
Case Report
*Address for Correspondence: Ang Peng Wong, MSc, Cyberjaya University College of Medical Sciences, No 3410, Jalan Teknokrat 3, Cyber 4, 63000 Cyberyaya, Selangor, Malaysia, Tel: +6013-3399898; E-mail: wongangpeng@hotmail.com
Citation: Wong AP, Mohamed AL. Congestive Heart Failure Treated with a Multiple Micronutrient Supplement Program: A Case Report. J Clin Med Case Reports. 2015;2(2): 3.
Copyright © 2015 Wong et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 2, Issue: 2
Submission: 29 September 2015 | Accepted: 07 November 2015 | Published: 12 November 2015
 Quality of life outcome measure
Quality of life outcome measure
Congestive Heart Failure Treated with a Multiple Micronutrient Supplement Program: A Case Report
Ang Peng Wong* and Abdul Latiff Mohamed
- Cyberjaya University College of Medical Sciences, Cyberjaya, Selangor, Malaysia
*Address for Correspondence: Ang Peng Wong, MSc, Cyberjaya University College of Medical Sciences, No 3410, Jalan Teknokrat 3, Cyber 4, 63000 Cyberyaya, Selangor, Malaysia, Tel: +6013-3399898; E-mail: wongangpeng@hotmail.com
Citation: Wong AP, Mohamed AL. Congestive Heart Failure Treated with a Multiple Micronutrient Supplement Program: A Case Report. J Clin Med Case Reports. 2015;2(2): 3.
Copyright © 2015 Wong et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 2, Issue: 2
Submission: 29 September 2015 | Accepted: 07 November 2015 | Published: 12 November 2015
Abstract
Congestive heart failure is a chronic progressive disorder of the cardiovascular system with loss of function of the cardiac myocytes. There is no cure and treatments only attempt to reduce the severity of symptoms. We present a case of a 50-year-old female that presented to the clinic with congestive heart failure with idiopathic primary pulmonary hypertension and New York Heart Association (NYHA) functional class IV. After adhering for eight months to the prescribed multiple micronutrient supplement program as an adjunct to conventional medication the patient experienced much improvement as measured by the Minnesota Living with Heart Failure Questionnaire (MLHFQ) and the 6-Minute Walk Test (6MWT).Keywords
Congestive heart failure; NYHA; MLHFQ; 6MWTIntroduction
Heart failure (HF) is a progressive cardiovascular disorder where there is loss of function of the cardiac myocytes. The classical definition of HF by Braunwald is that it is the pathological state in which an abnormality of myocardial function is responsible for the failure of the heart to pump blood at a rate commensurate with the requirements of the metabolizing tissue during ordinary activity [1]. HF patients may present with a wide variety of conditions ranging from asymptomatic with mild echocardiographic abnormalities to those with unstable angina and acute pulmonary edema. However, the prime manifestations of HF are dyspnea and fatigue, which may limit exercise tolerance and cause fluid retention, which may lead to pulmonary congestion and peripheral edema [2]. For this reason, HF is also commonly referred to as congestive heart failure (CHF).Patients with CHF are often treated with angiotensin-converting enzyme inhibitors, beta-blockers, calcium channel blockers, nitrates, statins, and diuretics. Despite advances in treatment options, patients with HF continue to have high morbidity and mortality [3]. Approximately 50% of the patients die within five years of the initial diagnosis [3].
In this report, we describe the case of a patient presenting with severe CHF and the result of treatment with a high dose multiple micronutrient supplement program.
Case Report
A 50-year-old woman presented to our integrated healthcare center in September 2014, with orthopnea, ankle swelling, and angina. Her blood pressure was 95/55 mmHg. She was diagnosed HF with idiopathic primary pulmonary hypertension in March 2013 with New York Heart Association (NYHA) functional class IV.An echocardiography on August 27, 2014 showed left ventricular ejection fraction (LVEF) of 58% with no evidence of hypertrophy or abnormality in the systolic function. The inferior vena cava was dilated. The right atrium was also dilated. There was presence of right ventricular strain. There was minimal pericardial effusion at anterior right ventricle and lateral right ventricle. An ultrasonography on August 29, 2014 showed mild hepatomegaly with dilatation of the inferior vena cava and hepatic veins, multiple hepatic and splenic calcifications, and right pleural effusion and minimal ascites. CECT thorax on September 2, 2014 showed right cardiac insufficiency secondary to pulmonary arterial hypertension with liver congestion, pulmonary veno-occlusion, right pleural effusion, and pericardial effusion.
The patient was on the following medications:
1. Sildenafil 25 mg – twice daily
2. Furosemide 40 mg – twice daily
3. Spironolactone 12.5 mg – twice daily
4. Potassium chloride 600 mg – twice daily
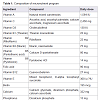
The patient was prescribed a specific multiple micronutrient supplement program taken three times a day, in addition to twice daily pharmaceutical medications. Table 1 shows the list of micronutrients in the supplement program.
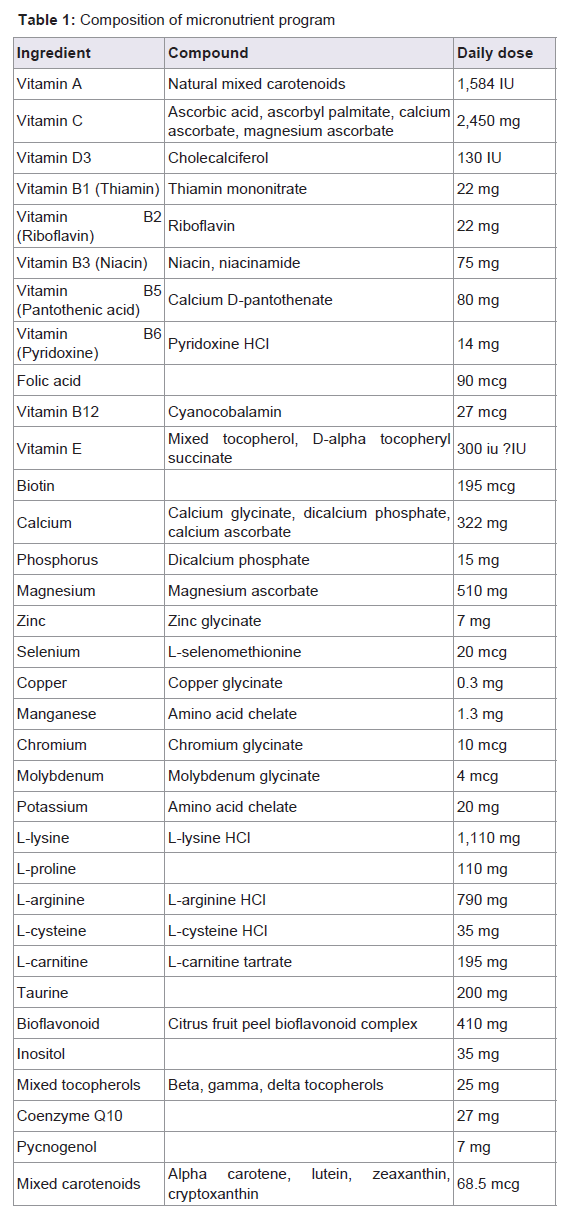
Table 1: Composition of micronutrient program.
In conjunction with the objective therapeutic measures, this case study utilized a quality of life (QOL) measure, the Minnesota Living with Heart Failure Questionnaire (MLHFQ), for therapeutic outcome. The MLHFQ is a validated patient-reported outcome measurement tool used in measuring patient-perceived changes in symptoms, functional limitations, and psychological distress scored on a 0 to 5 Likert scale. The measures were combined to provide scoring by two dimensions (physical function and emotional), and an overall profile score (global) that allowed for quantifiable assessment of overall change over time. The MLHFQ was used to record severity during the initial case taking and on each scheduled monthly return visit. A positive change of 5 points in the MLHFQ would have a clinically significant effect [4].
Clinical progression
Compliance with the nutritional supplement program was monitored during each follow-up visit. After one month of the intervention, the patient felt more energetic. However, stiffness and pain in the fingers that was present on admission were aggravated. There was no improvement in all other symptoms. After two months, edema in the lower extremities, angina, and orthopnea were much reduced. During the third month, the patient was admitted to the hospital due to a high fever, which aggravated her symptoms. Four months after therapy the patient was able to walk without symptoms, and was able to perform light work. Symptoms improved further after eight months and patient assessment revealed that she was in NYHA class I.
6 minute walk test
The initial 6-minute walk test (6 MWT) was conducted and the patient had to stop at 5 minutes after covering a distance of 75 meters in the hospital ward corridor. Blood pressure (BP) changed from 126/58 to 115/72 mmHg. The pulse rate increased from 80 to 113 beats per minute. After eight months of the nutritional supplement intervention, another 6 MWT showed an improvement and the patient was able to complete the 6 MWT and covered a distance of 450 meters. BP increased from 95/65 to 110/75 mmHg and her pulse rate increased from 71 to 88 beat per minute.
Data from MLHFQ
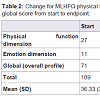
The patient was followed for eight months and at the endpoint she was still on the treatment protocol. During each monthly follow-up visit the MLHFQ was applied. The patient answered all 21 questions in the questionnaire. For the first six months only the English version of the MLHFQ was used. During the seventh and eighth months the Malay version was also used. The answers derived from the Malay version did not differ from the answers given in the English version or those given in the first six months. Table 2 summarizes the results of the MLHFQ for physical function and emotional dimensions, as well as the global or overall profile scores.
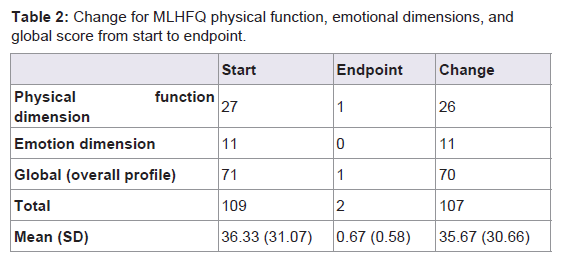
Table 2: Composition of micronutrient program.
Discussion
The patient was initially on appropriate medications for CHF but her condition continued to deteriorate over the next two years. From the MLHFQ data, there was a positive change in score for physical function dimension (26 points), emotional dimension (11 points), and overall profile (70 points). The mean change for the three dimensions was 35.67 ± 30.66. Rector and colleagues had suggested that a positive change of 5 points or more for the total score would be considered as clinically significant [4]. In this case study, the change of total overall score of 70 points is much higher than the 5 points suggested.This case study used a high (above the RDAs) dosage of the multiple micronutrients. It also used multiple amino acids such as L-lysine, L-proline, L-arginine, L-carnitine, L-cysteine, and taurine, which are important nutrients for cardiac functions.
Furthermore, the vitamin C dosage used in this study was also high. Vitamin C is important, and it has been shown in a large-scale observational study that the risk of HF decreases with increasing plasma vitamin C [5]. Furthermore, the use of vitamin C, lysine and proline is crucial for production of collagen and protection of the endothelium of the artery walls [6].
An important indication of good prognosis is that the patient feels more energetic even though the pathological symptoms may aggravate or show no sign of improvement. This was shown to be present in this study. Taegtmeyer has postulated that the deprivation of cardiac bioenergy has a major role in HF [7]. The heart consumes more energy than any other organ. This bioenergy is provided by the biochemical conversion of glucose and fatty acids into mechanical energy supporting the heart muscle functions.
The use of the Malay version together with the English version of the MLHFQ in this case study supports its validation. To our knowledge, there has been no other study on HF that has used the Malay version of the MLHFQ.
This clinical study has some limitations. Top among those is that it relies primarily on MLHFQ and 6MWT as outcome measures. It would have been better if the pulmonary vascular resistance were also measured for pre and post treatment comparison. Availability of data on hemoglobin and liver function would have strengthened the observations, but not.
In conclusion, this case study suggests that a large randomized control study could be beneficial to assess the use of a multiple micronutrient supplement program as an adjunct to conventional treatment for CHF due to primary pulmonary hypertension. More studies are needed to investigate the efficacy and safety of the nutrients.
Acknowledgements
We thank Dr. Aleksandra Niedzwiecki, Dr. Bilwa Bhanap, and Cathy Flowers for editorial and proofreading assistance.References
- Braunwald E, Ross J Jr, Sonnenblick EH (1967) Mechanisms of contraction of the normal and failing heart. N Engl J Med 277: 1012-1022 concl.
- Hunt SA; American College of Cardiology; American Heart Association Task Force on Practice Guidelines (2005) ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol 46: e1-e82.
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, et al. (2012) Heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation 125: e2-e220.
- Rector TS, Tschumperlin LK, Kubo SH, Bank AJ, Francis GS, et al. (1995) Use of the Living With Heart Failure questionnaire to ascertain patients' perspectives on improvement in quality of life versus risk of drug-induced death. J Card Fail 1: 201-206.
- Pfister R, Sharp SJ, Luben R, Wareham NJ, Khaw KT (2011) Plasma vitamin C predicts incident heart failure in men and women in European Prospective Investigation into Cancer and Nutrition-Norfolk prospective study. Am Heart J 162: 246-253.
- Rath M (1992) Reducing the risk for cardiovascular disease with nutritional supplements. J Orthomol Med 7: 153-162.
- Taegtmeyer H (2004) Cardiac metabolism as a target for the treatment of heart failure. Circulation 110: 894-896.