
Journal of Hematology & Thrombosis
Large Granular Lymphocytic Leukemia and Cocaine Abuse in A Patient With Chronic Neutropenia - Are They Co-Existing or Causally Related?
Sasapu A2*, Guru Murthy GS1, Insuasti-Beltran G3 and Makhoul I2
- 1Division of Internal Medicine, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA
- 2Division of Hematology/Oncology, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA
- 3Division of Pathology, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA
*Address for Correspondence: Sasapu A, MD, University of Arkansas for Medical Sciences, 4301, West Markham street, Slot 508, Little Rock, AR 72205, USA, E-mail: asasapu@uams.edu
Citation: Sasapu A, Guru Murthy GS, Insuasti-Beltran G, Makhoul I. Large Granular Lymphocytic Leukemia and Cocaine Abuse in A Patient With Chronic Neutropenia - Are They Co-Existing or Causally Related?. J Hematol Thromb 2017;3(1): 2.
Copyright © 2017 Sasapu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology & Thrombosis | ISSN: 2380-6842 | Volume: 3, Issue: 1
Submission: 15 November, 2016 | Accepted: 02 January, 2017 | Published: 09 January, 2017
Abstract
Chronic neutropenia is a hematological condition that could cause significant morbidity due to recurrent infections. Various benign and malignant disorders manifest with chronic neutropenia and a meticulous evaluation is needed. Complex interplay of several mechanisms could lead to neutropenia in the same patient. Hence it is important to understand the disease biology. Substances with abuse potential like cocaine are thought to cause immune mediated destruction of neutrophils. For disorders like large granular lymphocytic leukemia which arises from chronic antigenic stimulation, it is unclear whether agents like cocaine are potential triggering factors. The given case involves a patient with chronic neutropenia for which a complex interplay of cocaine abuse and large granular lymphocytic leukemia is postulated to be responsible for the clinical manifestation, enhancing the insight about the disease pathogenesis.Keywords
Large granular lymphocytic leukemia; Neutropenia; Cocaine; LevamisoleIntroduction
Chronic neutropenia is a hematological condition characterized by low neutrophil count in the peripheral blood (absolute neutrophil count of less than 1500 /microL) for more than 3 months. It can be caused by a variety of benign and malignant disorders. Evaluation of its etiology becomes challenging when there are multiple factors that could be attributed to this condition in the same patient. Some prior reports describe cocaine abuse to be associated with neutropenia and it is postulated that contamination of cocaine with levamisole is responsible for this condition [1]. In this report, we describe an interesting case of chronic neutropenia which was initially thought to be related to cocaine abuse, but on repeat evaluation was found to have large granular lymphocytic (LGL) leukemia. We describe the complex interplay of these factors explaining on how both these etiologies could be potentially causing neutropenia in the given patient.Case Vignette
A 42-year-old African-American woman with history of end stage renal disease on hemodialysis and cocaine abuse was admitted for hyperkalemia and hypertensive emergency. On initial evaluation, she was noted to have severe neutropenia with an absolute neutrophil count (ANC) of zero. Her rest of the blood counts was with in normal limits. Review of her previous records suggested that the neutropenia was present for more than 2 years with fluctuations in the neutrophil counts over different periods of time (Figure 1A). Prior evaluation (in 2010) with complete hematological workup including bone marrow examination did not reveal any specific etiology for neutropenia. Since the patient had a history of cocaine abuse and other workup was negative in the past, it was thought that the neutropenia was related to cocaine abuse as it improved during periods of cocaine abstinence. During this current presentation, the patient was noted to be febrile with no focal findings on physical exam such as hepatosplenomegaly or lymphadenopathy. She was started on medical therapy for hyperkalemia, hypertension, and antibiotics for febrile neutropenia.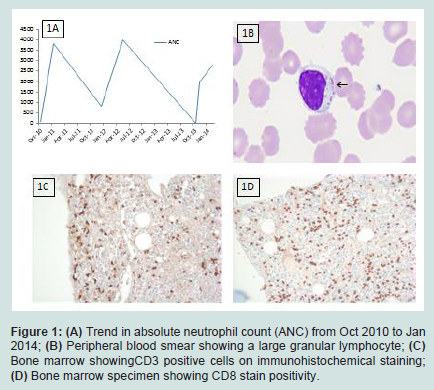
Evaluation of neutropenia was restarted during the current hospital admission. Her current home medications include darbopoetin, calcium acetate, metoprolol, and amlodipine. Peripheral blood smear showed an increase in lymphocytes which were large and granular in appearance (Figure 1B). Serum iron panel, vitamin B12, folic acid level, lactate dehydrogenase and haptoglobin levels were normal. CT scan of chest and abdomen did not reveal any evidence of hepatosplenomegaly or lymphadenopathy. Autoimmune panel revealed weak positivity for rheumatoid factor (RF) and anti-nuclear antibody (ANA), however anti double stranded DNA antibody, antineutrophil cytoplasmic antibody (ANCA), and complement levels were normal. Bone marrow exam showed mild hyper cellularity (70%) for age along with an increase in the interstitial T-lymphocytes. Flow cytometry of the bone marrow showed an aberrant T-cell population. Flow cytometry analysis of these cells were positive for CD3, CD7, CD8, CD16, CD57 and negative for CD4, CD56 (Figures 1C and 1D). Flow cytometry was not performed to look for surface expression of T-cell receptor (TCR) alpha-beta or gamma-delta heterodimers on the aberrant T-cells. Polymerase chain reaction analysis showed evidence of TCR-γ gene rearrangement consistent with a clonal T-cell expansion. The patient was managed with supportive measures in the form of granulocyte colony stimulating factor (G-CSF) and antibiotics with which her infection resolved and ANC normalized (2800 /microL). She was placed on periodic followup as the neutropenia improved and was advised to be abstinent from using cocaine. LGL leukemia-directed immunosuppressive therapy was not recommended as her ANC improved to >500/microL and she did not have recurrent infections.
Discussion
Chronic neutropenia is a hematological condition which could be caused by a variety of benign and malignant diseases. In the given case, there are at least two etiologies which could be attributed to the chronic neutropenia. One is a well-known cause (LGL leukemia) and the other is a rare cause (cocaine abuse). Whether these conditions are merely co-existing or causally related is an interesting point of discussion. Recent reports have suggested that levamisole contaminated cocaine abuse can trigger immune mediated processes like vasculitis and neutropenia which could be possible in our case too [1,2]. Levamisole is known to increase T-cell activation and proliferation. It acts as a hapten to form antibodies to various antigens and also triggers an immune response involving the opsonization and destruction of leukocytes [2]. In the given case, there is certainly a temporal correlation of worsening neutropenia during the periods when the patient was using cocaine. On the other hand, our patient also has a pathologically proven LGL leukemia which manifests with neutropenia. Careful analysis of the chronology of events in our patient suggests that the duration of neutropenia antedates the diagnosis of LGL leukemia by more than 1 year. Although LGL leukemia is a slow growing malignancy and the diagnosis is sometimes difficult to establish, the possibility of missing LGL leukemia during the initial evaluation is less likely in our case as careful review of the prior bone marrow specimens did not reveal any evidence of malignancy. One interesting speculation is that the chronic neutropenia was initially precipitated by cocaine abuse and got worse with the diagnosis of LGL leukemia. It is important to note that chronic antigenic stimulation and immune dysregulation are important mechanisms in the pathogenesis of LGL leukemia [3]. Hence, the other possibility is that cocaine could have acted as a chronic antigenic stimulation in our patient who also had some laboratory features of autoimmunity in the form of positive ANA and rheumatoid factor, and this eventually could have led to the progression to LGL leukemia. Our patient did not have other clinical features of rheumatoid arthritis.Conclusion
Chronic neutropenia requires a meticulous evaluation of its etiology. Slow growing chronic lymphoproliferative malignancies like LGL leukemia can present with neutropenia. With substance abuse being a common problem in the United States, it would be interesting to look for pathological associations between substance abuse and hematological malignancies to delineate if there is a causeeffect relationship.References
- Arora NP (2013) Cutaneous vasculopathy and neutropenia associated with levamisole-adulterated cocaine. Am J Med Sci 345: 45-51.
- Buchanan JA, Lavonas EJ (2012) Agranulocytosis and other consequences due to use of illicit cocaine contaminated with levamisole. Curr Opin Hematol 19: 27-31.
- Lamy T, Loughran TP Jr (2011) How I treat LGL leukemia. Blood 117: 2764-2774.
- Christopoulos PD, Katsoudas S, Androulaki A, Nakopoulou L, Economopoulos T, et al. (2009) T-cell large granular lymphocyte leukemia presenting as end-stage renal disease: the diagnostic role of flow-cytometric and clonality analysis of the urine sediment. Clin Nephrol 71: 198-202.
- Zhang D, Loughran TP Jr (2012) Large granular lymphocytic leukemia: molecular pathogenesis, clinical manifestations, and treatment. Hematology Am Soc Hematol Educ Program 2012: 652-659.