
Journal of Clinical & Medical Case Reports
Download PDF
Due to suboptimal glycemic control, the metformin XR dose was increased to 750 mg daily. Within two to three weeks following dose escalation, the patient experienced a significant worsening of gastrointestinal symptoms, including:
• Increased stool frequency (four to five times per day)
• Marked abdominal discomfort
• Postprandial urgency
• Exacerbation of symptoms after consumption of spicy food, coffee, and red meat
The patient had no history of hypertension or dyslipidemia. He was a non-smoker and reported occasional alcohol consumption.
• Fasting blood glucose: 140 mg/dL
• HbA1c: 6.5%
• Complete blood count: within normal limits
• Liver function tests: normal
• Thyroid function tests: normal
The HbA1c and FBG results were verified using the formula: Estimated Average Glucose (eAG) = (28.7 × HbA1c) − 46.7, as described by M. Nathan et al. Investigations including H. pylori testing, stool culture, stool routine examination, and barium X-ray were performed and showed no evidence of infection, inflammatory disease, or metabolic abnormalities. Colonoscopy was not indicated, as there was no rectal bleeding and no abnormalities were observed on the X-ray.
The temporal association between the escalation of the metformin dose and the worsening of gastrointestinal symptoms, together with the absence of alarm features, strongly suggested metformin-induced IBS-like gastrointestinal intolerance.
1. Discontinuation of metformin
2. Initiation of dapagliflozin 10 mg once daily
3. Dietary modification, including avoidance of known symptom-triggering foods
Following these interventions, the patient reported marked improvement in gastrointestinal symptoms. Stool frequency returned to normal, and abdominal discomfort resolved.
Glycemic control remained satisfactory with:
• Stable HbA1c of 6.5%
• Acceptable fasting glucose levels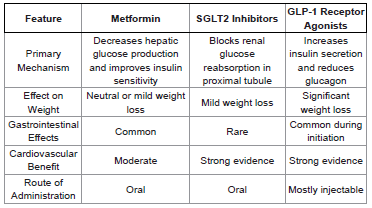 Table 1:Comparative Overview of Antidiabetic Drug Classes
Table 1:Comparative Overview of Antidiabetic Drug Classes
Additional benefits include:
• Modest weight loss
• Reduction in systolic blood pressure
• Cardiovascular and renal protection
The DECLARE-TIMI 58 trial demonstrated that dapagliflozin significantly reduced hospitalization for heart failure and slowed the progression of chronic kidney disease.
GLP-1 Receptor Agonists
Another therapeutic option for patient’s intolerant to metformin is the class of GLP-1 receptor agonists, including liraglutide and semaglutide.
Careful assessment of the temporal relationship between medication exposure and symptom onset is essential in identifying medication-related adverse effects.
Management strategies may include:
• Gradual dose titration
• Use of extended-release formulations
• Dietary modification
• Dose reduction or discontinuation
• Switching to alternative drug classes such as SGLT2 inhibitors or GLP-1 receptor agonists
Learning Points
1. Metformin remains the first-line therapy for type 2 diabetes but frequently causes gastrointestinal adverse effects.
2. In some patients, metformin intolerance may present with IBS-like symptoms such as abdominal pain, bloating, and diarrhea. 3. Symptoms may worsen after dose escalation of metformin.
4. Dietary triggers such as spicy foods, caffeine, and high-fat meals may exacerbate metformin-induced gastrointestinal symptoms.
5. Alternative therapies such as SGLT2 inhibitors can provide effective glycemic control in patients who cannot tolerate metformin.
Case Report
Metformin-Induced Irritable Bowel Syndrome–Like Symptom
Sibi Das*
Department of Medicine NC Medical College, Israna, Panipat, Haryana, India
Address for Correspondence:Dr. Sibi Das, Department of Medicine NC Medical College, Israna,
Panipat, Haryana, India. E-mail Id: sdsilvanose@gmail.com
Submission: 03 February, 2026
Accepted:13 March, 2026
Published:16 March, 2026
Copyright: © 2026 Das S, et al. This is an open access article
distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in
any medium, provided the original work is properly cited.
Keywords:Metformin intolerance; irritable bowel syndrome; Type 2
diabetes mellitus; Dapagliflozin; SGLT2 inhibitors
Abstract
Metformin is the first-line pharmacological therapy for type 2
diabetes mellitus (T2DM). Although gastrointestinal (GI) adverse
effects are common, persistent symptoms resembling irritable bowel
syndrome (IBS) are less frequently reported. We present the case of
a 56-year-old male with T2DM who developed metformin-induced
IBS-like symptoms (IBS -D) characterized by abdominal cramping,
bloating, and postprandial diarrhoea triggered by specific dietary
factors. Symptoms significantly worsened following metformin dose
escalation from 500 mg to 750 mg daily. Laboratory evaluation
revealed adequate glycemic control with fasting blood glucose of
140 mg/dL and HbA1c of 6.5%. After discontinuation of metformin and
initiation of dapagliflozin 10 mg daily along with dietary modification,
gastrointestinal symptoms markedly improved while glycemic control
remained stable. This case highlights the importance of recognizing
metformin-induced IBS-like symptoms and considering alternative
antidiabetic therapies when intolerance occurs.
Introduction
Metformin remains the cornerstone of therapy for type 2 diabetes
mellitus (T2DM) because of its well-established efficacy, favourable
safety profile, and low cost. Current clinical guidelines recommend
metformin as the first-line pharmacotherapy for most patients
with T2DM. Despite its overall favourable profile, gastrointestinal
intolerance represents the most frequently reported adverse effect
associated with metformin therapy. Approximately 20–30% of
patients receiving metformin experience gastrointestinal symptoms,
including diarrhea, abdominal discomfort, nausea, and bloating.
In most cases, these adverse effects are mild and transient. However, in some individuals, persistent gastrointestinal disturbances may develop that closely resemble symptoms of irritable bowel syndrome (IBS). Such symptoms can significantly affect quality of life and lead to poor medication adherence or discontinuation. Recognition of medication-induced gastrointestinal symptoms is therefore essential in the management of diabetic patients presenting with chronic bowel complaints. This report describes a case of dose-dependent metformin intolerance presenting with IBS-like symptoms, which improved after discontinuation of metformin and initiation of dapagliflozin.
In most cases, these adverse effects are mild and transient. However, in some individuals, persistent gastrointestinal disturbances may develop that closely resemble symptoms of irritable bowel syndrome (IBS). Such symptoms can significantly affect quality of life and lead to poor medication adherence or discontinuation. Recognition of medication-induced gastrointestinal symptoms is therefore essential in the management of diabetic patients presenting with chronic bowel complaints. This report describes a case of dose-dependent metformin intolerance presenting with IBS-like symptoms, which improved after discontinuation of metformin and initiation of dapagliflozin.
Case Presentation
A 56-year-old male with a three-year history of type 2 diabetes
mellitus presented with chronic gastrointestinal complaints
consisting of intermittent abdominal cramping, bloating, and
loose stools occurring two to three times daily, associated with
postprandial urgency. The symptoms were particularly triggered by
the consumption of spicy foods, coffee, and red meat.
The patient had no prior history of gastrointestinal disease, inflammatory bowel disease, or food allergies. He denied weight loss, hematochezia, nocturnal diarrhea, fever, or other systemic symptoms.
The patient had no prior history of gastrointestinal disease, inflammatory bowel disease, or food allergies. He denied weight loss, hematochezia, nocturnal diarrhea, fever, or other systemic symptoms.
Medical History:
The patient had been diagnosed with type 2 diabetes mellitus
three years earlier and was initially treated with extended-release
metformin (metformin XR) 500 mg once daily. During this period,
he reported mild intermittent loose stools, which were tolerable and
did not interfere with daily activities.Due to suboptimal glycemic control, the metformin XR dose was increased to 750 mg daily. Within two to three weeks following dose escalation, the patient experienced a significant worsening of gastrointestinal symptoms, including:
• Increased stool frequency (four to five times per day)
• Marked abdominal discomfort
• Postprandial urgency
• Exacerbation of symptoms after consumption of spicy food, coffee, and red meat
The patient had no history of hypertension or dyslipidemia. He was a non-smoker and reported occasional alcohol consumption.
Laboratory Investigations:
Laboratory evaluation revealed the following findings:• Fasting blood glucose: 140 mg/dL
• HbA1c: 6.5%
• Complete blood count: within normal limits
• Liver function tests: normal
• Thyroid function tests: normal
The HbA1c and FBG results were verified using the formula: Estimated Average Glucose (eAG) = (28.7 × HbA1c) − 46.7, as described by M. Nathan et al. Investigations including H. pylori testing, stool culture, stool routine examination, and barium X-ray were performed and showed no evidence of infection, inflammatory disease, or metabolic abnormalities. Colonoscopy was not indicated, as there was no rectal bleeding and no abnormalities were observed on the X-ray.
The temporal association between the escalation of the metformin dose and the worsening of gastrointestinal symptoms, together with the absence of alarm features, strongly suggested metformin-induced IBS-like gastrointestinal intolerance.
Management:
Considering the suspected drug intolerance, the following
management strategy was implemented:1. Discontinuation of metformin
2. Initiation of dapagliflozin 10 mg once daily
3. Dietary modification, including avoidance of known symptom-triggering foods
Following these interventions, the patient reported marked improvement in gastrointestinal symptoms. Stool frequency returned to normal, and abdominal discomfort resolved.
Glycemic control remained satisfactory with:
• Stable HbA1c of 6.5%
• Acceptable fasting glucose levels
Discussion
Metformin is widely recommended as the first-line therapy for
T2DM because of its efficacy, low risk of hypoglycemia, and beneficial
metabolic effects. However, gastrointestinal intolerance remains the
most common adverse effect and may limit long-term adherence in
some patients.
Mechanisms of Metformin-Induced Gastrointestinal Symptoms Several mechanisms have been proposed to explain metformin associated gastrointestinal intolerance.
1. Alteration of Gut Microbiota
Metformin significantly alters intestinal microbiota composition. Studies have demonstrated an increased abundance of bacterial species such as Akkermansia muciniphila and Escherichia species. Although these microbial changes may improve glucose metabolism, they may also increase intestinal fermentation and gas production, contributing to bloating and abdominal discomfort.
2. Increased Intestinal Glucose Metabolism
Metformin enhances intestinal glucose uptake and anaerobic metabolism, resulting in increased lactate production within enterocytes. This process may contribute to intestinal irritation and diarrhea.
3. Bile Acid Malabsorption
Metformin may interfere with bile acid reabsorption in the ileum. Increased bile acid concentrations in the colon stimulate intestinal secretion and motility, resulting in diarrhea resembling IBS.
Mechanisms of Metformin-Induced Gastrointestinal Symptoms Several mechanisms have been proposed to explain metformin associated gastrointestinal intolerance.
1. Alteration of Gut Microbiota
Metformin significantly alters intestinal microbiota composition. Studies have demonstrated an increased abundance of bacterial species such as Akkermansia muciniphila and Escherichia species. Although these microbial changes may improve glucose metabolism, they may also increase intestinal fermentation and gas production, contributing to bloating and abdominal discomfort.
2. Increased Intestinal Glucose Metabolism
Metformin enhances intestinal glucose uptake and anaerobic metabolism, resulting in increased lactate production within enterocytes. This process may contribute to intestinal irritation and diarrhea.
3. Bile Acid Malabsorption
Metformin may interfere with bile acid reabsorption in the ileum. Increased bile acid concentrations in the colon stimulate intestinal secretion and motility, resulting in diarrhea resembling IBS.
4. Serotonin Signalling in the Gut:
Metformin may increase serotonin release from enterochromaffin
cells, which plays a critical role in regulating intestinal motility
and visceral sensitivity. Enhanced serotonin activity may therefore
contribute to IBS-like symptoms.5. Effects on GLP-1 Secretion:
Metformin increases endogenous glucagon-like peptide-1 (GLP-
1) secretion. Although this contributes to improved glycemic control,
it may also influence gastrointestinal motility and appetite regulation.Role of Dietary Triggers:
Dietary factors may exacerbate gastrointestinal symptoms in
patients with metformin intolerance. Spicy foods can stimulate
intestinal motility, while coffee increases colonic activity through
caffeine-mediated hormonal effects. High-fat foods such as red meat
may delay gastric emptying and worsen bloating and abdominal
discomfort. In the present case, these dietary triggers significantly
intensified the patient’s symptoms.Alternative Antidiabetic Therapy
SGLT2 Inhibitors:
After discontinuation of metformin, the patient was treated
with dapagliflozin, a sodium-glucose co-transporter-2 (SGLT2)
inhibitor. SGLT2 inhibitors lower blood glucose by inhibiting renal
glucose reabsorption in the proximal renal tubule, thereby promoting
urinary glucose excretion. Because their mechanism of action is
independent of gastrointestinal absorption, they are less likely to
cause gastrointestinal adverse effects.Additional benefits include:
• Modest weight loss
• Reduction in systolic blood pressure
• Cardiovascular and renal protection
The DECLARE-TIMI 58 trial demonstrated that dapagliflozin significantly reduced hospitalization for heart failure and slowed the progression of chronic kidney disease.
GLP-1 Receptor Agonists
Another therapeutic option for patient’s intolerant to metformin is the class of GLP-1 receptor agonists, including liraglutide and semaglutide.
These agents improve glycemic control by:
• Enhancing glucose-dependent insulin secretion
• Suppressing glucagon release
• Delaying gastric emptying
• Increasing satiety and promoting weight loss
However, GLP-1 receptor agonists frequently cause gastrointestinal adverse effects, particularly nausea and vomiting during treatment initiation. Therefore, they may not be ideal for patients with significant baseline gastrointestinal intolerance.
• Enhancing glucose-dependent insulin secretion
• Suppressing glucagon release
• Delaying gastric emptying
• Increasing satiety and promoting weight loss
However, GLP-1 receptor agonists frequently cause gastrointestinal adverse effects, particularly nausea and vomiting during treatment initiation. Therefore, they may not be ideal for patients with significant baseline gastrointestinal intolerance.
Clinical Implications:
This case emphasizes the importance of recognizing druginduced
gastrointestinal symptoms in patients with diabetes.
IBS-like symptoms occurring during metformin therapy may be
misinterpreted as primary functional bowel disease, potentially
leading to unnecessary diagnostic investigations.Careful assessment of the temporal relationship between medication exposure and symptom onset is essential in identifying medication-related adverse effects.
Management strategies may include:
• Gradual dose titration
• Use of extended-release formulations
• Dietary modification
• Dose reduction or discontinuation
• Switching to alternative drug classes such as SGLT2 inhibitors or GLP-1 receptor agonists
Patient Perspective:
Following discontinuation of metformin and initiation of
dapagliflozin therapy, the patient reported significant relief from
gastrointestinal symptoms. He expressed satisfaction with the new
treatment regimen, noting improved daily comfort, reduced bowel
urgency, and better adherence to diabetes therapy. He was also able
to consume previously triggering foods such as spicy dishes, red meat,
and coffee without recurrence of gastrointestinal symptoms.Learning Points
1. Metformin remains the first-line therapy for type 2 diabetes but frequently causes gastrointestinal adverse effects.
2. In some patients, metformin intolerance may present with IBS-like symptoms such as abdominal pain, bloating, and diarrhea. 3. Symptoms may worsen after dose escalation of metformin.
4. Dietary triggers such as spicy foods, caffeine, and high-fat meals may exacerbate metformin-induced gastrointestinal symptoms.
5. Alternative therapies such as SGLT2 inhibitors can provide effective glycemic control in patients who cannot tolerate metformin.
Conclusion
Metformin-induced gastrointestinal intolerance may
occasionally present with IBS-like symptoms, particularly following
dose escalation. Clinicians should consider medication-related causes
when diabetic patients develop new-onset chronic gastrointestinal
complaints.
In this case, discontinuation of metformin and initiation of dapagliflozin successfully resolved gastrointestinal symptoms while maintaining adequate glycemic control. Recognition of metformin intolerance and timely adjustment of therapy can improve patient adherence, quality of life, and long-term diabetes management.
In this case, discontinuation of metformin and initiation of dapagliflozin successfully resolved gastrointestinal symptoms while maintaining adequate glycemic control. Recognition of metformin intolerance and timely adjustment of therapy can improve patient adherence, quality of life, and long-term diabetes management.
Informed Consent:
Written informed consent was obtained from the patient for
publication of this case report and any accompanying clinical
information.Conflict of Interest:
The author declares no conflict of interest related to this
manuscript.Ethical Considerations:
This case report was conducted in accordance with ethical
principles. Institutional approval was not required for a single
anonymized case report.References
Citation
Das S. Metformin-Induced Irritable Bowel Syndrome–Like Symptoms. J Clin Med Case Reports. 2026;10(1): 3.