
Journal of Clinical & Medical Case Reports
Download PDF
Case Report
*Address for Correspondence: Sarveswaran.V, Head of Department and Consultant, General Surgery, Sri Ramakrishna Hospital, 395, Sarojini Naidu Road, Sidhapudur, Coimbatore, Tamilnadu-641044, India, Tel: +(91)9842217268/+(91)4224500138; Fax: +(91)422-2240521; E-mail: sarvesh_59@yahoo.co.in
Citation: Sarveswaran V, Kumar S, Kumar R, Kumar A, Vamseedharan M. Spontaneous Perinephric Haemorrhage (Wunderlich Syndrome) Secondary to Upper Pole Renal Angiomyolipoma: A Rare Life Threatening Situation. J Clin Med Case Reports. 2015;2(1): 3.
Copyright © 2015 Sarveswaran et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN 2332-4120 | Volume: 2, Issue: 1
Submission: 09 January 2015 | Accepted: 23 January 2015 | Published: 28 January 2015
Reviewed & Approved by: Dr. Xu Zeng, Associate Professor, Department of Pathology and Laboratory Medicine, Temple University, USA
 The second set of blood investigations showed a drop in haemoglobin (6 g/dl) and haematocrit (21%). Blood transfusions were given and after stabilising the haemoglobin levels, the patient was planned for partial nephrectomy. But the surgical dissection was faced with difficulty in the form of torrential haemorrhage which could not be controlled, making it necessary to perform pedicle ligation and left total nephrectomy (Figure 2).
The second set of blood investigations showed a drop in haemoglobin (6 g/dl) and haematocrit (21%). Blood transfusions were given and after stabilising the haemoglobin levels, the patient was planned for partial nephrectomy. But the surgical dissection was faced with difficulty in the form of torrential haemorrhage which could not be controlled, making it necessary to perform pedicle ligation and left total nephrectomy (Figure 2).
 On gross analysis, the mass was made up of a large hematoma enclosed within the perinephric space [Figure 3] and a ruptured yellowish mass arising from the upper pole of the left kidney. Microscopic examination revealed that the lesion arising from the upper pole of kidney was composed of triphasic components- islands of mature adipose tissue, myoid spindle cells and dysmorphic thick blood vessels in a haemorrhagic background. Immunohistochemical staining with HMB- 45 confirmed the neoplasm to be a benign angiomyolipoma (Figure 3).
On gross analysis, the mass was made up of a large hematoma enclosed within the perinephric space [Figure 3] and a ruptured yellowish mass arising from the upper pole of the left kidney. Microscopic examination revealed that the lesion arising from the upper pole of kidney was composed of triphasic components- islands of mature adipose tissue, myoid spindle cells and dysmorphic thick blood vessels in a haemorrhagic background. Immunohistochemical staining with HMB- 45 confirmed the neoplasm to be a benign angiomyolipoma (Figure 3).
 The postoperative period was uneventful and the patient was discharged on ninth postoperative day. With 6 months completed after treatment, he is doing well.
The postoperative period was uneventful and the patient was discharged on ninth postoperative day. With 6 months completed after treatment, he is doing well.
Spontaneous Perinephric Haemorrhage (Wunderlich Syndrome) Secondary to Upper Pole Renal Angiomyolipoma: A Rare Life Threatening Situation: Case Report and Discussion
Sarveswaran.V1*, Urees Kumar2, Ravi Kumar3, ArunKumar3 and Vamseedharan.M3
- 1Head of Department and Consultant, General Surgery, Sri Ramakrishna Hospital, Tamilnadu, India
- 2Consultant, Department of General Surgery, Sri Ramakrishna Hospital, Tamilnadu, India
- 3NB Trainee, Department of General Surgery, Sri Ramakrishna Hospital, Tamilnadu, India
*Address for Correspondence: Sarveswaran.V, Head of Department and Consultant, General Surgery, Sri Ramakrishna Hospital, 395, Sarojini Naidu Road, Sidhapudur, Coimbatore, Tamilnadu-641044, India, Tel: +(91)9842217268/+(91)4224500138; Fax: +(91)422-2240521; E-mail: sarvesh_59@yahoo.co.in
Citation: Sarveswaran V, Kumar S, Kumar R, Kumar A, Vamseedharan M. Spontaneous Perinephric Haemorrhage (Wunderlich Syndrome) Secondary to Upper Pole Renal Angiomyolipoma: A Rare Life Threatening Situation. J Clin Med Case Reports. 2015;2(1): 3.
Copyright © 2015 Sarveswaran et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN 2332-4120 | Volume: 2, Issue: 1
Submission: 09 January 2015 | Accepted: 23 January 2015 | Published: 28 January 2015
Reviewed & Approved by: Dr. Xu Zeng, Associate Professor, Department of Pathology and Laboratory Medicine, Temple University, USA
Abstract
Wunderlich Syndrome is a rare condition in which spontaneous renal haemorrhage occurs into the subcapsular and perirenal spaces in absence of trauma. It can present as a life threatening situation with profound shock which demands urgent attention. Though angiomyolipoma of the kidney is the most common neoplasm associated with spontaneous renal haemorrhage, varied presentation and lack of suspicion often pose a challenge when arriving at the diagnosis. The key in management of a case of Wunderlich Syndrome is high index of suspicion, prompt resuscitative measures, focussed investigations, identifying the underlying cause, embolisation and/or surgery. However, diagnostic difficulties often lead to faultydiagnosisand under reporting of the Wunderlich Syndrome.Keywords
Angiomyolipoma; Spontaneous renal haemorrhage; Wunderlich SyndromeIntroduction
Wunderlich Syndrome is a rare entity in which spontaneous renal haemorrhage occurs into the sub capsular and perirenal spaces in absence of trauma [1]. It can present with profound shock leading to a life threatening situation which needs urgent attention. Though various aetiologies have been associated with this condition, angiomyolipoma of the kidney is the most common neoplasm associated with spontaneous renal haemorrhage [2]. Its rarity and nonspecific presentation often pose a challenge when arriving at the diagnosis. However, high index of suspicion is essential in patients presenting with lumbar region pain to rule out such a catastrophe [3]. Knowledge of the underlying cause, swift arrival at the diagnosis and initiation of the treatment still holds the key in managing a case of Wunderlich Syndrome. We describe here a case of Wunderlich Syndrome secondary to upper pole renal angiomyolipoma presenting as a rare life threatening situation.Case Report
A 67 year old gentle man, a known hypertensive on tablet amlodipine (5 mg/day) for last 2 years reported to our emergency department with complaints of left sided abdominal discomfort accompanied by nausea and vomiting. He described a history of severe, constant left sided abdominal pain which had a sudden onset 6 hours back and has progressively worsened since then. There had been no specific precipitating factors or history of trauma. On examination, patient was in discomfort with a blood pressure of 120/70 mmhg and a heart rate of 90 per minute. The pain was more localised to the left lumbar region and a vague mass was palpable over the left side of his abdomen. His bowel sounds were normal and there was no peritonism. He had leucocytosis (15,600 cells/cu.mm) with neutrophillia (9,360 cells/cu.mm), haemoglobin of 9 g/dl, haematocrit of 27% and normal serum urea and creatinine levels. Urine routine examination was unremarkable.Abdominal radiography showed distended faecal loaded colon with loss of left psoas shadow. Before the patient could undergo further radiological evaluation, patient developed sudden hypotension (blood pressure of 80/40 mmhg), tachycardia (130 per minute), feeble peripheral pulses and cold peripheries. Infusion of crystalloids corrected his hypotension. Meanwhile, a bedside ultrasonography revealed a large solid mass in left hypochondrium and lumbar region (16x12 cm) showing mixed echogenicity. Left kidney could not be visualised and other solid organs appeared normal. Minimal fluid collection was also noted in the left perinephric region Later after stabilising the patient, a computed tomography of abdomen was done which showed a large left retroperitoneal hematoma (17x14x12 cm) pushing the left kidney anteriorly andsuperiorly (Figure 1). A fat dense lesion was also seen arising from the superior pole of left kidney (5x4x2 cm). There was no active extravasation of contrast during the study. Late phases of study also indicated good excretory functions of both kidneys.
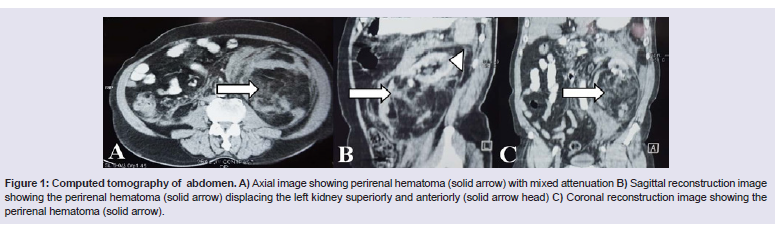
Figure 1: Computed tomography of abdomen. A) xial image showing perirenal hematoma (solid arrow) with mixed ttenuation B) Sagittal reconstruction image showing the perirenal ematoma (solid arrow) displacing the left kidney superiorly and nteriorly (solid arrow head) C) Coronal reconstruction image howing the perirenal hematoma (solid arrow).

Figure 2: Intraoperative photographs. A) Showing he large left renal mass (solid white arrow) B) Showing the erirenal hematoma (solid black arrow) C) Showing the post ephrectomy bed - psoas muscle (solid black arrow head) and bdominal aorta (solid white arrow head).
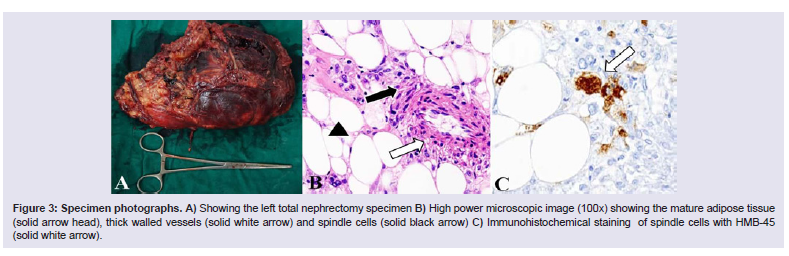
Figure 3: Specimen photographs. A) Showing the eft total nephrectomy specimen B) High power microscopic image 100x) showing the mature adipose tissue (solid arrow head), thick alled vessels (solid white arrow) and spindle cells (solid black rrow) C) Immunohistochemical staining of spindle cells with HMB- 45 (solid white arrow.
Discussion
Wunderlich Syndrome or spontaneous haemorrhage fromkidney was first observed by Bonet in 1700 and first clinically described as ‘spontaneous renal capsule apoplexy’ by Carl Reinhold August Wunderlich in 1856 [1]. The term Wunderlich Syndrome was first used by Coenen in 1910 [4]. This is a rare clinical phenomenon with only about 250 such cases reported since 2003 [5]. It is depicted as spontaneous bleeding of kidney into perirenal and sub capsular spaces sans trauma.Renal neoplasm’s accounts for 60-65% of spontaneous renal haemorrhage, the angiomyolipoma being the most common benign neoplasm [3]. It is also frequently found in association with hypertension [4]. Classically, Wunderlich Syndrome is described by the presence of Lenk’s triad which constitutes acute flank/lumbar pain, palpable tender mass and features of active internal bleed like hypotension, tachycardia and anaemia [7]. Clinically however, this triad is rarely seen and commonly presents with abdominal pain (67%), haematuria (40%) and hypovolemic shock (26.5%) [4]. The other common symptoms being nausea, vomiting, low grade fever and anaemia [8]. In contrary to hypovolemic shock, compression of the kidney by the hematoma may result in ischemia leading to renin release and hypertension [9].
Spontaneous renal haemorrhage is often detected by imaging while searching for other causes of lumbar pain and hypotension. Ultrasonography being quick and inexpensive is generally accepted first choice of investigation [7]. A Computed Tomography is considered the gold standard in establishing the diagnosis and often elucidates the underlying etiology attributing to this condition [6]. Also, Computed Tomography can identify active bleed in the form of contrast leak, Angiogram may be considered in cases of contrast leak in identifying the malefactor vessel [1]. However, the role of Computed Tomography is limited in hemodynamically unstable patients and may overlook a small neoplasm [10]. Magnetic Resonance Imaging is a valuable alternative if other radiological investigations are equivocal [6].
In treating Wunderlich Syndrome, achieving hemodynamic stability is of foremost importance. In the pursuit of achieving this, endovascular and/or surgical interventions play a major role.Although, Trans arterial embolisation has emerged as initial choice of treatment in spontaneous renal haemorrhage [11] conventional exploratory surgery holds its domain especially in patients with unidentified source of haemorrhage after radiological evaluation [12]. Diagnostic laparoscopy also has a role to play in establishing the diagnosis when clear diagnosis cannot be reached. There have been several literatures which propose robotic assisted laparoscopicnephrectomy as an alternate to conventional surgery [13]. Some surgeons even recommend an early surgery with possible nephrectomy if needed, as delayed surgery often results in more difficult resection due to adhesions [12]. However, there are no solid evidence based guidelines to favour either approaches as a choice of initial treatment [11]. Preoperative contralateral renal status assessment is a necessity in all cases as one may land up doing total nephrectomy due to unforeseen circumstances as it was in our case. Patients, who have been treated conservatively, needs follow up at three months intervals so as to know the status of the haematoma [8]. One must also be ready to face a malignancy which may have been missed in the initial radiological investigations especially, the renal cell carcinoma being the most common malignant neoplasm [6].
In conclusion, cornerstones in management of a case of Wunderlich Syndrome includes high index of suspicion, prompt resuscitative measures, focussed investigations, identifying the underlying cause, embolisation and/or surgery. Still, the choice and timing of the treatment modality needs to be tailored based on the resources available and should be individualised to achieve optimum results. In order to obtain better insight into this rare condition all diagnosed cases however trivial should be published. The low incidence of Wunderlich Syndrome could be attributed to the varied presentation, lack of suspicion and moreover the diagnostic difficulties encountered. All these factors contribute to faulty diagnosis and under reporting of the Wunderlich Syndrome
References
- Albi G, del Campo L, Tagarro D (2002) Wünderlich's Syndrome: causes, diagnosis and radiological management. Clin Radiol 57: 840-845.
- Vaddi SP, Reddy VP, Devraj R (2011) Wunderlich's Syndrome in a tuberous sclerosis patient. Indian J Surg 73: 227-229.
- Medda M, Picozzi SC, Bozzini G, Carmignani L (2009) Wunderlich′s Syndrome and hemorrhagic shock. J Emerg Trauma Shock 2: 203-205.
- 4. Daliakopoulos S (2011) Spontaneous retroperitoneal hematoma: A rare devastating clinical entity of a pleiada of less common origins. J Surg Tech Case Rep 3: 8-9.
- Blakeley CJ, Thiagalingham N (2003) Spontaneous retroperitoneal haemorrhage from a renal cyst: an unusual cause of haemorrhagic shock. Emerg Med J 20: 388.
- Katabathina VS, Katre R, Prasad SR, Surabhi VR, Shanbhogue AK, et al. (2011) Wunderlich Syndrome: cross-sectional imaging review. J Comput Assist Tomogr 35: 425-433.
- Ayhan Ö, Mansura D, Muratb O (2012) Subcapsular Renal Hematoma: Three Case Reports and Literature Reviews. Emerg Med 02.
- Baishya RK, Dhawan DR, Sabnis RB, Desai MR (2011) Spontaneous subcapsular renal hematoma: A case report and review of literature. Urol Ann 3: 44-46.
- Calvo-Romero JM, Ramos-Salado JL (2003) Spontaneous renal hematoma (Wunderlich Syndrome) associated with severe hypertension. J Clin Hypertens 5: 76-77.
- Lin CY, Lin YH, Wu FZ, Pan HB (2011) Wunderlich's Syndrome in spontaneous angiomyolipoma bleeding. Clin Kidney J 4: 211-212.
- Zhu Jain V, Ganpule A, Vyas, J, Muthu V, Sabnis RB, et al. (2009) Management of non-neoplastic renal hemorrhage by transarterial embolization. Urology 74: 522-52.
- Hao LW, Lin CM, Tsai SH (2008) Spontaneous hemorrhagic angiomyolipoma present with massive hematuria leading to urgent nephrectomy. Am J Emerg Med 26: 249.
- Ploumidis A, Katafigiotis I, Thanou M, Bodozoglou N, Athanasiou L, et al. (2013) Spontaneous retroperitoneal hemorrhage (Wunderlich Syndrome) due to large upper pole renal angiomyolipoma: does robotic-assisted laparoscopic partial nephrectomy have a role in primary treatment? Case Rep Urol: 498694.