
Research article
Evaluation of Prostate CancerDetection Rates in PatientsUndergoing TransrectalUltrasound (TRUS) GuidedProstate Biopsy
Erkan Erdem1*, Murat Bozlu2
- 1Department of Urology, Ota Jinemed Hospital, Turkey
- 2Mersin University, Medical Faculty, Department of Urology
*Address for correspondence: Erkan Erdem, Department of Urology, Ota Jinemed Hospital, İstanbul, Turkey, E-mail: erkanerdemmd@gmail.com
Citation: Erdem E. Evaluation of Prostate Cancer Detection Rates in Patients Undergoing Transrectal Ultrasound (TRUS) Guided Prostate Biopsy. J Cancer Sci. 2018;5(1): 4.
Journal of Cancer Sciences | ISSN: 2377-9292 | Volume: 5, Issue: 1
Submission: 22 November, 2018| Accepted: 26 December, 2018 | Published: 28 December, 2018
Copyright: © 2018 Erdem E. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Prostate cancer is one of the most common types of organ cancer among males in Turkey as well as all over the world. The gold standard method for histopathological diagnosis of prostate cancer is Trans rectal Ultrasound (TRUS)-guided prostate biopsy. Today, the most common indications for prostate biopsy are suspicious findings on digital rectal examination and increased serum Prostate Specific Antigen (PSA) level. Although there is no generally accepted guideline regarding the preparation and performing prostate biopsies, it has been reported that prostate cancer is detected at different frequencies with different techniques. In this study, we aimed to investigate the frequency of prostate cancer detected in patients undergoing TRUS-guided prostate biopsy and its relationship with patient characteristics and technique.
Material and methods: Patients, who had undergone TRUSguided prostate biopsy between January 2003 and December 2007 at the Urology Department of Mersin University Faculty of Medicine, were enrolled in the study. All patients were standardly prepared before the biopsy and at least 12 pieces of biopsy specimens were obtained during the procedure.
Results: A total of 906 biopsies were performed in 832 patients. The mean age of the patients was 67.2±8.7 years. Sixty-two patients (6.8%) had undergone biopsy two-times and 12 patients (1.3%) had undergone the procedure 3-times. Prostate cancer detection rates were 29.4% in first biopsies and 12.9% in second biopsies. No cancer was detected in any of the patients who had undergone the third prostate biopsy. When evaluated according to years, the prostate cancer detection rates were found to be 16.5%, 30.2%, 25.1%, 31% and 30.1% from 2003 to 2007, respectively. Prostate cancer rates were 19% and 8.6% in patients with normal (n = 573) and suspicious (n = 259) digital rectal examination findings. When the rates of prostate cancer according to PSA values were evaluated, the prostate cancer rates in patients with serum PSA <4 ng / ml, 4-10 ng / ml and > 10 ng / ml were found to be 4.8%, 17.9% and 47%, respectively.
Conclusion: Prostate cancer, the rate of which has increased in recent years, responds very well to treatment when diagnosed early. Our findings, in particular, the frequent use of PSA and advances in biopsy techniques have been shown to be important factors in the increase in prostate cancer detection rates. Our findings show that a number of factors, especially more frequent measurement of PSA and improvements in biopsy techniques play important roles in the increase in prostate cancer detection rates.
Keywords
TRUS-guided prostate biopsy; Prostate cancer; Prostatespecific antigen; Gleason score
Introduction
Prostate cancer is one of the most common organ cancers in men today. It is the second cause of death following lung cancer. According to autopsy studies, the risk of prostate cancer in a 50-year-old male is 30-50%, whereas this rate increases up to 80% by the age of 80 years [1]. According to a study in US, clinically significant prostate cancer is detected in one in 10 men aged 50 and over. A mortality prevalence of up to 30% per year has been reported for this disease, which increases with age. As a result of its age-related incidence, prostate cancer is the most common cause of death in the USA among the male population over 75 years of age [2].
The most common and ancient method in the diagnosis of prostate cancer is Digital Rectal Examination (DRE). However, since it is difficult to diagnose prostate cancer with DRE, the disease can only be detected in advanced stages. A delay in the diagnosis results in difficulty in treatment and even makes it impossible to cure. In addition to DRE, tumor markers (PSA) and imaging modalities (Transrectal Ultrasound) are used to obviate the delay in diagnosis [3]. TRUS was first applied by Wild and Reid in 1957, and was placed into clinical practice by Watanabe et al. in 1967 [4,5]. It is the first-line diagnostic radiological modality in prostate diseases. In addition to the fact that TRUS is easy to use and cheap, it also provides guidance to biopsy in cases with suspicious clinical and laboratory findings of prostate cancer and its use in staging and follow-up of cases diagnosed with cancer also plays an important role.
In comparative studies using different combinations of thesemethods, none of these methods was found to be sufficient to diagnose prostate cancer alone. However, the results showed that the cancer detection rate of each method increased in cases with cancer suspicion and the sensitivity of the methods increased. Moreover, the use of free PSA (fPSA) and PSA Density (PSAD) has been introduced in order to eliminate the false positive results caused by elevated serum PSA levels due to benign causes and to increase the sensitivity.
In the light of this information, the aim of our study was todetermine prostate cancer detection rates in TRUS-guided prostate biopsies performed for appropriate indications. Curative treatment of prostate cancer is possible when diagnosed early. We think that a reduction in the number of unnecessary prostate biopsies is the most effective way of preventing biopsy-related complications.
Materials and Methods
The study included male patients who had presented to the Urology Outpatient Clinic of Mersin University Faculty of Medicine, Urology Outpatient Clinic, with lower urinary tract and / or other urological complaints and undergone TRUS-guided prostate biopsy between January 2003 and December 2007 due to high serum PSA or abnormal rectal digital examination findings. All patients had undergone digital rectal examination and serum PSA had been measured on admission. The TRUS-guided prostate volumes were calculated. Serum PSA values were evaluated based on the reference PSA intervals of the patient′s age group. All patients had been informed about the procedure and 12-core biopsy protocol had been carried out. Ciprofloxacin 500 mg was administered intravenously to all patients at night prior to the biopsy and on the morning of the biopsy and repeated every 12 hours for 3 days. A rectal enema was applied to all patients before biopsy. Prostate biopsies were performed using an 18 Gauge × 20 cm biopsy needle and automatic biopsy gun (Angiotech Tru-Core I, U.S.A) guided by a 7.5 MHz rectal probe (Siemens Sonoline Adara, Germany) with the patient lying on left lateral decubitus position. All core biopsy specimens were sent to the pathology laboratory in separate tubes.
Statistical analysis
The Chi-Square test, the Mann-Whitney U test, the Shapiro-Wilktest and the Independent samples T test were used for the statistical analyses of the data. For the statistical analysis, the SPSS (Statistical Package for the Social Sciences) Standard Version Package for Windows Release 11.5.1 was used. The Microsoft Office Standard Edition for students and Teachers, Microsoft ® Office Excel 2003 module was used as a second tool.
Ethical Issues
This study was approved by the Mersin University Medical Faculty Ethics Committee (dated 24.01.2008, numbered 2008/04).
Results
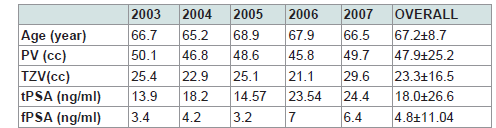
A total of 832 patients undergoing TRUS-guided prostate biopsywere included in the study. The mean age of the patients was 67.2±8.7 years. The distribution of age, prostate volumes and serum PSA levels according to years have been displayed in (Table 1). 62 (6.8%) of the patients had undergone a second biopsy and 12 (1.32%) patients had undergone a third biopsy, and a total of 906 prostate biopsy procedures had been performed during the study period.
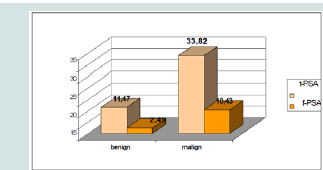
The mean serum PSA level of the patients diagnosed with prostatecancer was 33.82 ng / ml. While prostate cancer was detected in 17.9% of patients with PSA values in the gray zone (4-10 ng / ml), the rates of cancer detected in patients with different PSA values have been demonstrated in (Figure 1).
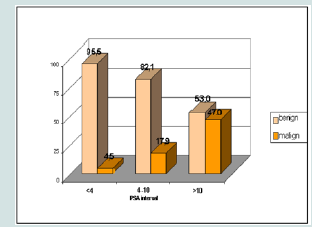
While the cancer rate was 4.5% in the group with a PSA of less than 4 ng / ml, a 17.9% rate of prostate cancer was detected in patients with a serum PSA level of 4-10 ng / ml, which is considered as the ‘gray zone’. In the group with a PSA value of higher than 10 ng / ml, the prostate cancer rate was dteremined to be 47% (Figure 2).
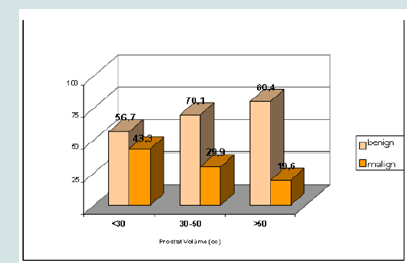
When the prostate volumes were examined, the prostate cancer rates of <30 cc, 30-50 cc and >50 cc prostates were 43.3%, 29.9% and 19.6%, respectively (Figure 3).
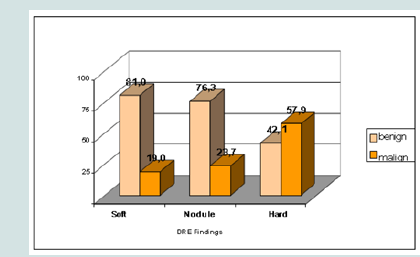
When the DRE findings were examined, 574 (68.8%) of the caseshad soft (no nodules and no hard), 218 (26.2%) had hard and 41 (4.9%) had nodules. The prostate cancer rates in patients with normal and suspected DRE findings were 19% and 81.6%, respectively (Figure 4).
Discussion
TRUS-guided prostate biopsy is an important diagnostic tool in prostate cancer. It requires many stages such as patient preparation, technique, delivery of materials to pathology, reporting by pathologists, and interpretation of the report by the urologist. Although there are differences in patient preparation and technique, the most commonly used method is TRUS-guided prostate needle biopsies. As a result of pathological evaluation of biopsy specimens, prostate cancer is detected in 20-67% of cases and lesions other than cancer can be reported in the remaining [5,6]. Recent studies have shown that approximately 20-30% of pathologically negative patients in the 6-core old biopsy technique have been diagnosed as prostate cancer in recurrent biopsies [7,8].Different nomograms can also be used to increase cancer detection rates in patients undergoing prostate biopsy. In particular, in patients with a serum PSA level between 2 and 10 ng / ml, it can be determined how many cores should be obtained from the patient using the Vienna nomogram [8,9]. In this nomogram, biopsy specimens from 6-to-18 cores are obtained according to patient’s age and prostate volume. As the numbers of biopsies and cores increase, the cancer detection rates increase. In our study, the rate of cancer in the first biopsies was 29.4%, and this rate was 12.9% in the second biopsies. None of our patients who had undergone prostate biopsy for the third time was diagnosed with prostate cancer. Having a negative result in the first biopsy does not exclude prostate cancer, because a significant number of patients whose pathological examination of the first biopsy specimens were reported as ‘lesions other than cancer’, may be diagnosed with prostate cancer in repeat biopsies performed for various reasons. The rates of cancer reported in the first, second, third and fourth biopsies were 22%, 10%, 5% and 4%, respectively [10-12]. We did not detect any cancer in those undergoing biopsy for the third time, because we performed 12-core biopsies instead of 6, 8 or 10-core at the first biopsy procedure. According to our findings, if the 12-core specimens were obtained in the first biopsy procedure and the second biopsy was reported as negative, then the third biopsy would be unnecessary.
One of the main examination methods in a patient suspected of prostate diseases is DRE. Prostate biopsy is recommended in patients who have suspicious findings on DRE. In our study, the rate of prostate cancer was found to be 81.6% in patients with suspected DRE findings. The American Cancer Society has reported the sensitivity of DRE as 57.9%. Biopsies based on rectal examination findings with fingers only have detected cancer at a rate of 6% to 21%. According to the findings of the European Randomized Study of Screening for Prostate Cancer, the positive predictive values of DRE are 2% and 6.3% in individuals with a serum PSA level of <1 ng / ml and 3-3.9 ng / ml, respectively. These results suggest that the use of DRE as a diagnostic method alone is limited, and since it is a subjective examination, its sensitivity is low due to false negativity and its positive predictive value low.
One of the most important laboratory tests used in prostate cancer screening is the measurement of the serum PSA level. With the recent introduction of PSA into daily practice, the incidence of prostate cancer and the rate of diagnosis, especially at the localized disease stage, have increased. The yearly serum PSA measurement for screening is recommended after the age of 50 years for those with a life expectancy of more than 10 years. The mean serum PSA value was found to be 33.82 ng / ml in our patients diagnosed with prostate cancer. While the frequency of prostate cancer is 21-25% in patients with normal DRE findings and a serum PSA level of 4-to-10 ng / ml, this rate increases up to 42% in patients with serum PSA of > 10 ng / ml. In our study, the prostate cancer rate in patients with serum PSAlevels of 4-10 ng / ml, called the gray zone, is approximately 18%. Prostate cancer was detected in 47% of our patients with a serum PSA level of > 10 ng / ml. There is no accepted common value for the lower limit of serum PSA level. In recent years, the PSA threshold has been reduced and prostate cancer has been reported in 22-27% of those having a serum PSA level in the 2.5-to-4 ng / ml range. We detected prostate cancer in 4.5% of our cases with serum PSA of <4 ng / ml. In young patients, due to high mortality and morbidity, it is recommended that the threshold value of serum PSA should be considered to be lower; whereas in elderly patients it is recommended that the threshold value should be considered higher. By decreasing the serum PSA threshold values, it is thought that the number of unnecessary biopsies has increased and most of the cancers diagnosed are clinically insignificant prostate cancer.
TRUS used in prostate biopsies is an important imaging modality. The most important feature of TRUS is that it can detect cancer foci that cannot be identified with DRE. Prostate cancer was detected in 5% of patients with normal DRE findings and PSA values, but with suspected TRUS findings [13]. The American Cancer Society reported the sensitivity of TRUS in the diagnosis of prostate cancer as 77.7%. In our study, the rate of detection of cancer by biopsy was 43.3% in patients with a prostate volume of <30 cc measured on TRUS; this rate was 29.9% in those with a prostate volume between 30-50 cc and 19.6% for those having an > 50 cc prostate volume. Our results suggest that cancer is more frequently encountered in cases with lower prostate volumes and higher PSA levels.
Conclusion
Prostate cancer is a disease that responds very well to treatment when diagnosed at early stages. When examining for clinical prostate cancer, the patient must be evaluated with DRE and serum PSA should be measured before TRUS is performed.
References
- Whingo PA, Tong T, Bolden S (1995) Cancer statistics 1995. CA CancerJ Clin 45: 8-30.
- Murph GP, Natarajan N, Pantes JE, Schmitz RL, Smart CR, et al. (1982) The national surve of prostate cancer in the United States by American College of Surgeons. J Urol 127: 928-934.
- Cooner WH, Mosley BR, Rutherford CL, Beard JH, Pond HS, et al. (1990) Prostate cancer detection in a clinical urological practice by ultrasonography, digital rectal examination and prostate specific antigen. J Urol 143: 1146.
- Hammerer PG, McNeal JE, Stamey TA (1995) Correlation between serum prostate specific antigen levels and the volume of the individual glandular zones of the human prostate. J Urol 153: 111-114.
- Papsidero LD, Wang MC, Valenzuela LA, Murphy GP, Chu TM (1980) A prostate antigen in sera of prostatic cancer patients. Cancer Res 40: 2428-2432.
- Partin AW, Oesterling JE (1994) The clinical usefulness of prostate specific antigen: update 1994. J Urol 152: 1358-1368.
- Catalona WJ, Smith DS, Ornstein DK (1997) Prostate cancer detection in men with serum PSA concentrations of 2.6 to 4.0 ng/mL and benign prostate examination. Enhancement of specificity with free PSA measurements. JAMA 277: 1452-1455.
- Coley CM, Barry MJ, Fleming C, Wasson JH, Fahs MC, et al. (1995) Should Medicare provide reimbursement for prostate-specific antigen testing for early detection of prostate cancer? Part II: early detection strategies. Urology 46: 125-141.
- Catalona WJ, Smith DS, Ratliff TL, Dodds KM, Coplen DE, et al. (1991) Measurement of prostate specific antigen in serum as a screening test for prostate cancer. N Engl J Med 324: 1156-1161.
- Catalona WJ, Partin AW, Slawin, et al. (1997) A multicenter clinical trial evaluation of free PSA in the differentiation of prostate cancer from benign disease. J Urol 157: 111.
- Hankey BF, Feuer EJ, Clegg LX, Hayes RB, Legler JM, et al. (1999) Cancer Surveillance Series: İnterpreting trends in prostate cancer- Part-I: Evidence of the effects of screening in recent prostate cancer incidance mortality, and survival rates. J Natl Cancer Inst 91: 1017-1024.
- Keetch DW, Catalona WJ, Smith DS (1994) Serial prostatic biopsies in men with persistently elevated serum prostate specific antigen values. J. Urol 151: 1571-1574.
- Uzzo RG, Wei JT, Waldbaum RS, Perlmutter AP, Byrne JC, et al. (1995) The influence of prostate size on cancer detection. Urology 46: 831-836.