, bump into walls in their home, drag his right foot, and sometimes veer the car to the right side of the road. The patient had no significant past medical or family history. He had been married for 21 years in a monogamous relationship with two children, 21 and 19 years old. He did not smoke or use recreational drugs, and ran 3 miles a day. He worked as a manager in the computer industry.
Review of systems
The only pertinent positives in the review of systems were neurological complaints such as deficits in the delivery of speech, writing, and coordinated movements. The patient was able to think of what he wanted to do, but was not able to perform it correctly. For example, he was not able to write in a legible manner or in a straight line.
Physical exam
Neurological findings were limited to a left nystagmus in the right eye, a little swaying in his balance, and a right facial droop. The remainder of his exam was normal.
Assessment and plan
The patient was admitted and had an extensive work up with a differential diagnosis of: 1) cerebral vascular accidents: ischemic vs. hemorrhagic 2) myocardial infarction 3) embolic etiologies 4) neurological disorders. The CMP, CBC, lipid profile, TSH and T4 levels, PSA, and homocysteine levels were all normal. A CT of the head showed hypodensity within the posterior portion of the left internal capsule and within the corona radiate just superior to the anterior horn of the right lateral ventricle. Both were suspicious for ischemic changes with no signs of hemorrhage. Cardiac enzymes, EKG, transthoracic echo, carotid Doppler, VDRL, B12, folate and ESR were all normal. The MRI of the neck was normal; however, the MRI of the head showed a total of 8 multi-focal, white matter lesions that were predominately periventricular in location. These lesions included the ones seen on the earlier CT and one right enhancing lesion.
Progress
At this point, the patient’s facial droop had improved, but he still had difficulty with writing, speaking, and typing. Physical, occupational, and speech therapy were consulted. Motor and sensory functions were still equal and bilateral, but the delivery of fine motor skills was still problematic. Myocardial infarction and embolic phenomenon were ruled out.
Differential diagnosis
Demyelination disorders with white matter involvement such as MS were obviously considered. Toxoplasmosis and HIV are also known to cause ring enhancing lesions. Brain tumors causing white matter lesions particularly primary central nervous lymphoma were of concern due to the rapid onset of the disease and the patient’s young age. Further investigation showed that the toxoplasmosis IgG titers were negative as was the HIV. CSF gram stain, culture, glucose and protein, cytology, MS and lyme profiles were ordered but pending when the patient requested to go home to await results. One week later, the patient was readmitted to the hospital for partial paralysis of the right arm and leg. Motor strength in the right extremities would wax and wane, progressing from weak to complete paralysis. Final CSF results revealed a presence of the IgG Index for MS proteins, a finding commonly seen in 90% of MS patients and suggestive of intrathecal synthesis of CSF immunoglobulins [2]. Oligoclonal bands (OCB) are limited classes of antibodies in 85 to 95% of MS patients [3] and were also positive. The patient was sent home on Solumedrol IV 1000 mg IV over 6 hours for 5 days; one week later, the patient again returned to the hospital, this time with complete paralysis of the right arm.
Epidemiology
The mean age of MS onset is 30 years of age. MS has a higher incidence of occurrence in women than men, and women also tend to have an onset 5 years earlier than men. White populations, especially those from Northern Europe, are more susceptible than Asian, African or American Indian populations. In the United States, the prevalence is 1 per 1,000 (0.1%) with a total of about 250,000 people with MS. Studies suggest smokers have a higher risk for incidence and disease progression than non-smokers
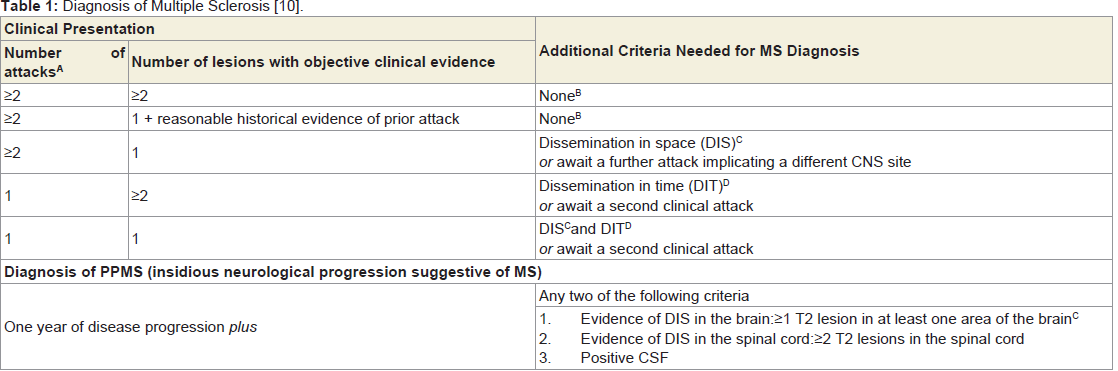
Table 1: Diagnosis of Multiple Sclerosis.A. An attack (aka relapse or exacerbation) is patient-reported or objectively observed events typical of an acute inflammatory demyelinating event in the CNS. Duration must be at least 24 hours without the presence of fever or infection.
B. No additional criteria required, but it is still desirable to confirm the diagnosis with imaging1. Dissemination in space demonstrated by ≥
1 T2 lesion in at least 2 of the following areas of the CNS (excluded if brainstem or spinal cord syndrome) Periventricular
2. Juxtacortical
3. Infratentorial
4. Spinal Cord
C. Dissemination in time demonstrated by
1. A new T2 and/or gadolinium-enhancing lesion(s) on follow-up MRI, with reference to a baseline scan, irrespective of the timing of the baseline MRI
2. Simultaneous presence of asymptomatic gadolinium-enhancing and nonenhancing lesions at any time.
The exact etiology of MS is still unknown. A possible hypothesis includes immune system stimulus with a common type likely being viral infectious stimulus [5]. There are studies that suggest that Epstein Barr Virus may increase the risk for MS [6,7], but there is no conclusive evidence that confirm this hypothesis. Studies have also hypothesized a possible protective benefit from adequate Vitamin D levels [8].
Clinical presentation
MS is difficult to assess due to the variable nature of its manifestations. The most common symptoms are sensory, visual, and motor deficits. When the disease affects the spinothalamic column, posterior column, and dorsal root, patients can feel numbness, tingling, pins-and-needles, tightness, coldness, or swelling of the limbs or trunk. Radicular pains radiating from the lower lumbar region as well as unilateral pruritis in the cervical dermatomes can be presenting symptoms. The most common sensory deficits involve vibration, joint sense, light touch perception in the distal extremities, and patchy areas of reduced pain in the limbs and trunk. Visual deficits may present with optic neuritis or internuclear opthalmoplegia. Optic neuritis is the most common visual deficit and can present as acute or subacute unilateral eye pain exacerbated by ocular movements. Internuclear opthalmoplegia is the delayed adduction or horizontal nystagmus of the abducting eye, which is usually the result of a lesion in the medial longitudinal fasciculus. Motor deficits usually present with paraparesis, paraplegia, spasticity of the lower limbs, and increased deep tendon reflexes. Coordination problems such as gait imbalance, slurred speech, and complex actions with the arms may also occur if the cerebellar pathways are involved. Other features highly characteristic of MS include relapses and remissions, onset between 15 and 50 years of age, Lhermitte’s sign (a transient, sensory shock down limbs or spine with flexion of neck), internuclear opthalmoplegia, and Uhthoff’s phenomenon (a small increase in body temp will worsen symptoms) and fatigue [4].
Types of MS
Multiple sclerosis can be categorized into four types according to its pattern and course: relapsing-remitting (RR), primary-progressive (PP), secondary-progressive (SP), and progressive-relapsing (PR). RRMS is characterized by a clearly defined relapse with a full or partial recovery of symptoms. The disease does not progress between the relapses. PP is characterized by disease progression initially with occasional plateaus and minor improvements of symptoms later on. SP is characterized by RR disease initially, followed with later progression. PR is characterized by progression initially with clear acute relapse and remissions. Progression of disease continues between these relapses. A clinic-based study of 1,100 patients found that at onset 66% had RR disease which in nine years progressed to SP in half of the patients, 19% had PP disease, and 15% had PR disease [8].
The RR form has a better prognosis than the progressive forms. Onset at an early age has a more favorable prognosis than onset at an older age. MS tends to have a more benign course in women than in men. Initial symptoms of sensory and cranial nerve dysfunction, such as optic neuritis, have a favorable prognosis, while symptoms presenting with pyramidal, brain stem, and cerebellar involvement carry a poor prognosis [9].
Diagnosis
MS is a clinical diagnosis based on neuroimaging and clinical presentation. The International Panel on MS Diagnosis revised the McDonald Criteria for diagnosis in 2010 to simplify neuroimaging requirements while still maintaining sensitivity and specificity. MS is diagnosed if criteria are fulfilled as outlined in Table 1. If diagnostic criteria are not completely met, possible MS would be diagnosed. If diagnostic criteria are not met and neuroimaging and other tests such as cerebrospinal fluid analysis are negative, alternative diagnosis need to be explored with extreme caution taken before diagnosing MS [10]. Dissemination of central nervous system (CNS) lesions in both space and time are criteria necessary for diagnosis. These can be based on clinical presentation alone or in combination with MRI findings. MRI is the test of choice to support the clinical diagnosis of MS. MRI lesions characteristic of MS are white matter plaques that involve the periventricular region, corpus callosum, and centrum semiovale. The lesions are typically ovoid in nature, hyperintense on T2-weighted images, and hypointense on T1 weighted images [3]. Patients with MS typically have white matter lesions in 90% of the cases; however, other CNS lesions can present in similar fashion especially ischemic lesions. The sensitivity and specificity depends on the diagnostic criteria implemented. One study showed that criteria involving three areas of increased signal intensity plus two of the following features: lesion next to the lateral ventricle, infratentorial lesion, and size > 5 mm had 96% specificity, 65% positive predictive value, and 81% sensitivity. Gadolinium-DTPA, a paramagnetic contrast agent is utilized to further assess plaque activity [3].
Cerebrospinal fluid (CSF) analysis also can aid in the diagnosis of PPMS [3,10,11]. A common CSF finding is an altered immunoglobulin level, especially IgG relative to other proteins, which suggests intrathecal synthesis of antibodies to MS proteins. A normal IgG index is < 0.66 (may vary slightly depending on lab), and an elevated IgG index is found in 90% of MS patients [1]. Another component of the CSF that is helpful in diagnosis is the oligoclonal bands (OCBs), which are a limited class of antibodies that are depicted as discrete bands on agarose gel. OCBs are found in 85 to 95% of patients with MS; however, chronic CNS infections, viral infections, and neuropathies can also elevate OCBs [2]. The 2010 McDonald criteria note CSF findings only for supporting the diagnosis of PP type of MS [3,10].
Treatment
Advances in disease monitoring and treatment are focused on slowing the progression of MS through immunosuppression. Specific treatment of MS depends upon whether the disease is an acute attack, RR disease or progressive disease. Mild attacks that do not cause functional decline may not require treatment, but if ability is affected, the current treatment is corticosteroids. Short bursts of intravenous (IV) methylprednisolone of 500 mg to 1000 mg daily for 3 to 7 days with or without a prednisone taper are commonly used [12,13]. Oral prednisone of 500 mg per day for 5 days with a 10 day tapering period has also shown a benefit compared to placebo [12-14] without a statistical difference between IV and oral form [12,15]. However, oral methylprednisolone should not be offered to patients with acute optic neuritis, since patients on oral prednisone are more likely to suffer reoccurrences of optic neuritis compared to patients on IV methylprednisolone, who have a quicker recovery of visual loss [16-18]. Adrenocorticotropic hormone (ACTH) is an alternative treatment option for patients who cannot tolerate highdose corticosteroid treatment [12,14].
Treatment of RR disease is focused ondisease modifying therapy. Options include interferon-beta-1b (Betaseron), interferon-beta-1a (Avonex), interferon-beta-1a (Rebif), glatiramer acetate (Copaxone), teriflunomide (Aubagio), dimethyl fumarate (Tecfidera), and natalizumab (Tysabri). Evidence suggests similar clinical benefit J Integrative Med Ther 1(1): 5 (2014) Page - 04 between interferon therapy and glatiramer therapy which are often used as first line treatment options. Natalizumab should be reserved for patients who have failed other therapies due to the risk profile of potentially fatal progressive multifocal leukoencephalopathy (PML). Other immune therapies continue to be investigated for possiblebenefits in patients with MS.
In progressive disease, treatment is focused on chemotherapy agents and irradiation as immunosuppressive therapies [19,20]. Plasma exchange may show some benefit in very rapidly progressive MS [21]. Other therapies such as IV immunoglobulin and bone marrow transplant are still under investigation but are not recommended at this time. Because there are no clear guidelines for the treatment of MS, it is important to discuss with the patient the risks and benefits, available clinical data, route of administration and side effect profile of each treatment and develop a treatment plan in conjunction with the patient. It is imperative that patients understand treatment of MS is not to cure but rather to slow the disease progression [21].
A family practice and integrative approach
In the treatment of MS, it is very important to consider the “Bio-Psycho-Social” aspects of the disease to provide care to the whole person. In addition to the clinical presentation, diagnosis, and treatment options for MS, a physician should also address mental health and lifestyle issues because MS is an inevitable, debilitating disease that can affect all levels of a patient’s health. In this case, the patient was educated about the clinical presentation, diagnosis, and treatment of MS with the most updated information about MS from scientific journals.
It should be made clear to the patient that treatments are aimed to slow the progression of MS and not to cure it. The issue of depression should be addressed with the patient and family. Reassurance that the physician is always willing to discuss these issues helps establish a comfortable rapport.
Through these simple gestures, a physician can provide a positive and realistic perspective that will help the patient psychologically cope with MS. Social aspects should be considered as well. It is very important to establish a support system so that the patient does not feel alone. Family is an appropriate place to start and in this case, the patient’s wife was very willing to provide support. Local MS support groups were also made available to the patient and his wife. Rehabilitation options including physical therapy, occupational therapy, and speech therapy were involved to help the patient adjust to a new lifestyle. Other disciplines to involve in the patient’s care team include mental health specialist such as psychologists and social workers to help the patient with coping and adapting, as well as a nutritionist and a pharmacist to help the patient understand lifestyle changes and medication regimens. Such a comprehensive approach would not be possible without applying the “Bio-Psycho-Social” model of the disease and a team of integrated health care specialists.
Conclusion
MS is a demyelinating, autoimmune disease of the central nervous system that can present in various ways. The four basic clinical courses of MS are RR, PR, SP and PR with the rarest course being PR MS which presents with progressive disease that relapses and remits with progression of the disease between each relapse. This type of presentation only occurs in 15% of the patients with MS [8]. This case is unique for its rapid PR course. The patient first presented with dysgraphia which did not resolve on his first admission. One week later, the patient presented again with partial paralysis of his right arm and leg. The patient’s motor strength in his right arm and leg waxed and waned, demonstrating the RR nature of the disease, with residual symptoms of paralysis.At that time, MS of the PR type began to manifest itself. Later, the patient was again admitted for relapse of his MS. This time he demonstrated complete paralysis of his right arm, further supporting the diagnosis of multiple sclerosis of the PR. In the span of three weeks, the patient’s clinical course rapidly progressed from dysgraphia to partial paralysis to complete paralysis.This case does not outline the most common presentation of a patient with MS, but it highlights the importance of identifying symptoms suggestive of possible MS and an appropriate differential diagnosis and work-up of an uncommon presentation. Primary care physicians need to be aware of these symptoms to consider the possibility of MS in patients like the one presented here. This is an atypical presentation of MS for two reasons: the rapid progression of the disease, and its rare PR clinical course. In a very short period of time, the patient went from running three miles a day to a debilitating state that has changed his life forever. As family practice physicians, it is incumbent on us to be aware of the different clinical presentations of MS, to keep MS in the working differential in a patient presenting with dysgraphia, and to treat the MS patients within the context of the “Bio-Psycho-Social” model.
References
- Olek MJ (2013) Diagnosis of Multiple Sclerosis in adults.
- McLean BM, Luxton RW, Thompson EJ (1990) A study of immunoglobulin G in the cerebrospinal fluid of 1007 patients with suspected neurological disease using isoelectric focusing and the Log IgG-Index. A comparison and diagnostic applications. Brain 113: 1269-1289.
- Rudick RA, Whitaker JN (1987) Cerebrospinal fluid tests for multiple sclerosis. In: Scheinberg P (Ed). Neurology/neurosurgery update series, 7: CPEC, Princeton.
- Olek MJ (2013) Epidemiology and clinical features of multiple sclerosis in adults.
- Hernan MA, Zhang SM, Lipworth L, Olek MJ, Ascherio A (2001) Multiple sclerosis and age at infection with common viruses. Epidemiology 12: 301-306.
- Marrie RA, Wolfson C, Sturkenboom MC, Gout O, Heinzlef O, et al. (2000) Multiple sclerosis and antecedent infections: a case-control study. Neurology 54: 2307-2310.
- Wandinger K, Jabs W, Siekhaus A, Bubel S, Trillenberg P, et al. (2000) Association between clinical disease activity and Epstein-Barr virus reactivation in MS. Neurology 55: 178-184.
- Lublin FD, Reingold SC (1996) Defining the clinical course of multiple sclerosis: results of an international survey. National Multiple Sclerosis Society (USA) Advisory Committee on Clinical Trials of New Agents in Multiple Sclerosis. Neurology 46: 907-911.
- Weinshenker BG (1994) Natural history of multiple sclerosis. Ann neurol 36: S6-S11.
- Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, et al. (2011) Diagnostic Criteria for Multiple Sclerosis: 2010 Revisions to the McDonald Criteria. Ann Neurol 69: 292-302.
- Offenbacher H, Fazekas F, Schmidt R, Freidl W, Flooh E, et al. (1993) Assessment of MRI criteria for a diagnosis of MS. Neurology 43: 905-909.
- Olek MJ (2014) Treatment of acute exacerbations of multiple sclerosis in adults.
- Kupersmith MJ, Kaufman D, Paty DW, Ebers G, McFarland H, et al. (1994) Megadose corticosteroids in multiple sclerosis. Neurology 44: 1-4.
- Berkovich R (2013) Treatment of Acute Relapses in Multiple Sclerosis. Neurotherapeutics 10: 97-105.
- Burton JM, O’Connor PW, Hohol M, Beyene J (2012) Oral versus intravenous steroids for the treatment of relapses in multiple sclerosis. Cochrane Database Syst Rev 12: CD006921.
- Beck RW1, Cleary PA, Anderson MM Jr, Keltner JL, Shults WT, et al. (1992) A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group. N Engl J Med 326: 581-588.
- Beck RW, Cleary PA, Trobe JD, Kaufman DI, Kupersmith MJ, et al. (1993) The effect of corticosteroids for acute optic neuritis on the subsequent development of multiple sclerosis. The Optic Neuritis Study Group. N Engl J Med 329: 1764-1769.
- Beck RW, Cleary PA (1993) Optic neuritis treatment trial. One-year follow-up results. Arch Ophthalmol 111: 773-775.
- Olek MJ (2014) Treatment of relapsing-remitting multiple sclerosis in adults.
- Olek MJ (2013) Treatment of progressive multiple sclerosis in adults.
- Weinshenker BG, O’Brien PC, Petterson TM, Noseworthy JH, Lucchinetti CF, et al. (1999) A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann Neurol 46: 878-886.