
Research Article
*Address for Correspondence: Claudio Dello Russo, PhD, Department of Human Genetics, Altamedica, Fetal-Maternal Medical Centre, Rome, Italy, E-mail: claudio.dellorusso@artemisia.it
Citation: Russo CD, Giorlandino C, Mesoraca A. Prenatal Diagnosis of Vesicoureteral Reflux: Role of Combined Ultrasound Study and Next Generation Sequencing in Clinical Characterization. The Application of NGS in Prenatal Diagnosis. J Clin Med Case Reports. 2016;3(2): 5.
Copyright © 2016 Russo CD, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 3, Issue: 2
Submission: 16 November, 2016 | Accepted: 17 December, 2016 | Published: 24 December, 2016
 Through our analysis pipeline we identified a missense mutation in gene SOX17 located on chromosome 8q11 (SRY Sex Determining Region Y-Box 17; OMIM: 610928) c.775T>A (NM_022454.3), p.Tyr259Asn (NP_071899.1), previously described as vesicoureteral reflux 3 (VUR) causing (Figure 1) [2], compatible to clinical ultrasound phenotype.
Through our analysis pipeline we identified a missense mutation in gene SOX17 located on chromosome 8q11 (SRY Sex Determining Region Y-Box 17; OMIM: 610928) c.775T>A (NM_022454.3), p.Tyr259Asn (NP_071899.1), previously described as vesicoureteral reflux 3 (VUR) causing (Figure 1) [2], compatible to clinical ultrasound phenotype.

Prenatal Diagnosis of Vesicoureteral Reflux: Role of Combined Ultrasound Study and Next Generation Sequencing in Clinical Characterization. The Application of NGS in Prenatal Diagnosis
Claudio Dello Russo1*, Claudio Giorlandino2 and Alvaro Mesoraca1
- 1Department of Human Genetics, Altamedica, Fetal-Maternal Medical Centre, Rome, Italy
- 2Department of Prenatal Diagnosis, Altamedica, Fetal-Maternal Medical Centre, Rome, Italy
*Address for Correspondence: Claudio Dello Russo, PhD, Department of Human Genetics, Altamedica, Fetal-Maternal Medical Centre, Rome, Italy, E-mail: claudio.dellorusso@artemisia.it
Citation: Russo CD, Giorlandino C, Mesoraca A. Prenatal Diagnosis of Vesicoureteral Reflux: Role of Combined Ultrasound Study and Next Generation Sequencing in Clinical Characterization. The Application of NGS in Prenatal Diagnosis. J Clin Med Case Reports. 2016;3(2): 5.
Copyright © 2016 Russo CD, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 3, Issue: 2
Submission: 16 November, 2016 | Accepted: 17 December, 2016 | Published: 24 December, 2016
Abstract
Background: Pathophysiology and clinical prognosis of congenital anomalies of the kidney and urinary tract are known, especially in adult. Recent studies using massively sequencing approach in adult are clarifying genetic basis of these pathologies. Moreover a great attention is turning to antenatal diagnosis of kidney and urinary anomalies, as this could improve the prognosis after birth.Methods: Next Generation Sequencing methods, using extensive gene panel (4,800 genes) combined to pipeline for analysis and variant prioritization suited for prenatal diagnosis.
Results: we report a case of genetic and clinical characterization for fetal megacystis, revealed by ultrasound scan at 12 weeks of gestation. SOX17 gene variant, identified as causative for fetal megacystis, is already known for its pathogenic role in adult but was never described associated to fetal development. Furthermore, we introduce a Next Generation Sequencing method for a large number of disorders/genes analysis, with low incidental findings and variants of unknown significance risk, hence compatible to prenatal diagnosis.
Conclusions: In our study we showed the relevance of genetic characterizing of ultrasound sign, for clinical definition and good clinical management immediately after birth. The absence of any genetic diagnosis often precludes clinical interpretation and definition of fetal megacystis, since it may be associated to several disorders and genetic/chromosomal anomalies, with different pathological effects, also involving neuronal development. In these cases it is very challenging to determine the prognosis and pregnancy risks.
Keywords
Prenatal diagnosis; Next generation sequencing; Ultrasound; Vesicoureteral refluxBackground
Congenital anomalies of the kidney and urinary tract (CAKUTs) occur in about 5 per 1000 live births and featuring a wide variety of birth defects that occur at the level of the kidney (hypoplasia and dysplasia), bladder (ureterocele and vesicoureteral reflux), urethra (posteriorurethral valves) and collecting system (megaureter and hydronephrosis). Whereas in nonsyndromic CAKUT congenital structural anomalies are confined only to the kidney and urinary tract, syndromic CAKUTs may involve additional congenital abnormalities outside of the kidney and urinary tract. CAKUT is the main cause of chronic kidney disease in childhood and in young adults needing renal replacement therapy. A monogenic cause can be detected in around 12% of patients, however the latest whole exome studies are identifying new candidate genes [1].In prenatal diagnosis combination of ultrasound screening and massively genetic analysis methods could lead to clinical data characterization. In particular in recent years, a great effort has been made to introduce NGS methods in noninvasive prenatal testing both for the detection of common aneuploidies (associated to chromosomes 21, 18 and 13) and, in the latest studies, for single gene disorder analysis. We have introduced a new target resequencing NGS approach in prenatal diagnosis, called Next Generation Prenatal Diagnosis (NGPD), for the screening of a wide range of genetic disorders both in low and high-risk pregnancies when an ultrasound screening fails to show a definite clinical phenotype, in cases where ultrasound indications must be supported by a molecular genetic diagnosis, or in cases where one or both parents are carriers of a genetic disorder.
Methods
After copy number variation analysis performed by Array-CGH, prenatal sample was processed by Next Generation Sequencing. We described NGPD method in a previous paper [3]. Shortly, for library preparation we used an extensive gene panel (Trusight One Sequencing Panel, Illumina), which enriches for 62 000 exons of 4813 genes selected for direct genetic disorder association.Sequencing and primary data analysis were performed on NextSeq500 platform. Basespace on site software (Illumina) performed the secondary analysis on the base calls and produced a Phred-like quality score (Qscore) generated by Real Time Analysis software (RTA) during the sequencing run. The Trusight one sequencing panel workflow performed the demultiplexing of indexed reads, generated FASTQ files, aligned reads to a reference, identified variants and wrote output files for the alignment folder. Single nucl eotide polymorphisms (SNPs) and short indels were identified using the Genome Analysis Toolkit (GATK), by default. Based on the guidelines of the American College of Medical Genetics and Genomics, all regions that have been sequenced with a sequencing depth < 30 were considered unsuitable for analysis. Furthermore, we established a minimum threshold in Qscore of 30 (base call accuracy of 99.9%). After Trusight One library sequencing, the first step of analysis was focused on a panel of genes, defined the NGPD pane l (Table 1), that we selected for their direct associatio n with Mendelian disorders, their clinical significance, severity and incidence in population. The disorders and groups of disorders included neuromuscular, cardiomyopathic and osteochondroplastic diseases and diseases involved in fetal development. In order to carry out only variants w ith pathogenic and characterized annotation, we used the Variant Studio software (Illumina) in combination with software developed in our center (NGPD software) which allows matching of VCF file to main annotation database (HGMD professional, ClinVar and the OMIM NCBI database).
Results
In present case, ultrasound scan at 12 weeks of gestation has led to the early diagnosis of fetal megacystis (Figure 1). In the ultrasound scanning of the abdominal region a cystic structure was detected with a maximum longitudinal diameter of 7.7 mm. The parents decided for chorionic villous sampling (CVS). The amniotic fluid volume was normal, ultrasound study during pregnancy has not revealed aberrations in other tissues and the fetal karyotype of the fetal chorionic villous cells showed normal female fetus.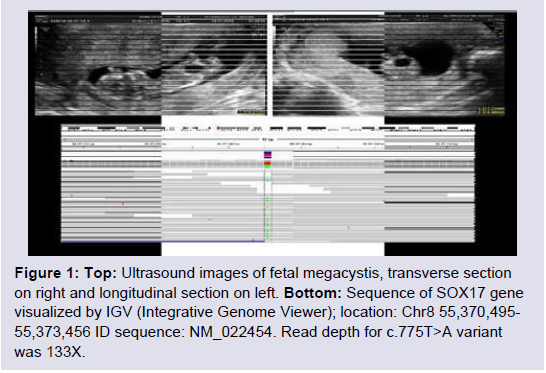
Figure 1: Top: Ultrasound images of fetal megacystis, transverse section on right and longitudinal section on left. Bottom: Sequence of SOX17 gene visualized by IGV (Integrative Genome Viewer); location: Chr8 55,370,495-55,373,456 ID sequence: NM_022454. Read depth for c.775T>A variant was 133X.
For high-risk pregnancy cases, we perform further investigation to verify possible presence of variants not yet described in the literature but associated to genes potentially involved in clinical phenotype. For this purpose we used the VarElect-NGS Phenotyper software entering all the genes carried mutations (about 400) found after sequencing and using for gene prioritization disorders associated with kidney, urinary tract and bladder. This analysis showed high association score to Sox17, ACE (Angiotensin I Converting Enzyme), FGFR3 (Fibroblast Growth Factor Receptor 3) and ADRA1A (Adrenoceptor Alpha 1A). However variants found on these genes were described as benign in scientific literature, confirming p.Tyr259Asn in Sox17 gene as only pathogenic variant.
Finally, in order to determine the inheritance pattern of mutation we performed a TRIO study. p.Tyr259Asn was absent in father and transmitted from mother. It was not possible verify VUR as she never performed cystography, however patient presenting an history of recurrent urinary tract infection. Moreover incomplete penetrance, variability of expression and environment effects are described as characteristic features of VUR.
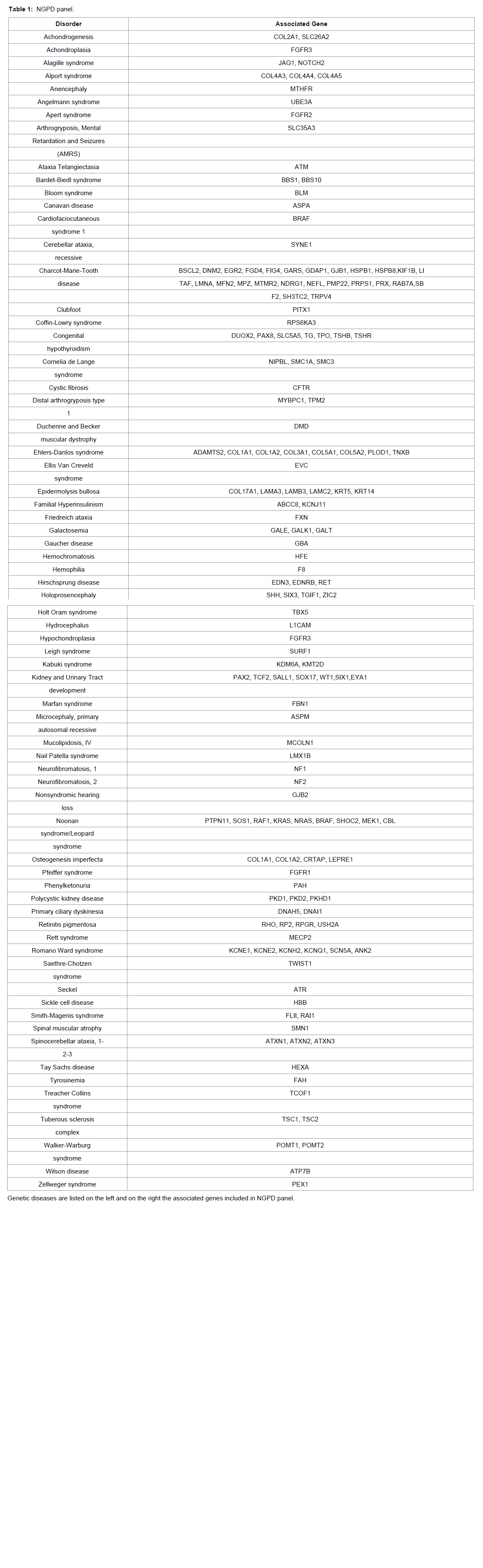
Table 1: NGPD panel.
Discussion
Fetal megacystis at 10-14 weeks has a prevalence of 1-1500 pregnancies and the onsets are classified in obstructive and not obstructive causes [4]. Obstructive causes determinate obstruction to the flow of urine out of the bladder. In male fetus, bladder obstruction are mostly associated to urethra maldevelopment. Instead, in female bladder obstruction is associated to complex defects in urogenital system development. Non-obstructive causes, form a heterogeneous group, often with complex underlying pathologies, chromosomal defects and genetic syndrome like Prune Belly Syndrome, megacystis, megaureter, megacystis-microcolon-hypoperistalsis syndrome, neurogenic bladder, and primary vesicoureteral reflux.Using a target resequencing NGS method specifically designed for prenatal diagnosis, based on analysis pipeline which allows the filtering for known and well-characterized genetic variants, we identified a missense variant on SOX17 gene, previously described as pathogenic in adult.
Human tissues analysis [5] has detected the main SOX17, a SOX family member transcription factor, expression in adult heart, lung, spleen, testis, ovary, placenta, and in fetal lung and kidney. Tyr259Asn variant in Sox17 gene induces an increase of the protein levels, responsible of Wnt signaling pathway inhibition during kidney and urinary tract development causing congenital defects. Wnt pathway underlies embryonic processes as cell fate determination, cell proliferation and migration, and determines the arrangement of the organs on the right or left of embryonic medial axis. These processes are necessary for the proper formation of tissues such as bones, heart, muscles and in nephrogenesis [6].
Identification of Sox17 Tyr259Asn variant associated to clinical phenotype, and family inheritance pattern studies, were essential to exclude the presence of other syndromes associated to bladder abnormalities and to determine future pregnancies risk factor. The diagnosis of megacystis exclusively by ultrasound would not have been able to determine causes and prognosis for pregnancy. After birth will be possible to establish the grade of severity of vesicoureteral reflux, and based on this evaluation it will be possible to determine the most appropriate intervention.
Children with low grade of severity do not need any kind of intense therapy and the reflux will be corrected during growth. Mild grade of VUR leads to frequent fevers or infections may require ongoing preventive antibiotic therapy. Only high grade reflux may require surgical intervention.
Conclusion
High association to urinary tract infections and permanent renal damage, make reflux-associated nephropathy one of the most frequent causes of end stage renal disease and kidney transplantation in children and adults; nevertheless most of VUR are diagnosed only after recurrent urinary tract infection, condition that increase risk of renal damage. Prenatal diagnosis should allow management of VUR immediately after birth, improving the clinical prognosis in adult.Next Generation Prenatal Diagnosis method and prioritized method used for data analysis, combined to ultrasound, enabled genetic characterization of clinical signs in compatible manner to limited quantity and quality of the DNA obtained from fetal sample and to times foreseen in prenatal diagnostics. For low-risk pregnancy cases, analysis exclusively focused on previously characterized variants in interest genes, by scientific literature and database, can prevent incidental findings and data with conflicting significance. In high-risk cases, however, a further study may be required through genes prioritization according to ultrasonographic phenotype and family study, in order to verify the presence of variants not yet described, with presumed pathogenic effects (eg. stop gained, frameshift mutation).
Ethics approval and consent to participate: Diagnosis, privacy and confidentiality conditions, and informed consent were approved from Ethical Board of Altamedica Fetal-Maternal Medical Centre institute, director Prof. Claudio Giorlandino – CEO, in accordance with World Medical Association’s Declaration of Helsinki and SIGU (Italian Society of Human Genetics) guidelines.
References
- Renkema KY, Stokman MF, Giles RH, Knoers VA (2014) Next-generation sequencing for research and diagnostics in kidney disease. Nat Rev Nephrol 10: 433-444.
- Gimelli S, Caridi G, Beri S, McCracken K, Bocciardi R, et al. (2010) Mutations in SOX17 are associated with congenital anomalies of the kidney and the urinary tract. Hum Mutat 31: 1352-1359.
- Dello Russo C, Padula F, Di Giacomo G, Mesoraca A, Gabrielli I, et al. (2015) A new approach for Next Generation Sequencing in prenatal diagnosis applied to a case of Charcot-Marie-Tooth syndrome. Prenat Diagn 35: 1018-1021.
- Bornes M, Spaggiari E, Schmitz T, Dreux S, Czerkiewicz I, et al. (2013) Outcome and etiologies of fetal megacystis according to the gestational age at diagnosis. Prenat Diagn 33: 1162-1166.
- Ayatollahi M , Sanati MH, Kabir Salmani M, Geramizaeh B (2012) Differential expression pattern of the human endoderm-specific transcription factor sox17 in various tissues and cells. Int J Organ Transplant Med 3: 183-187.
- Halt K, Vainio S (2014) Coordination of kidney organogenesis by Wnt signaling. Pediatr Nephrol 29: 737-744.