
Journal of Clinical and Investigative Dermatology
Download PDF
 Figure 1:Solitary dome-shaped pink papule over the forehead.
Figure 1:Solitary dome-shaped pink papule over the forehead.
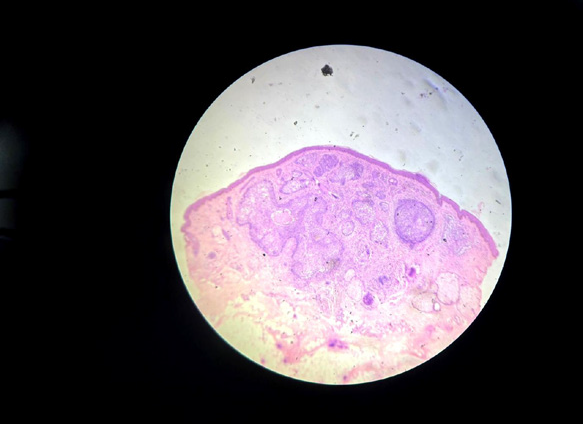 Figure 2:Low-power view showing well-circumscribed dermal tumor nests
(H&E).
Figure 2:Low-power view showing well-circumscribed dermal tumor nests
(H&E).
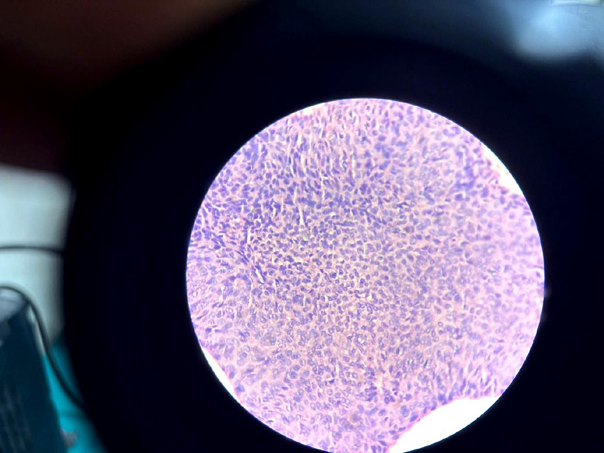 Figure 3:Basaloid nests with peripheral palisading (H&E).
Figure 3:Basaloid nests with peripheral palisading (H&E).
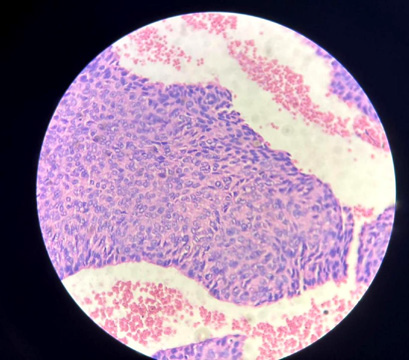 Figure 4:Central pale epithelial cells with vesicular nuclei (H&E).
Figure 4:Central pale epithelial cells with vesicular nuclei (H&E).
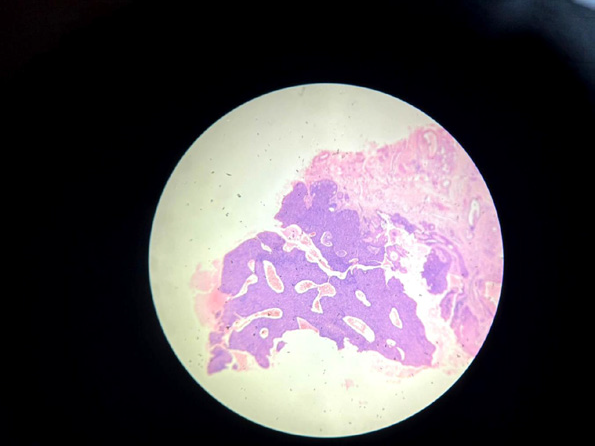 Figure 5:Dense lymphocytic infiltrate within tumor islands (H&E).
Figure 5:Dense lymphocytic infiltrate within tumor islands (H&E).
Case Report
Cutaneous Lymphadenoma Presenting as a Solitary Forehead Papule: A Clinicopathological Correlation
Bhattacharya S and Bhattacharyya AK
1Department of Dermatology, Venereology and Leprosy Prafulla Chandra
Sen Government Medical College and Hospital Aram bag, West Bengal,
India.
2Senior consultant, Divisional Railway Hospital Howrah, West Bengal,India.
2Senior consultant, Divisional Railway Hospital Howrah, West Bengal,India.
*Address for Correspondence:Dr. Shatanik Bhattacharya, Department of Dermatology, Venereology and Leprosy Prafulla Chandra Sen Government Medical College and Hospital Aram bag, West Bengal, India. E-mail Id: shatanik.bhattacharya.97@gmail.com
Submission: 16 April, 2026
Accepted: 27 May, 2026
Published: 30 May, 2026
Copyright: © 2026 Bhattacharya S, et al. This is an open access
article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Keywords:Cutaneous Lymphadenoma; Trichoblastoma Variant;
Adnexal Tumor; Forehead Papule; Basaloid Nests
Abstract
Cutaneous lymphadenoma represents an uncommon follicular
adnexal neoplasm characterized histologically by epithelial lobules
associated with dense lymphocytic infiltrates. We describe a young
woman with a solitary forehead papule whose biopsy demonstrated
basaloid epithelial islands admixed with prominent intratumoral
lymphocytes, leading to the diagnosis. Complete excision resulted
in an excellent outcome with no recurrence. Awareness of this rare
entity is essential to differentiate it from basal cell carcinoma and other
adnexal tumors.
Introduction
Cutaneous lymphadenoma, currently regarded within the
spectrum of trichoblastoma, is an exceptionally uncommon adnexal
neoplasm. It usually affects the head and neck region and may
clinically mimic basal cell carcinoma because of its pearly papular
appearance. Histologically, the lesion is composed of epithelial nests
embedded within a lymphocyte-rich stroma.
Cutaneous lymphadenoma- or Adamantinoid Trichoblastoma
was first described by Santa Cruz and Barr in 1987 as “lymphoepithelial
tumor of skin” which was later renamed as cutaneous lymphadenoma
in 1991.The lesions are seen mainly in the head and neck and present
as nonspecific papules and nodules.usually occurs in young adults.
Both sexes are equally affected.It is a rare benign adnexal tumor with
follicular, sebaceous or ductal differentiation therefore regarded as a
variant of Trichoblastoma,a neoplasm with folliculosebaceous and
apocrine germ differentiation.The tumor consists of nests and lobules
of basaloid cells in the reticular dermis with no epidermal connection.
The aggregates of cells are embedded in fibrous stroma. Tumor cells
are bland and display peripheral palisading. Presence of prominent
infiltration by T lymphocytes noted in the centre of tumor lobules and
nests. Focal areas of keratinisation are seen in some cases. No cellular
atypia seen and mitotic figures are rare. The pattern of cytokeratin 17
expression is patchy and peripheral in cutaneous lymphadenoma as
opposed to diffuse expression in Basal cell Merkel cells may be found
in cutaneous lymphadenoma, CEA and EMA expression may be seen.
Less than 50 cases have been reported in the world literature
Case Report
A 24-year-old lady presented with a firm nodular slowly
progressive swelling in the forehead for last 1 year duration.
Punch biopsy specimen of 4 mm was taken from the lesion over
the forehead. Section showed unremarkable epidermis. Dermis
shows nests of basaloid cells with peripheral palisading of basaloid
cells. These enclose larger epithelial cells with eosinophilic cytoplasm,
vesicular nuclei and prominent Many lymphocytes are admixed with
these large epithelial cells . Hair follicular differentiation is noted in
one focus. lymphocytic infiltrate is seen in the stroma. No evidence of
malignancy seen. Reed Sternberg like cells also seen
Cutaneous lymphadenoma is a rare benign adnexal neoplasm
that poses a significant diagnostic challenge because of its close
resemblance to basal cell carcinoma (BCC) and other follicular
tumors. In the present case, the lesion clinically presented as a small,
dome-shaped, pink papule over the forehead without ulceration or
telangiectasia, leading to consideration of benign adnexal tumors,
intradermal nevus, and BCC in the differential diagnosis.
Histopathological examination was decisive in establishing the diagnosis. Microscopy demonstrated sharply demarcated epithelial lobules situated within the dermis. The lobules were composed predominantly of basaloid cells arranged along the periphery, enclosing larger pale-staining epithelial cells amid dense lymphocytic infiltrates.
Histopathological examination was decisive in establishing the diagnosis. Microscopy demonstrated sharply demarcated epithelial lobules situated within the dermis. The lobules were composed predominantly of basaloid cells arranged along the periphery, enclosing larger pale-staining epithelial cells amid dense lymphocytic infiltrates.
Trichoblastoma was another important differential diagnosis
because of the follicular germinative differentiation seen in both
entities. However, trichoblastoma typically lacks the prominent
intraepithelial lymphocytic infiltrate characteristic of cutaneous
lymphadenoma. Likewise, lymphoepithelioma-like carcinoma of
the skin was excluded due to the absence of cellular atypia, invasive
growth pattern, and malignant cytological features.
The intimate admixture of reactive lymphocytes within epithelial
tumor islands is considered a hallmark of cutaneous lymphadenoma
and remains the most useful diagnostic clue distinguishing it from
other basaloid adnexal neoplasms.
Diagnosis- Nodular Adamantinoid Trichoblastoma
Cutaneous lymphadenoma (variant of trichoblastoma).
Diagnosis- Nodular Adamantinoid Trichoblastoma
Cutaneous lymphadenoma (variant of trichoblastoma).
Differential diagnosis:
Basal cell carcinoma was considered an important differential
diagnosis because both lesions may present as solitary pearly papules
over sun-exposed facial skin. However, the absence of stromal
retraction clefts, mucinous stromal alteration, significant cytological
atypia, and increased mitotic activity argued against basal cell
carcinoma in the present case.
Trichoblastoma was another close histological mimic due to the presence of basaloid follicular germinative cells. Nevertheless, conventional trichoblastoma generally lacks the dense intratumoral lymphocytic infiltrate that represents a defining feature of cutaneous lymphadenoma.
Trichoblastoma was another close histological mimic due to the presence of basaloid follicular germinative cells. Nevertheless, conventional trichoblastoma generally lacks the dense intratumoral lymphocytic infiltrate that represents a defining feature of cutaneous lymphadenoma.
Lymphoepithelioma-like carcinoma of the skin was also excluded
because the present lesion did not demonstrate infiltrative growth,
marked nuclear pleomorphism, or overt malignant cytological
features.
Clear cell syringoma may occasionally enter the differential diagnosis because of the presence of epithelial nests; however, ductal eccrine differentiation and characteristic tadpole-shaped structures were absent in our specimen.
Pilomatricoma was ruled out due to the lack of matrical differentiation, ghost cells, and calcification. Similarly, dermatofibroma was excluded because the lesion lacked a fibrohistiocytic proliferation and instead showed distinct epithelial lobules with peripheral basaloid arrangement.
Overall, the combination of epithelial islands, prominent lymphocytic infiltrates, follicular differentiation, and bland cytology strongly favored a diagnosis of cutaneous lymphadenoma. Basal cell carcinoma – present usually in sun exposed area, usually single, painless pearly or waxy papule or nodule often with central ulceration. (Rodent ulcer)
Presence of telangiectasia, often bleeding or crusting
Clear cell syringoma may occasionally enter the differential diagnosis because of the presence of epithelial nests; however, ductal eccrine differentiation and characteristic tadpole-shaped structures were absent in our specimen.
Pilomatricoma was ruled out due to the lack of matrical differentiation, ghost cells, and calcification. Similarly, dermatofibroma was excluded because the lesion lacked a fibrohistiocytic proliferation and instead showed distinct epithelial lobules with peripheral basaloid arrangement.
Overall, the combination of epithelial islands, prominent lymphocytic infiltrates, follicular differentiation, and bland cytology strongly favored a diagnosis of cutaneous lymphadenoma. Basal cell carcinoma – present usually in sun exposed area, usually single, painless pearly or waxy papule or nodule often with central ulceration. (Rodent ulcer)
Presence of telangiectasia, often bleeding or crusting
Presence of retraction artefact, fibromyxoid stroma, peripheral
palisading with atypia.
Intradermal naevus- papules or macules tan brown uniformly pigmented and small (less than 0.6 cm), usually adjacent to hair follicle. Often erosion and ulcerations are present.
Presence of naevus cell aggregates in the dermis. Abundant eosinophilic to amphophilic cytoplasm containing coarse melanin granules.
Clear cell syringoma – Multiple small (1-4 mm) firm flesh coloured lesion typically bilaterally symmetrical Common in female(eyelid). Pruritus exacerbates during summer months and menstruation. Presence of tadpole-like structures of eccrine differentiation, absence of intratubular lymphocytic infiltrate.
Lymphoepithelial tumor of skin-This is a malignant tumor that also features basaloid nests with prominent lymphocytic infiltration (lymphotropic). However, LELC shows more cellular atypia and higher mitotic figures compared to the bland cytology of AT.
Intradermal naevus- papules or macules tan brown uniformly pigmented and small (less than 0.6 cm), usually adjacent to hair follicle. Often erosion and ulcerations are present.
Presence of naevus cell aggregates in the dermis. Abundant eosinophilic to amphophilic cytoplasm containing coarse melanin granules.
Clear cell syringoma – Multiple small (1-4 mm) firm flesh coloured lesion typically bilaterally symmetrical Common in female(eyelid). Pruritus exacerbates during summer months and menstruation. Presence of tadpole-like structures of eccrine differentiation, absence of intratubular lymphocytic infiltrate.
Lymphoepithelial tumor of skin-This is a malignant tumor that also features basaloid nests with prominent lymphocytic infiltration (lymphotropic). However, LELC shows more cellular atypia and higher mitotic figures compared to the bland cytology of AT.
Trichoblastic carcinoma -Malignant, highly infiltrative
counterpart that shows much greater cytologic atypia than the benign
AT.
Pilomatricoma -Hair matrix tumor that can also contain basaloid
cells, but it usually shows distinct ghost cell keratinization
Dermatofibroma: A superficial dermal tumor that can be excluded by its characteristic fibrotic histology and lack of distinct basaloid nests.
The patient underwent complete surgical excision of the lesion. The postoperative period was uneventful, with satisfactory cosmetic healing. No evidence of local recurrence or development of new lesions was observed during follow up.
Dermatofibroma: A superficial dermal tumor that can be excluded by its characteristic fibrotic histology and lack of distinct basaloid nests.
The patient underwent complete surgical excision of the lesion. The postoperative period was uneventful, with satisfactory cosmetic healing. No evidence of local recurrence or development of new lesions was observed during follow up.
Discussion
Adamantinoid Trichoblastoma/ Cutaneous lymphadenoma is a
rare benign adnexal tumor commonly presenting as asymptomatic
dome shaped, flesh coloured papule or nodule in the head and They
are commonly seen in young to middle aged patients with male
dominance.Due to the rarity of Adamantinoid Trichoblastoma,it is
often misinterpreted as Basal cell carcinoma, adnexal tumor, naevus
or dermatofibroma.The present case was clinically thought to be
intradermal naevus.[2]
Microscopic examination revealed a triphasic tumor with cell nests with peripheral palisading of basaloid cells (epithelial component), lymphoid infiltration and desmoplastic stroma (mesenchymal components). There can be large Reed Sternberg like cells within the lobules.Focal ductal, follicular and sebaceous differentiation and central keratinisation and stromal mucinosis have been documented [3]. The tumor is well circumscribed and unencapsulated, but presence of infiltrating outlines makes tumor recurrence possible.[2]
The Histological differential diagnosis includes clear cell Basal cell carcinoma, clear cell syringoma, trichoepithelioma and malignant lymphoepithelioma like carcinoma. In younger patients, it has to be differentiated from dermal thymus, which is an Aberrant location of thymic tissue in the skin due to defective migration and present as linear symmetric ulcerated scar Like lesions in the neck in patients with other facial branchial anomalies.[2]
Several proposals regarding the possible histogenesis of the tumour have been reported. Santa cruz Barr told it to be immature pilosebaceous differentiation. [5,6]
Others suggested eccrine or lynphotropic solid syringoma, lynphotropic eccrine benign tumors.[7,8].Dahil and Seywright reported synchronous occurrence of cutaneous lymphadenoma and eccrine syringoid carcinoma in a single person providing additional evidence in support of eccrine differentiation.Filipo et al [10] argued that cutaneous lymphadenoma/ Adamantinoid Trichoblastoma is a distinct entity that may mimic Basal cell carcinoma with pilar or eccrine differentiation.Mc Niff et al [11] evaluated the immunohistochemical staining pattern of CK 20 Merkel cells,,BCL2 epithelial cells,S100 & CD1a( langerhans cell),CD34( stromal cells) in cutaneous lymphadenoma., Trichoblastoma and nodular Basal cell carcinoma.They observed similar staining pattern of first three markers in cutaneous lymphadenoma and Trichoblastoma ( importantly peripheral staining of BCL2 in tumor lobules) and were of the opinion that cutaneous lymphadenoma is a variant of Trichoblastoma.Most recently these tumors have been classified as Adamantinoid Trichoblastoma considering its resemblance to dental Adamantinomas.( Epithelial and mesenchymal tumor of oral cavity). [2,12,13].
The marked lymphocytic infiltrate in these tumors is thought to be due to defective lymphocytes – epithelial interaction or exuberant host response to tumour cells. [14,15]
A benign clinical course has been reported in the literature. Complete surgical excision is the definitive treatment of choice.To conclude
Adamantinoid Trichoblastoma is a benign adnexal tumor that clinically masquerade as a variety of benign and malignant Due to the presence of infiltrating lymphocytes within tumor lobules, we feel that “Lymphotropic Adamantinoma” would be the appropriate terminology to describe this rare entity.
Cutaneous lymphadenoma remains an exceptionally uncommon adnexal tumor, with relatively few cases documented in literature. Most reported cases occur in middle-aged or elderly individuals and predominantly involve the head and neck region, especially the cheek, forehead, eyelids, and nose. The present case is noteworthy because the lesion occurred in a young 24-year-old female, which is relatively uncommon for this entity.
Microscopic examination revealed a triphasic tumor with cell nests with peripheral palisading of basaloid cells (epithelial component), lymphoid infiltration and desmoplastic stroma (mesenchymal components). There can be large Reed Sternberg like cells within the lobules.Focal ductal, follicular and sebaceous differentiation and central keratinisation and stromal mucinosis have been documented [3]. The tumor is well circumscribed and unencapsulated, but presence of infiltrating outlines makes tumor recurrence possible.[2]
The Histological differential diagnosis includes clear cell Basal cell carcinoma, clear cell syringoma, trichoepithelioma and malignant lymphoepithelioma like carcinoma. In younger patients, it has to be differentiated from dermal thymus, which is an Aberrant location of thymic tissue in the skin due to defective migration and present as linear symmetric ulcerated scar Like lesions in the neck in patients with other facial branchial anomalies.[2]
Several proposals regarding the possible histogenesis of the tumour have been reported. Santa cruz Barr told it to be immature pilosebaceous differentiation. [5,6]
Others suggested eccrine or lynphotropic solid syringoma, lynphotropic eccrine benign tumors.[7,8].Dahil and Seywright reported synchronous occurrence of cutaneous lymphadenoma and eccrine syringoid carcinoma in a single person providing additional evidence in support of eccrine differentiation.Filipo et al [10] argued that cutaneous lymphadenoma/ Adamantinoid Trichoblastoma is a distinct entity that may mimic Basal cell carcinoma with pilar or eccrine differentiation.Mc Niff et al [11] evaluated the immunohistochemical staining pattern of CK 20 Merkel cells,,BCL2 epithelial cells,S100 & CD1a( langerhans cell),CD34( stromal cells) in cutaneous lymphadenoma., Trichoblastoma and nodular Basal cell carcinoma.They observed similar staining pattern of first three markers in cutaneous lymphadenoma and Trichoblastoma ( importantly peripheral staining of BCL2 in tumor lobules) and were of the opinion that cutaneous lymphadenoma is a variant of Trichoblastoma.Most recently these tumors have been classified as Adamantinoid Trichoblastoma considering its resemblance to dental Adamantinomas.( Epithelial and mesenchymal tumor of oral cavity). [2,12,13].
The marked lymphocytic infiltrate in these tumors is thought to be due to defective lymphocytes – epithelial interaction or exuberant host response to tumour cells. [14,15]
A benign clinical course has been reported in the literature. Complete surgical excision is the definitive treatment of choice.To conclude
Adamantinoid Trichoblastoma is a benign adnexal tumor that clinically masquerade as a variety of benign and malignant Due to the presence of infiltrating lymphocytes within tumor lobules, we feel that “Lymphotropic Adamantinoma” would be the appropriate terminology to describe this rare entity.
Cutaneous lymphadenoma remains an exceptionally uncommon adnexal tumor, with relatively few cases documented in literature. Most reported cases occur in middle-aged or elderly individuals and predominantly involve the head and neck region, especially the cheek, forehead, eyelids, and nose. The present case is noteworthy because the lesion occurred in a young 24-year-old female, which is relatively uncommon for this entity.
The tumor is currently regarded as a variant of trichoblastoma
with follicular germinative differentiation. Some authors propose
derivation from hair follicle stem cells because of its morphological
overlap with follicular adnexal tumors. Despite its benign nature,
cutaneous lymphadenoma continues to be clinically important
because it is frequently mistaken for BCC, both clinically and
histologically.
Recent dermatopathology literature emphasizes the importance of careful recognition of its characteristic lymphocyte-rich epithelial islands and the absence of stromal retraction artifact. Misdiagnosis as BCC may lead to unnecessarily wide excision or aggressive management, particularly when lesions occur on cosmetically sensitive facial sites.
Immunohistochemistry may occasionally assist in diagnostically difficult cases. Cytokeratin positivity confirms epithelial differentiation, while CD3 and CD20 highlight the reactive T- and B-lymphocytic infiltrate. BerEP4 positivity may overlap with BCC and therefore should be interpreted cautiously in conjunction with morphology.
Overall prognosis is excellent following complete surgical excision, and recurrence is extremely uncommon. No definite malignant transformation has been convincingly established in the literature to date.
Skin coloured semicircular nodule with telangiectasia, absence of ulceration or crusting
Although dermoscopy was not formally documented in the present case, previously reported dermoscopic features of cutaneous lymphadenoma include pink-white structureless areas, fine arborizing vessels, and homogeneous erythematous background. These findings may overlap with basal cell carcinoma, further emphasizing the importance of histopathological confirmation.
Recent dermatopathology literature emphasizes the importance of careful recognition of its characteristic lymphocyte-rich epithelial islands and the absence of stromal retraction artifact. Misdiagnosis as BCC may lead to unnecessarily wide excision or aggressive management, particularly when lesions occur on cosmetically sensitive facial sites.
Immunohistochemistry may occasionally assist in diagnostically difficult cases. Cytokeratin positivity confirms epithelial differentiation, while CD3 and CD20 highlight the reactive T- and B-lymphocytic infiltrate. BerEP4 positivity may overlap with BCC and therefore should be interpreted cautiously in conjunction with morphology.
Overall prognosis is excellent following complete surgical excision, and recurrence is extremely uncommon. No definite malignant transformation has been convincingly established in the literature to date.
Skin coloured semicircular nodule with telangiectasia, absence of ulceration or crusting
Although dermoscopy was not formally documented in the present case, previously reported dermoscopic features of cutaneous lymphadenoma include pink-white structureless areas, fine arborizing vessels, and homogeneous erythematous background. These findings may overlap with basal cell carcinoma, further emphasizing the importance of histopathological confirmation.
Cutaneous lymphadenoma is an uncommon benign adnexal
neoplasm currently regarded within the spectrum of follicular
tumors, particularly trichoblastoma. Owing to its rarity and
nonspecific clinical appearance, the lesion is frequently mistaken for
more common cutaneous neoplasms, especially basal cell carcinoma.
Most reported lesions arise on the head and neck region as slowly
enlarging asymptomatic papules or nodules.
The present case is notable because the lesion occurred in a young adult female and clinically simulated a benign papular lesion of the forehead. Histopathological examination was essential for establishing the diagnosis. The biopsy demonstrated sharply circumscribed dermal epithelial lobules composed of peripheral basaloid cells surrounding larger pale epithelial cells within a dense lymphocyte-rich stroma. Importantly, there was no evidence of stromal retraction, necrosis, significant atypia, or brisk mitotic activity.
The characteristic admixture of epithelial nests and abundant reactive lymphocytes remains the most valuable diagnostic clue in distinguishing cutaneous lymphadenoma from other basaloid adnexal tumors. Some lesions may additionally demonstrate follicular or sebaceous differentiation. Occasional Reed–Sternberg-like cells and focal keratinization have also been described in previous reports.
The present case is notable because the lesion occurred in a young adult female and clinically simulated a benign papular lesion of the forehead. Histopathological examination was essential for establishing the diagnosis. The biopsy demonstrated sharply circumscribed dermal epithelial lobules composed of peripheral basaloid cells surrounding larger pale epithelial cells within a dense lymphocyte-rich stroma. Importantly, there was no evidence of stromal retraction, necrosis, significant atypia, or brisk mitotic activity.
The characteristic admixture of epithelial nests and abundant reactive lymphocytes remains the most valuable diagnostic clue in distinguishing cutaneous lymphadenoma from other basaloid adnexal tumors. Some lesions may additionally demonstrate follicular or sebaceous differentiation. Occasional Reed–Sternberg-like cells and focal keratinization have also been described in previous reports.
Although the exact histogenesis remains uncertain, most
authors support follicular germinative differentiation because of the
morphological overlap with trichoblastoma. Immunohistochemical
studies described in the literature have demonstrated expression
patterns supporting epithelial differentiation along with reactive Tand
B-lymphocytic infiltrates. However, routine histopathology is
usually sufficient for diagnosis in typical cases.
Recognition of this entity is clinically important because misinterpretation as basal cell carcinoma may lead to unnecessarily aggressive treatment. Complete surgical excision remains curative in the majority of cases, and recurrence is distinctly uncommon.
In conclusion, cutaneous lymphadenoma should be considered in the differential diagnosis of solitary facial papules showing basaloid epithelial nests with dense lymphoid infiltrates. Careful clinicopathological correlation is essential to avoid diagnostic pitfalls and overtreatment.
Recognition of this entity is clinically important because misinterpretation as basal cell carcinoma may lead to unnecessarily aggressive treatment. Complete surgical excision remains curative in the majority of cases, and recurrence is distinctly uncommon.
In conclusion, cutaneous lymphadenoma should be considered in the differential diagnosis of solitary facial papules showing basaloid epithelial nests with dense lymphoid infiltrates. Careful clinicopathological correlation is essential to avoid diagnostic pitfalls and overtreatment.
Conclusion
Awareness of this uncommon follicular adnexal neoplasm is
important because its clinicopathological resemblance to basal cell
carcinoma may result in diagnostic confusion and unnecessary
aggressive treatment.
Patient Consent:
Written informed consent was obtained from the patient for
publication of clinical images and data.
References
Citation
Bhattacharya S, Bhattacharyya AK. Cutaneous Lymphadenoma Presenting as a Solitary Forehead Papule: A Clinicopathological Correlation. J Clin Investigat Dermatol. 2026;14(1): 1