
Case Report
*Address for Correspondence: Gulin Feykan Yegin Akcay, Department of Gynecology and Obstetrics, Atatürk Education and Research Hospital, Ufuk Universitesi Cad.No: 30/30 Cukurambar, Ankara, Turkey, Tel: +90 312 291 25 25; Fax: +90 312 291 27 26; E-mail:gulin_yegin@hotmail.com
Citation: Yavuz AF, Akcay GFY, Kara H, Tas EE, Keskin HL. Autoimmune Progesterone Dermatıtıs durıng Pregnancy Results in a Full-Term Delivery. J Clin Med Case Reports. 2016;3(1): 3.
Copyright: © 2016 Yavuz AF, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 3, Issue: 1
Submission: 28 April, 2016 | Accepted: 06 May, 2016 | Published: 11 May, 2016
 At 13 weeks gestation, the patient no longer had pain due to cutaneous lesions, and, within one month, she noted a dramatic improvement in her urticarial and angioedema. Until the date of delivery, had no complaints and was free from obstetric complications during her antenatal care. At 39 weeks gestation, the patient delivered a 3,580-gram infant, with initial and 5 min Apgar scores of 8 and 10, respectively. The patient did not experience any complications during the intrapartum or postpartum period. While brea stfeeding and at postpartum follow-up, the patient continued with cetirizine (10 mg/day) without any episodes of skin lesions. In the first year of followup, the patient was treated with 1,000 mg medroxyprogesterone acetate by intramuscular injection once every three months, and she had no complaints or episodes of lesions for 18 months.
At 13 weeks gestation, the patient no longer had pain due to cutaneous lesions, and, within one month, she noted a dramatic improvement in her urticarial and angioedema. Until the date of delivery, had no complaints and was free from obstetric complications during her antenatal care. At 39 weeks gestation, the patient delivered a 3,580-gram infant, with initial and 5 min Apgar scores of 8 and 10, respectively. The patient did not experience any complications during the intrapartum or postpartum period. While brea stfeeding and at postpartum follow-up, the patient continued with cetirizine (10 mg/day) without any episodes of skin lesions. In the first year of followup, the patient was treated with 1,000 mg medroxyprogesterone acetate by intramuscular injection once every three months, and she had no complaints or episodes of lesions for 18 months.
Autoimmune Progesterone Dermatitis during Pregnancy Results in a Full-Term Delivery
Ayse Filiz Yavuz1, Gulin Feykan Yegin Akcay2*, Halil Kara3, Emre Erdem Tas1 and Huseyin LeventKeskin2
- 1Department of Gynecology and Obstetrics, Yıldırım Beyazıt University, Ankara, Turkey
- 2Department of Gynecology and Obstetrics, Atatürk Education and Research Hospital, Ankara, Turkey
- 3Department of Pharmacology, Yildirim Beyazit University, Ankara, Turkey
*Address for Correspondence: Gulin Feykan Yegin Akcay, Department of Gynecology and Obstetrics, Atatürk Education and Research Hospital, Ufuk Universitesi Cad.No: 30/30 Cukurambar, Ankara, Turkey, Tel: +90 312 291 25 25; Fax: +90 312 291 27 26; E-mail:gulin_yegin@hotmail.com
Citation: Yavuz AF, Akcay GFY, Kara H, Tas EE, Keskin HL. Autoimmune Progesterone Dermatıtıs durıng Pregnancy Results in a Full-Term Delivery. J Clin Med Case Reports. 2016;3(1): 3.
Copyright: © 2016 Yavuz AF, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 3, Issue: 1
Submission: 28 April, 2016 | Accepted: 06 May, 2016 | Published: 11 May, 2016
Abstract
Autoimmune progesterone dermatitis (APD) is a rare disease that may first appear, worsen, or improve during pregnancy. We report a case of a 37-year-old primigravid woman who was referred to our clinic eight weeks pregnant with complaints of urticarial plaques on her lower extremities. As there were no obstetric complications, she was prescribed cetirizine (10 mg/day) treatment with follow-up. However, during the follow-up at 10 weeks gestation, she was admitted to the hospital with multiple aggravated erythematous lesions. Her symptoms were controlled with cetirizine (10 mg/day) and prednisone (40 mg/day) together for one week. At 13 weeks gestation, she no longer had pain associated with cutaneous lesions, and, within one month, she noted a dramatic improvement in her urticaria. She had no further complaints, and delivered a 3,580-gram infant at 39 weeks gestation, with initial and 5 min Apgar scores of 8 and 10, respectively. The patient did not have any complications during the intrapartum or postpartum periods. These findings suggest that APD symptoms and attacks can be controlled or avoided during pregnancy with proper medication and follow-up.Keywords
Autoimmune; Dermatitis; Pregnancy; ProgesteroneIntroduction
Autoimmune progesterone dermatitis (APD) is a rare disease characterized by cyclical premenstrual flares of cutaneous and mucocutaneous manifestations caused by an immune reaction to endogeneous progesterone or exogenous exposure to progesterone in medications [1]. Skin lesions typically occur due to increased progesterone during the luteal phase of the menstrual cycle [2]. Clinical symptoms are frequently confused with other forms of dermatosis [3]. We present a case study of a pregnant woman with APD who had a full-term delivery.Case Report
A 37-year-old primigravid woman was referred to our clinic during her eighth week of pregnancy with complaints of urticarial plaques on her lower extremities. In her medical history, she noted that her urticarial lesions began at the age of 28 years, with episodes always occurring during the second half of her menstrual cycle. Each individual lesion would last from 12-24 hours, and her overall symptoms would last from 5-10 days. The lesions would usually start on her chest and then spread over her entire body. The results of multiple laboratory tests taken over the years had been unremarkable. Tests included measurements of corticotropin releasing hormone levels, adrenocorticotropic hormone levels, angiotensin levels, anti- Ro/SSA antibodies, anti-Smith antibodies, C3/C4 complement tests, hepatitis panel, anti-anti-nuclear antibodies, anti-doublestranded DNA antibodies, serum protein electrophoresis, C1 esterase inhibitor levels and function, chemistry panel, liver tests, thyroid stimulating hormone (TSH) level, anti-thyroid antibody levels, rheumatoid factor levels, erythrocyte sedimentation rate (ESR), and complete blood count (CBC). A skin prick test was negative, and an intradermal test using 50 mg/ml progesterone at dilutions of 1:10 and 1:1 showed a positive response. A skin biopsy of one of the lesions had been diagnosed as “chronic urticaria”. Based on all of these examinations, the patient was diagnosed with APD. She had seen by multiple physicians, including allergists and dermatologists, and had been treated with a variety of medications, including cetirizine, desloratadine, hydroxyzine, montelukast, ranitidine, and diphenhydramine, without relief. Finally, follow-up visits with intramuscular injection of medroxyprogesterone acetate (1,000 mg) once every three months successfully limited her symptoms until she became pregnant.The patient was evaluated when she was eight weeks pregnant, and did not show any obstetric complications. She was examined in the dermatology clinic, and follow-up with cetirizine (10 mg/day) was recommended. However, she was admitted during her followup visit to our clinic at 10 weeks gestation with multiple aggravated erythematous lesions ranging in size from size of 3 x 1 cm to 10 x 8 cm on her upper arm, chest, and lower extremities (Figure 1). A CBC showed hemoglobin 9.8 g/dl, hematocrit 28%, white blood cell 10,000/ μL (eosinophils 600/μL), and platelets 250,000/μL. Liver and thyroid function tests were within normal limits. Because of the gestational week, treatment options were limited and the patient was followed while treated with cetirizine (10 mg/day) and prednisone (40 mg/day) for one week. During the first week, as patient’s outbreaks steadily decreased in intensity, we decreased the prednisone dose each day (10 mg/day) and stopped the prednisone on the fourth day.
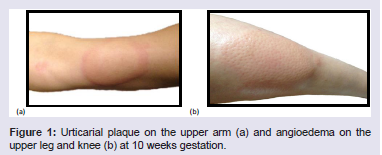
Figure 1: Urticarial plaque on the upper arm (a) and angioedema on the upper leg and knee (b) at 10 weeks gestation.
Discussion
The menstrual cycle has been associated with a variety of skin eruptions, including eczema, prurigo, erythema multiforme, stomatitis, bullous-vesiculo pustuler eruptions, folliculitis, angioedema, and urticarial plaques [4-6]. APD is a rare disorder characterized by recurrent skin manifestations during the luteal phase of the menstrual cycle [6]. The first documented case of APD was in 1921, in which a patient’s premenstrual serum caused acute urticarial lesions [7].The clinical symptoms of APD correlate with progesterone levels, usually beginning at 3-10 days before menstruation and ending at 1-2 days into the menstrual flow. Common presentations of APD include: urticaria, erythema multiforme-like lesions, eczema, petechiae, purpura and vesiculobullous reactions [6]. In the literature, laryngeal edema, hypotension, bronchospasm, and anaphylactic reactions have been described; however these cases are definitely rare [8]. Some studies have noted that the majority of APD patients had taken an oral contraceptive prior to the onset of APD; however, in multiple cases, women with APD have never been exposed to exogenous progesterone, as in this case [5,8,9]. There are no specific histological features on biopsy in APD, and it is usually noted as ‘chronic urticaria’ [8].
The diagnostic criteria for APD proposed by Warin include: skin lesions related to menstrual cycle; positive response to intradermal testing with progesterone; and symptomatic improvement after inhibiting progesterone secretion by suppressing ovulation [10]. During pregnancy, especially in cases not previously diagnosed, the typical history must warn us about APD.
Out of 89 APD cases in the literature, 13 have been reported as related to a pregnancy, and seven of them occurred during the postpartum period [8]. Pregnancy can complicate or improve the symptomatology of APD. In one case report, APD during pregnancy was associated with spontaneous abortion of a 10-week pregnancy [11]. Pregnancy is associated with an increase in maternal progesterone levels by 10-5,000 times relative to non-pregnancy levels, which may explain the initiation or worsening of APD symptoms [4].
On the other hand, there is a group of APD patients without complaints or with improvements in their APD symptoms during pregnancy. In this group, improvements in APD symptoms can be explained by the theories suggesting that the slow rise of progesterone during pregnancy serves as a method of desensitization, a decrease in the maternal immune response during pregnancy, or an increased production of anti-inflammatory glucocorticoids [9].
APD is usually resistant to antihistamines. Because of drug safety issues, we have limited options during pregnancy, and antihistamines are first-line therapy. The use of systemic glucocorticoids has been reported to control the cutaneous lesions of APD is some studies, but their use is controversial during pregnancy, especially in high doses [5,8]. The most common approach is to give these agents only during periods of attacks and at as low of a dose as possible during pregnancy. Other therapy alternatives are designed to induce ovarian suppression (hormonal contraceptives, GnRHa), but they cannot be used during pregnancy because of fetal toxicity.
During the postpartum period, oral contraceptives can be used as an initial therapy, but they show limited success, possibly due to the progesterone component [5]. Conjugated estrogens have also been used for the treatment of APD, however, due to increased risk of endometrial carcinoma, this treatment is not commonly used today [4]. During the prepartum and postpartum periods, desensitization with progesterone is another treatment option, as shown in this case. However, reports in the literature have shown that latent autoimmunity may be aggravated in genetically predisposed women [5].
Gonadotropin releasing hormone (GnRH) agonists, such as buserelin and triptorelin, have been used to induce remission of APD symptoms by causing ovarian suppression, but this approach may require estrogen supplementation during therapy because of deficiency [8]. During the perimenstrual period, alkylated steroids, such as stanozol and danazol, have been used successfully to suppress ovulation, sometimes in combination with low doses of corticosteroids [5]. Tamoxifen is another therapeutic option used in APD, and, as with GnRH agonists, patients treated with tamoxifen may experience symptoms of estrogen deficiency [8]. In addition, tamoxifen treatment has been associated with an increased risk of venous thrombosis and cataract formation [5]. In some patients that are refractory to medical treatment, bilateral oophorectomy has been required [7,8]. While this definitive treatment has been successful in controlling symptoms, it is rarely used today, unless all other medical options have been exhausted.
Conclusion
APD may first appear, worsen, or improve in pregnancy. The best approach to APD treatment during pregnancy depends on the gestational stage, but should include regular follow-ups and suitable choices of medications to control symptoms and avoid attacks.References
- Aksoy FC, Evans SE, Karaduman A (2009) Autoimmune progesterone dermatitis: A case report and review of literature. Turkderm 43: 122-125.
- George R, Badawy SZ (2012) Autoimmune progesterone dermatitis: a case report. Case Rep Obstet Gynecol 2012: 1-2.
- Lahmam Bennani Z, El Fekih N, Baccouche D, Khaled A, Zaglaoui F, et al. (2012) Autoimmune progesterone dermatitis, Ann Dermatol Venereol 139: 832-835
- Baptist AP, Baldwin JL (2004) Autoimmune progesterone dermatitis in a patient with endometriosis: case report and review of the literature. Clin Mol Allergy 2: 10.
- Solomon M, Itsekson AM, Lev-Sagie A (2013) Autoimmune progesterone dermatitis. Curr Dermatol Rep 2: 258-263.
- Geber H (1921) IV. Einige daten zur pathologic der urticaria menstruationalis. Dermatol J 32: 143-150.
- Snyder JL, Krishnaswamy G (2003) Autoimmune progesterone dermatitis and its manifestation as anaphylaxis: a case report and literature review. Ann Allergy Asthma Immunol 90: 469-477.
- Nguyen T, Razzaque Ahmed A (2016) Autoimmune progesterone dermatitis: update and insights. Autoimmun Rev 15: 191-197.
- George R, Badawy SZ (2012) Autoimmune progesterone dermatitis: a case report. Case Rep Obstet Gynecol 2012: 757854.
- Warin AP (2001) Case 2. Diagnosis: erythema multiforme as a presentation of autoimmune progesterone dermatitis. Clin Exp Dermatol 26: 107-108.
- Wojnarowska F, Greaves MW, Peachey RD, Drury PL, Besser GM (1985) Progesterone-induced erythema multiforme. J R Soc Med 78: 407-408.