
Review Aricle
*Address for Correspondence: Benedict Yan, Department of Laboratory Medicine, Molecular Diagnosis Centre, National University Hospital, National University Health System, Singapore; E-mail: benedict_yan@nuhs.edu.sgEvelyn Siew-Chuan Koay, Department of Pathology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; E-mail: evelyn_koay@nuhs.edu.sg
Citation: Yan B, Lee PL, Ng C, Ng CH, Chng WJ, et al. Kinase Mutations as Predictive Biomarkers in Hematolymphoid Malignancies. J Hematol Thromb 2015;1(1): 4.
Copyright © 2015 by Yan et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology & Thrombosis | ISSN: 2380-6842 | Volume: 1, Issue: 1
Submission: 10 January 2015 | Accepted: 27 January 2015 | Published: 31 January 2015
Reviewed & Approved by: Dr. Kamal Kant Singh Abbi, Assistant Professor of Hematology, Oncology and Blood & Marrow transplantation, University of Iowa Hospitals and Clinics, USA

 Compound mutations (defined as two or more mutations in the same BCR-ABL molecule [17]) resulting in high-level resistance may arise due to sequential TKI treatment [18,19].
Compound mutations (defined as two or more mutations in the same BCR-ABL molecule [17]) resulting in high-level resistance may arise due to sequential TKI treatment [18,19].
Kinase Mutations as Predictive Biomarkers in Hematolymphoid Malignancies
Benedict Yan1*, Peak-Ling Lee1, Christopher Ng1, Chin Hin Ng2,Wee-Joo Chng2,3,4 and Evelyn Siew-Chuan Koay1,5*
- 1Department of Laboratory Medicine, Molecular Diagnosis Centre, National University Hospital, National University Health System, Singapore
- 2Department of Haematology-Oncology, National University Cancer Institute, Singapore, National University Health System
- 3Cancer Science Institute, Singapore, National University of Singapore
- 4Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore
- 5Department of Pathology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
*Address for Correspondence: Benedict Yan, Department of Laboratory Medicine, Molecular Diagnosis Centre, National University Hospital, National University Health System, Singapore; E-mail: benedict_yan@nuhs.edu.sgEvelyn Siew-Chuan Koay, Department of Pathology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; E-mail: evelyn_koay@nuhs.edu.sg
Citation: Yan B, Lee PL, Ng C, Ng CH, Chng WJ, et al. Kinase Mutations as Predictive Biomarkers in Hematolymphoid Malignancies. J Hematol Thromb 2015;1(1): 4.
Copyright © 2015 by Yan et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology & Thrombosis | ISSN: 2380-6842 | Volume: 1, Issue: 1
Submission: 10 January 2015 | Accepted: 27 January 2015 | Published: 31 January 2015
Reviewed & Approved by: Dr. Kamal Kant Singh Abbi, Assistant Professor of Hematology, Oncology and Blood & Marrow transplantation, University of Iowa Hospitals and Clinics, USA
Introduction
Targeted therapeutics against kinases has been employed in the clinic for over a decade. Their use of ten times requires concomitant molecular diagnostics evaluating the mutational status of the targeted kinases. While kinase mutations function as diagnostic and prognostic biomarkers in hematolymphoid malignancies, in this review, we focus on kinase mutations with predictive utility and their relevance to molecular diagnostics.ABL Mutations in Philadelphia-Positive Leukemias
The development of the tyrosine kinase inhibitor (TKI) imatinib against the BCR-ABL fusion product in chronic myeloid leukemia (CML) was a watershed event that ushered in the era of targeted therapeutics in oncology [1,2].Although CML patients show a high rate of response to imatinib [3] and other approved TKIs (nilotinib [4], dasatinib [5] and bosutinib [6], primary and acquired resistance is observed [7,8]. One of the earliest documented mechanisms of resistance to TKIs is mutations in the ABL kinase domain [9]. ABL kinase domain mutations are now believed to be one of the more frequent causes of TKI resistance [8].
The T315I mutation was the first mutation reported in the context of TKI resistance [9]. To date, more than 90 mutations have been described, although it appears that 15 amino acid substitutions account for more than 85% of the mutations observed clinically [8]. Kinase domain mutations may be classified into two groups – those that alter amino acids directly in contact with the TKI; or those that prevent the oncoprotein from achieving the inactive conformational state required for TKI binding [10]. Several studies have examined the relationship between specific ABL kinase domain mutations and TKI response [11-13]. Table 1 provides a list of mutations that have been studied for their clinical significance. (The reader is referred to other references for the in vitro sensitivity data of the mutations [14]). Our local institutional data for the distribution of ABL kinase domain mutations is displayed in Figure 1.
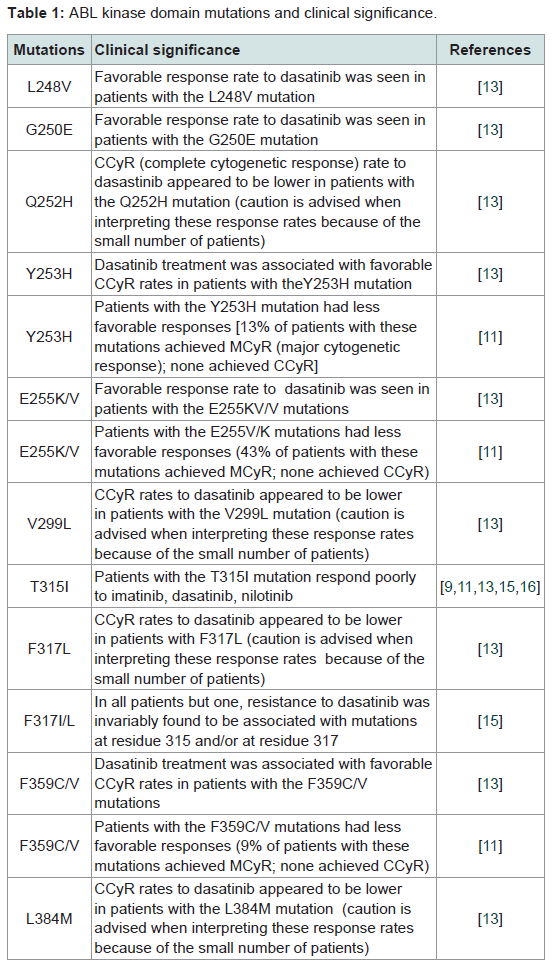
Table 1: ABL kinase domain mutations and clinical significance.
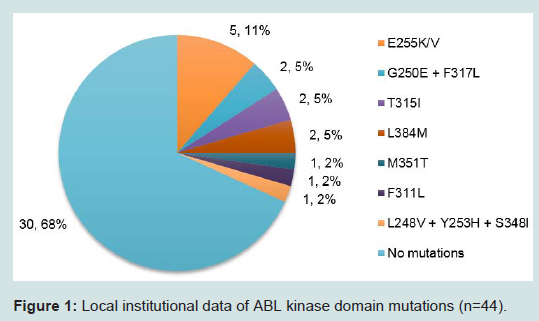
Figure 1: Local institutional data of ABL kinase domain mutations (n=44).
With regards to the implications of ABL kinase domain mutations for the molecular diagnostics laboratory, several issues are noteworthy. The first is that conventional Sanger sequencing has a detection limit of 10-20% and may not enable the detection of low level mutations that might have an impact on therapeutic response and clinical outcome [20]. Several techniques have been employed to detect low-level mutations, including allele-specific oligonucleotide polymerase chain reaction (PCR) [21] and mass spectrometry [20]. More recently, next-generation sequencing (NGS) platforms have been utilized for the detection of low-level mutations [22,23].
Second, the distinction between compound and polyclonal mutations is difficult to address by existing platforms (conventional Sanger sequencing or NGS) due to PCR-mediated recombination generating chimeric amplicons containing sequences from more than one allele [24]. A conceivable solution is single-molecule sequencing, which has not yet entered the clinical molecular diagnostic arena [25].
BRAF Mutations in Hematolymphoid Neoplasms
BRAF, a serine/threonine kinase is an established oncogene and therapeutic target [26]. BRAF mutations were first reported in solid tumors in 2002 [27] and subsequently identified in hematolymphoid neoplasms (reviewed in Machnicki et al. [28]). The most common BRAF mutation across all tumor types is the V600E mutation [26]. Vemurafenib was the first small molecule inhibitor reported to display enhanced activity against the BRAF V600E mutant protein compared to the wild-type protein [26,29]; currently, both vemurafenib and dabrafenib are approved for the treatment of BRAF V600E-mutant melanomas [30,31].To date, the companion diagnostic-therapeutic paradigm for BRAF inhibitors has been reported in hairy cell leukemia [32-39], Langerhans cell histiocytosis (LCH) [40,41] / Erdheim-Chester disease (ECD) [41-43] and multiple myeloma [44,45]. These are discussed in detail below.
The genetic drivers of hairy cell leukemia (HCL) were unknown until 2011, when Tiacci et al. performed whole-exome sequencing of an index case which led to the identification of the BRAF V600E mutation and subsequently showed the mutation to be present in a larger cohort of HCL samples [46]. Approximately a year later, Dietrich et al. reported the first case of a patient with refractory BRAF V600E-mutant HCL who responded to vemurafenib monotherapy; similar reports of response to BRAF inhibitors have since followed [32-39].
Similar to HCL, the genetic events in LCH and ECD (both diseases of histiocytes), remained obscure until the identification of BRAF V600E mutations in LCH (reported in 2010 [47]) and ECD (reported in 2012 [48,49]). Subsequent studies have demonstrated response of BRAF V600E-mutant LCH and ECD patients to vemurafenib [40-43].
The existence of BRAF mutations in multiple myeloma was first reported in 2011 [50]. Around two years later, Andrulis et al. reported clinical response in a multiple myeloma patient with the BRAF V600E mutation treated with the mutation-specific inhibitor vemurafenib [44]. Other authors have reported similar findings [45]. This represents the first example of an effective kinase inhibitor against multiple myeloma.
BTK Mutations in B-Cell Malignancies
Bruton’s tyrosine kinase (BTK) is a non-receptor tyrosine kinase that was first implicated in X-linked agammaglobulinemia [51]. Subsequent work demonstrated that BTK is an important player in many B-cell malignancies [52].Ibrutinib [53], an irreversible BTK inhibitor that binds covalently to the C481 residue of BTK at its active site [54], has been approved for the treatment of relapsed or refractory mantle cell lymphoma (MCL) [55]. Phase 1 and 2 trials have showed that ibrutinib is also efficacious against chronic lymphocytic leukemia (CLL) [56,57].
Similar to what has been observed with ABL resistance mutations developing in response to TKI therapy, a BTK C481S mutation resulting in ibrutinib resistance [58] has been reported in both MCL [59] and CLL [60,61] patients.
Conclusion
The BRAF inhibitors, vemurafenib, dabrafenib and BTK inhibitor, ibrutinib have only recently been employed clinically for the treatment of hematolymphoid neoplasms and experience with these agents is still limited. The decade-long accumulated wisdom with BCR-ABL inhibitors for the treatment of CML suggests that multiple resistance mutations against vemurafenib/dabrafenib and ibrutinib might similarly develop. In melanomas, MEK1 and MEK2 mutations have been identified as a possible resistance mechanism against BRAF inhibitors [62]. The results of further studies into resistance mutations are eagerly anticipated.References
- Druker BJ (2009) Perspectives on the development of imatinib and the future of cancer research. Nat Med 15: 1149-1152.
- Druker BJ, Talpaz M, Resta DJ, Peng B, Buchdunger E, et al. (2001) Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N Engl J Med 344: 1031-1037.
- Druker BJ, Guilhot F, O'Brien SG, Gathmann I, Kantarjian H, et al. (2006) Five-year follow-up of patients receiving imatinib for chronic myeloid leukemia. N Engl J Med 355: 2408-2417.
- Saglio G, Kim DW, Issaragrisil S, le Coutre P, Etienne G, et al. (2010) Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med 362: 2251-2259.
- Kantarjian H, Shah NP, Hochhaus A, Cortes J, Shah S, et al. (2010) Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med 362: 2260-2270.
- Khoury HJ, Cortes JE, Kantarjian HM, Gambacorti-Passerini C, Baccarani M, et al. (2012) Bosutinib is active in chronic phase chronic myeloid leukemia after imatinib and dasatinib and/or nilotinib therapy failure. Blood 119: 3403-3412.
- Apperley JF (2007) Part I: mechanisms of resistance to imatinib in chronic myeloid leukaemia. Lancet Oncol 8: 1018-1029.
- Apperley JF (2014) Chronic myeloid leukaemia. Lancet.
- Gorre ME, Mohammed M, Ellwood K, Hsu N, Paquette R, et al. (2001) Clinical resistance to STI-571 cancer therapy caused by BCR-ABL gene mutation or amplification. Science 293: 876-880.
- Shah NP, Nicoll JM, Nagar B, Gorre ME, Paquette RL, et al. (2002) Multiple BCR-ABL kinase domain mutations confer polyclonal resistance to the tyrosine kinase inhibitor imatinib (STI571) in chronic phase and blast crisis chronic myeloid leukemia. Cancer Cell 2: 117-125.
- Hughes T, Saglio G, Branford S, Soverini S, Kim DW, et al. (2009) Impact of baseline BCR-ABL mutations on response to nilotinib in patients with chronic myeloid leukemia in chronic phase. J Clin Oncol 27: 4204-4210.
- Jabbour E, Branford S, Saglio G, Jones D, Cortes JE, et al. (2011) Practical advice for determining the role of BCR-ABL mutations in guiding tyrosine kinase inhibitor therapy in patients with chronic myeloid leukemia. Cancer 117: 1800-1811.
- Muller MC, Cortes JE, Kim DW, Druker BJ, Erben P, et al. (2009) Dasatinib treatment of chronic-phase chronic myeloid leukemia: analysis of responses according to preexisting BCR-ABL mutations. Blood 114: 4944-4953.
- Soverini S, Hochhaus A, Nicolini FE, Gruber F, Lange T, et al. (2011) BCR-ABL kinase domain mutation analysis in chronic myeloid leukemia patients treated with tyrosine kinase inhibitors: recommendations from an expert panel on behalf of European LeukemiaNet. Blood 118: 1208-1215.
- Soverini S, Colarossi S, Gnani A, Castagnetti F, Rosti G, et al. (2007) Resistance to dasatinib in Philadelphia-positive leukemia patients and the presence or the selection of mutations at residues 315 and 317 in the BCR-ABL kinase domain. Haematologica 92: 401-404.
- Talpaz M, Shah NP, Kantarjian H, Donato N, Nicoll J, et al. (2006) Dasatinib in imatinib-resistant Philadelphia chromosome-positive leukemias. N Engl J Med 354: 2531-2541.
- O'Hare T, Zabriskie MS, Eiring AM, Deininger MW (2012) Pushing the limits of targeted therapy in chronic myeloid leukaemia. Nat Rev Cancer 12: 513-526.
- Khorashad JS, Milojkovic D, Mehta P, Anand M, Ghorashian S, et al. (2008) In vivo kinetics of kinase domain mutations in CML patients treated with dasatinib after failing imatinib. Blood 111: 2378-2381.
- Shah NP, Skaggs BJ, Branford S, Hughes TP, Nicoll JM, et al. (2007) Sequential ABL kinase inhibitor therapy selects for compound drug-resistant BCR-ABL mutations with altered oncogenic potency. J Clin Invest 117: 2562-2569.
- Parker WT, Lawrence RM, Ho M, Irwin DL, Scott HS, et al. (2011) Sensitive detection of BCR-ABL1 mutations in patients with chronic myeloid leukemia after imatinib resistance is predictive of outcome during subsequent therapy. J Clin Oncol 29: 4250-4259.
- Ernst T, Gruber FX, Pelz-Ackermann O, Maier J, Pfirrmann M, et al. (2009) A co-operative evaluation of different methods of detecting BCR-ABL kinase domain mutations in patients with chronic myeloid leukemia on second-line dasatinib or nilotinib therapy after failure of imatinib. Haematologica 94: 1227-1235.
- Kastner R, Zopf A, Preuner S, Proll J, Niklas N, et al. (2014) Rapid identification of compound mutations in patients with Philadelphia-positive leukaemias by long-range next generation sequencing. Eur J Cancer 50: 793-800.
- Soverini S, De Benedittis C, Machova Polakova K, Brouckova A, Horner D, et al. (2013) Unraveling the complexity of tyrosine kinase inhibitor-resistant populations by ultra-deep sequencing of the BCR-ABL kinase domain. Blood 122: 1634-1648.
- Parker WT, Phillis SR, Yeung DT, Hughes TP, Scott HS, et al. (2014) Many BCR-ABL1 compound mutations reported in chronic myeloid leukemia patients may actually be artifacts due to PCR-mediated recombination. Blood 124: 153-155.
- Chaisson MJ, Huddleston J, Dennis MY, Sudmant PH, Malig M, et al. (2014) Resolving the complexity of the human genome using single-molecule sequencing. Nature [Epub ahead of print].
- Holderfield M, Deuker MM, McCormick F, McMahon M (2014) Targeting RAF kinases for cancer therapy: BRAF-mutated melanoma and beyond. Nat Rev Cancer 14: 455-467.
- Davies H, Bignell GR, Cox C, Stephens P, Edkins S, et al. (2002) Mutations of the BRAF gene in human cancer. Nature 417: 949-954.
- Machnicki MM, Stoklosa T (2014) BRAF--a new player in hematological neoplasms. Blood Cells Mol Dis 53: 77-83.
- Tsai J, Lee JT, Wang W, Zhang J, Cho H, et al. (2008) Discovery of a selective inhibitor of oncogenic B-Raf kinase with potent antimelanoma activity. Proc Natl Acad Sci U S A 105: 3041-3046.
- Kim G, McKee AE, Ning YM, Hazarika M, Theoret M, et al. (2014) FDA approval summary: vemurafenib for treatment of unresectable or metastatic melanoma with the BRAFV600E mutation. Clin Cancer Res 20: 4994-5000.
- Menzies AM, Long GV (2014) Dabrafenib and trametinib, alone and in combination for BRAF-mutant metastatic melanoma. Clin Cancer Res 20: 2035-2043.
- Dietrich S, Glimm H, Andrulis M, von Kalle C, Ho AD, et al. (2012) BRAF inhibition in refractory hairy-cell leukemia. N Engl J Med 366: 2038-2040.
- Dietrich S, Hullein J, Hundemer M, Lehners N, Jethwa A, et al. (2013) Continued response off treatment after BRAF inhibition in refractory hairy cell leukemia. J Clin Oncol 31: e300-303.
- Follows GA, Sims H, Bloxham DM, Zenz T, Hopper MA, et al. (2013) Rapid response of biallelic BRAF V600E mutated hairy cell leukaemia to low dose vemurafenib. Br J Haematol 161: 150-153.
- Maurer H, Haas P, Wengenmayer T, Lubbert M, Duyster J, et al. (2014) Successful vemurafenib salvage treatment in a patient with primary refractory hairy cell leukemia and pulmonary aspergillosis. Ann Hematol 93: 1439-1440.
- Munoz J, Schlette E, Kurzrock R (2013) Rapid response to vemurafenib in a heavily pretreated patient with hairy cell leukemia and a BRAF mutation. J Clin Oncol 31: e351-352.
- Peyrade F, Re D, Ginet C, Gastaud L, Allegra M, et al. (2013) Low-dose vemurafenib induces complete remission in a case of hairy-cell leukemia with a V600E mutation. Haematologica 98: e20-e22.
- Samuel J, Macip S, Dyer MJ (2014) Efficacy of vemurafenib in hairy-cell leukemia. N Engl J Med 370: 286-288.
- Vergote V, Dierickx D, Janssens A, Verhoef G, Tousseyn T, et al. (2014) Rapid and complete hematological response of refractory hairy cell leukemia to the BRAF inhibitor dabrafenib. Ann Hematol 93: 2087-2089.
- Charles J, Beani JC, Fiandrino G, Busser B (2014) Major response to vemurafenib in patient with severe cutaneous Langerhans cell histiocytosis harboring BRAF V600E mutation. J Am Acad Dermatol 71: e97-99.
- Haroche J, Cohen-Aubart F, Emile JF, Arnaud L, Maksud P, et al. (2013) Dramatic efficacy of vemurafenib in both multisystemic and refractory Erdheim-Chester disease and Langerhans cell histiocytosis harboring the BRAF V600E mutation. Blood 121: 1495-1500.
- Haroche J, Cohen-Aubart F, Emile JF, Maksud P, Drier A, et al. (2014) Reproducible and Sustained Efficacy of Targeted Therapy With Vemurafenib in Patients With BRAFV600E-Mutated Erdheim-Chester Disease. J Clin Oncol [Epub ahead of print].
- Mazor RD, Manevich-Mazor M, Kesler A, Aizenstein O, Eshed I, et al. (2014) Clinical considerations and key issues in the management of patients with Erdheim-Chester Disease: a seven case series. BMC Med 12: 221.
- Andrulis M, Lehners N, Capper D, Penzel R, Heining C, et al. (2013) Targeting the BRAF V600E mutation in multiple myeloma. Cancer Discov 3: 862-869.
- Sharman JP, Chmielecki J, Morosini D, Palmer GA, Ross JS, et al. (2014) Vemurafenib response in 2 patients with posttransplant refractory BRAF V600E-mutated multiple myeloma. Clin Lymphoma Myeloma Leuk 14: e161-163.
- Tiacci E, Trifonov V, Schiavoni G, Holmes A, Kern W, et al. (2011) BRAF mutations in hairy-cell leukemia. N Engl J Med 364: 2305-2315.
- Badalian-Very G, Vergilio JA, Degar BA, MacConaill LE, Brandner B, et al. (2010) Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood 116: 1919-1923.
- Haroche J, Charlotte F, Arnaud L, von Deimling A, Helias-Rodzewicz Z, et al. (2012) High prevalence of BRAF V600E mutations in Erdheim-Chester disease but not in other non-Langerhans cell histiocytoses. Blood 120: 2700-2703.
- Blombery P, Wong SQ, Lade S, Prince HM (2012) Erdheim-Chester disease harboring the BRAF V600E mutation. J Clin Oncol 30: e331-332.
- Chapman MA, Lawrence MS, Keats JJ, Cibulskis K, Sougnez C, et al. (2011) Initial genome sequencing and analysis of multiple myeloma. Nature 471: 467-472.
- Vetrie D, Vorechovsky I, Sideras P, Holland J, Davies A, et al. (1993) The gene involved in X-linked agammaglobulinaemia is a member of the src family of protein-tyrosine kinases. Nature 361: 226-233.
- Hendriks RW, Yuvaraj S, Kil LP (2014) Targeting Bruton's tyrosine kinase in B cell malignancies. Nat Rev Cancer 14: 219-232.
- Cameron F, Sanford M (2014) Ibrutinib: first global approval. Drugs 74: 263-271.
- Honigberg LA, Smith AM, Sirisawad M, Verner E, Loury D, et al. (2010) The Bruton tyrosine kinase inhibitor PCI-32765 blocks B-cell activation and is efficacious in models of autoimmune disease and B-cell malignancy. Proc Natl Acad Sci U S A 107: 13075-13080.
- Herrera AF, Jacobsen ED (2014) Ibrutinib for the treatment of mantle cell lymphoma. Clin Cancer Res 20: 5365-5371.
- Advani RH, Buggy JJ, Sharman JP, Smith SM, Boyd TE, et al. (2013) Bruton tyrosine kinase inhibitor ibrutinib (PCI-32765) has significant activity in patients with relapsed/refractory B-cell malignancies. J Clin Oncol 31: 88-94.
- Byrd JC, Furman RR, Coutre SE, Flinn IW, Burger JA, et al. (2013) Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med 369: 32-42.
- Cheng S, Guo A, Lu P, Ma J, Coleman M, et al. (2014) Functional characterization of BTK mutation that confers ibrutinib resistance: exploration of alternative kinase inhibitors. Leukemia.
- Chiron D, Di Liberto M, Martin P, Huang X, Sharman J, et al. (2014) Cell-cycle reprogramming for PI3K inhibition overrides a relapse-specific C481S BTK mutation revealed by longitudinal functional genomics in mantle cell lymphoma. Cancer Discov 4: 1022-1035.
- Furman RR, Cheng S, Lu P, Setty M, Perez AR, et al. (2014) Ibrutinib resistance in chronic lymphocytic leukemia. N Engl J Med 370: 2352-2354.
- Woyach JA, Furman RR, Liu TM, Ozer HG, Zapatka M, et al. (2014) Resistance mechanisms for the Bruton's tyrosine kinase inhibitor ibrutinib. N Engl J Med 370: 2286-2294.
- Rizos H, Menzies AM, Pupo GM, Carlino MS, Fung C, et al. (2014) BRAF inhibitor resistance mechanisms in metastatic melanoma: spectrum and clinical impact. Clin Cancer Res 20: 1965-1977.