
Journal of Clinical and Investigative Dermatology
Download PDF
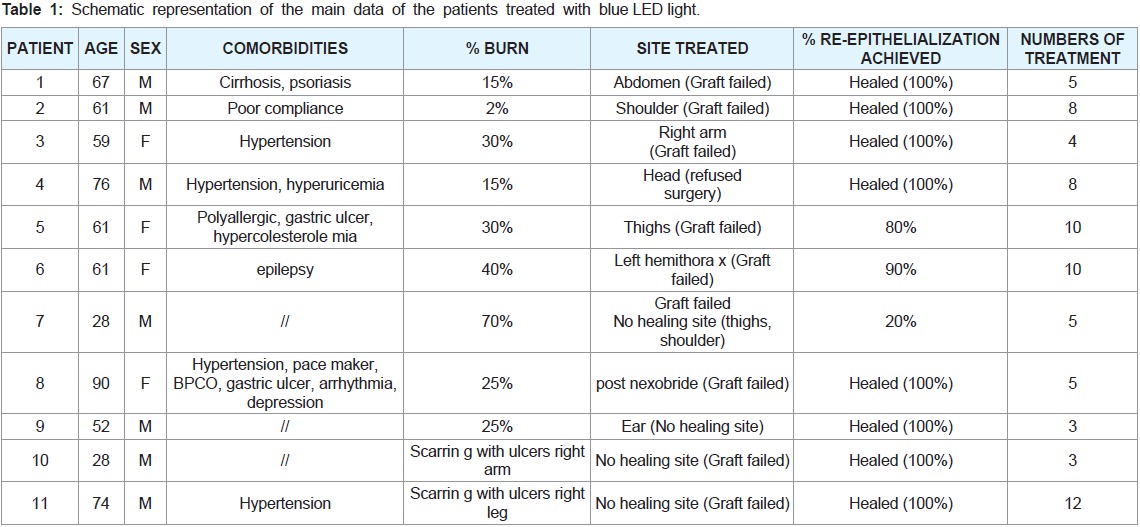 Table 1: Schematic representation of the main data of the patients treated with blue LED light.
Table 1: Schematic representation of the main data of the patients treated with blue LED light.
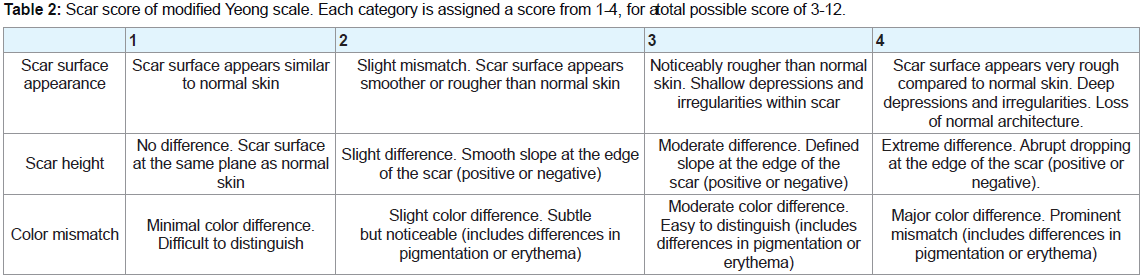 Table 2: Scar score of modified Yeong scale. Each category is assigned a score from 1-4, for a total possible score of 3-12.
Table 2: Scar score of modified Yeong scale. Each category is assigned a score from 1-4, for a total possible score of 3-12.
 Figure 1: Clinical case 1 treated with blue LED light. A,B: Deep burns of the
abdomen at the admission Burns after surgical treatment and the application
of autologous skin grafts then failed. C, C-1: Beginning of the Blue LED light
treatment. Magnification of the Blue LED light treatment on the lesion area.
D: Improvement of the wound bed after 3 treatments with a reduction of
lesion’s depth and inflammation, exudation and re-epithelialization. E: End of
treatment. F,G: Follow-up after 3 and 14 months.
Figure 1: Clinical case 1 treated with blue LED light. A,B: Deep burns of the
abdomen at the admission Burns after surgical treatment and the application
of autologous skin grafts then failed. C, C-1: Beginning of the Blue LED light
treatment. Magnification of the Blue LED light treatment on the lesion area.
D: Improvement of the wound bed after 3 treatments with a reduction of
lesion’s depth and inflammation, exudation and re-epithelialization. E: End of
treatment. F,G: Follow-up after 3 and 14 months.
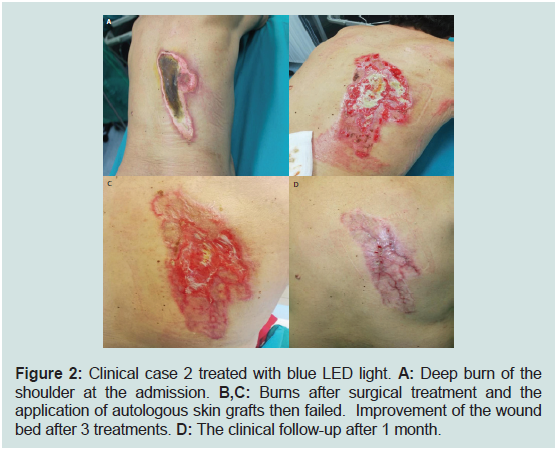 Figure 2: Clinical case 2 treated with blue LED light. A: Deep burn of the
shoulder at the admission. B,C: Burns after surgical treatment and the
application of autologous skin grafts then failed. Improvement of the wound
bed after 3 treatments. D: The clinical follow-up after 1 month.
Figure 2: Clinical case 2 treated with blue LED light. A: Deep burn of the
shoulder at the admission. B,C: Burns after surgical treatment and the
application of autologous skin grafts then failed. Improvement of the wound
bed after 3 treatments. D: The clinical follow-up after 1 month.
 Figure 3: Clinical case 3 treated with blue LED light. A: Deep burn of the
right upper limb at the admission. B: Burn of the right upper limb after surgical
treatment and the application of autologous skin grafts then failed. C: Burn of
the right upper limb after failed grafts treated with advanced dressings. D,E:
Spontaneous re-epithelialization of the wound after 2 and 4, treatments twice
a week. F,G: Clinical follow-up after 6 and 9 months. Aesthetic results of right
upper limb treated with blue LED light. H: Those of the lower limb with grafted
skin after surgery.
Figure 3: Clinical case 3 treated with blue LED light. A: Deep burn of the
right upper limb at the admission. B: Burn of the right upper limb after surgical
treatment and the application of autologous skin grafts then failed. C: Burn of
the right upper limb after failed grafts treated with advanced dressings. D,E:
Spontaneous re-epithelialization of the wound after 2 and 4, treatments twice
a week. F,G: Clinical follow-up after 6 and 9 months. Aesthetic results of right
upper limb treated with blue LED light. H: Those of the lower limb with grafted
skin after surgery.
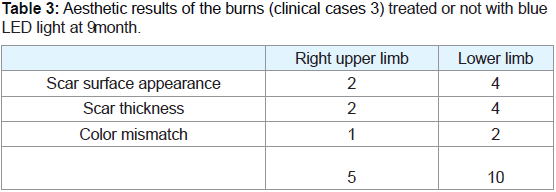 Table 3: Aesthetic results of the burns (clinical cases 3) treated or not with blue
LED light at 9 month.
Table 3: Aesthetic results of the burns (clinical cases 3) treated or not with blue
LED light at 9 month.
Case Report
Blue Led Light in Burns: A New Treatment’s Modality
Orlandi C, Purpura V* and Melandri D
Burns Centre, Dermatology and Emilia Romagna Regional Skin Bank, M.
Bufalini Hospital, Italy
*Address for Correspondence: Purpura V, Burns Centre, Dermatology and Emilia Romagna Regional Skin
Bank, M. Bufalini Hospital, Viale Ghirotti 286, 47522 Cesena (FC), Italy; Fax: 39
0547 394327; Tel: 39 0547 352919; Email: Valeria.Purpura@Auslromagna.It
Submission: 27 July, 2021;
Accepted: 30 August, 2021;
Published: 05 September, 2021
Copyright: © 2021 Orlandi C, et al. This is an open access article distributed
under the Creative Commons Attribution License, which permits unrestricted
use, distribution, and reproduction in any medium, provided the original work
is properly cited.
Abstract
The management of full-thickness severe burns is an important
issue from the medical point of view, especially when the autologous
skin is not able to engraft on the wound area and, in turn, to induce
its re-epithelialization. As a consequence, the wound healing process
occurs slowly, by second intention leading to an increased formation of
scar tissue. The delay in wound healing leads to a longer management
of the patient, increasing inconveniences and increasing the costs for
the health system. In addition, comorbidity factors of the patients such
as diabetes, infections or its elderly age can also affect the healing
process.
With the aim to improve the wound bed as well as the healing
time, we decided to test photobiomodulation therapy (PBMT) as a
new practice for the burn-care treatment. The results here reported
show its effectiveness in the promotion of wound healing leading to
faster and better final aesthetic results.
Keywords
Wounds; Healing process; Photobiomodulation therapy;
Hard to heal burns
Abbreviations
PBMT: Photobiomodulation Therapy
Introduction
Burns is a type of acute trauma affecting millions of people
worldwide that frequently occurs for an incidental/intentional
exposure to fire as well as wrong use of inflammable liquids [1].
The therapeutic strategy used to manage burned patients is related
to the severity, depth and anatomic area of the burn and the clinical
condition of the patient. In fact, a spontaneous re-epithelialization
of the wound area is expected up to a superficial/medium seconddegree
burn, while the removal of necrotic tissue and the replacement
of skin defect with autologous skin is performed on burns of deep
second/ third degree [2-4]. However, the engraftment of autologous
skin on the damaged area is not always guaranteed and its partial/
total detachment from lesion leads to a delayed healing process by
second intention further affected by patient’s comorbidities. Among
the different approaches developed to stimulate wound healing,
the use of PBMT appears to be very promising. The underlying
mechanism of this new therapy is a photothermal effect, due to
the selective absorption of the blue light by the hemoglobin - in
particular the heme group - in the bleeding wound able to improve
the healing process, with an apparent modulation of the fibroblast
activity and better recovery of the collagen content in the wound
area. The direct light energy transfer from the device to the patient
permits the interaction and the stimulation of some chromophores
of blood and skin, in particular cytochrome C and protoporphryn
IX. Once activated by the blue light, cytochrome C interacts with the
last two mitochondrial transport chain complexes and contributes
to strengthening the cellular respiratory process, increasing the
production of adenosine triphosphate, energy currency of the cell,
which can intensify its metabolic activity. A further important
effect is an increased production of reactive oxygen species (ROS), signal transducers of numerous cellular pathways in tissue repair;
an increased production of ROS induces a controlled increase of
inflammatory functions sufficient for stimulating tissue response
[5-7]. Although the mechanism underlying photobiomodulation is
still not completely understood, it has accumulated evidences of a
positive action on all phases of wound repair, from inflammation to
remodeling.
These beneficial effects include acceleration of wound healing,
cellular and extracellular matrix proliferation, collagen production
and granulation tissue formation [8]. It also shows anti-microbial
activity [9] leading to synergic, beneficial effects on healing process.
Important scientific literature supports the evidence that light
stimulates tissue regeneration and skin repair owing to its ability to
interact with tissue inducing the photobiomodulation [10]. Previous
studies show how PBMT is able to promote metabolism of all cellular
processes by ATP synthesis and, in turn, to stimulate angiogenesis
[11], tissue repair with reduction of scar tissue and formation of
keloids [12]. To date, the use of blue light with a low frequencies range
of 400-450 nm results to be effective for the treatment of different
dermatologic pathologies such as acne [13-15], psoriasis [16] and
eczema [17] as well as skin wounds [18-19]. For all these advantages,
the use of PBMT is now increasing in clinical practice to improve
wound bed as well as the healing time.
In this study, we evaluated for the first time the effectiveness of
this treatment both in burned patients not able for surgery for their
comorbidities and those in which skin engraftment failed, in order to
promote the healing process. Our results lead us to consider PBMT
an effective new burn- care approach available in the clinical practice
of burn-care.
Material and Methods
The observations were made on 11 patients (4 females and 7
males) with burns resistant to standard treatment then treated with
PBMT in order to promote the skin lesion healing. In particular, 9
patients showed deep burns of different etiologies not responding
to surgery with skin grafts while the other 2 patients showed skin
scarring treated with dermo-epidermal substitutes with incomplete
re-epithelialization.
To perform PBMT, we used a portable medical device emitting
blue light with a wavelength of between 400 to 430 nm; it was applied
for one minute/application at a distance of 4 cm from the wound
bed, providing it a LED radiation of 120 mW/cm2 power density,
which corresponds to an energy density dose of 7,2 J/cm2; light
covered a circular 5 cm diameter area so that application numbers
were correlated to wound size. The treatment schedule adopted
was the application of blue LED light for 60 seconds twice a week
for a maximum period of ten weeks at the time of dressing change
and after wound cleaning with distilled water. Following the blue
LED light treatment, appropriate dressing for the type of lesion was
applied according to the required standard. This treatment does not
interfere with other systemic therapies that may be in place and does
not involve any additional risk compared to standard treatment; the
comparative evaluation of aesthetic outcomes was performed using
modified Yeong scale (Table 2).
Results
In our study, we selected patients with burns resistant to standard
treatment candidates to alternative, not invasive approaches such as
PBMT. In particular, we mainly evaluated data of the patients treated
reported in Table 1. The treatment was well tolerated, there were no
reports of side effects or other adverse events and compliance was
excellent. The patients recorded a significant reduction in pain at the
end of the treatment period. We witnessed the reactivation of the
reparative process with the complete re-epithelialization of the burns
or of the burned area where the autologous graft was not successful
in 8 cases out of [11]. In 2 cases we observed a percentage reduction
of the lesion area of at least 80% compared to the initial one. In only
1 case there was a poor response to the treatment probably due to
the extreme severity of the initial picture and the consequent severe
physical deterioration of the patient.
We describe below three cases particularly interesting from a
clinical point of view, for the results obtained given the initial lesion
conditions.
Clinical case 1:
The first patient we treated with blue LED light was a 67 year old
man with cirrhosis and psoriasis. He presented deep burns of the
abdomen (Figure 1A) treated with surgery with the application of
autologous skin grafts then failed (Figure 1B). Thus, we decided to use
PBMT to promote the healing process. In this case, five applications
twice a week were required to obtain the wound healing, according
to the protocol described in material and methods (Figure 1C, detail
Figure 1 C-1).
Surprisingly, we observed a marked improvement of the wound
bed after only three treatments as well as a reduction of lesion’s depth
and inflammation, exudation and re-epithelialization (Figure 1D).
The wound bed at the end of the treatments showed a complete reepithelialization
with focal atrophic areas, without an inflammatory
response (Figure 1E) and the clinical follow-up after 3 and 14
months showed a scarcely erythematous and hypertrophic scarring,
not retracting and soft to the touch. The atrophic areas were also
significantly reduced (Figure 1F-G).
Clinical case 2:
The second patient was a 61 year old man with deep burn of
shoulder (Figure 2A) treated with surgery with the application of
autologous skin grafts then failed (Figure 2B). Although a new surgery
was recommended, the patient refuse it. Thus, we decided to use
PBMT to promote the healing process. In this case, eight applications
twice a week were required to obtain the wound healing. We quickly
observed a revitalization of the wound bed, with reduction of slough
and clean base, normal exudate and proliferative edges already after
3 treatments (Figure 2C) with a flat scarring, soft to the touch, pink
in color and with the presence of fine superficial telangiectasias in the
follow-up after 1 months (Figure 2D).
Clinical case 3:
The third patient was a 59 year old woman suffering from hypertension. She presented deep burns of the right upper and
lower limb (Figure 3A) treated with surgery with the application of
autologous skin grafts then failed only on the arm (Figure 3B). We
initially treated this area with advanced dressing (Figure 3C) but
given the slow response we decided to use the PBMT to promote the
healing.
In most clinical cases, we also noticed that the use of blue LED
light induced a modulation of fibroblast’s activity, so as to reduce the
possibility of the appearance of keloids or hypertrophic scars keloid
recurrence. Thus, in some cases we have also taken into account
the aesthetic results, identified as the scar surface appearance, scar
height and color mismatch of wounds after 6 and 12 - 14 months
after hospitalization/healing according to parameters of the modified
Yeong scale (Table 2). In particular, we could compare at 9 months
the aesthetic outcomes obtained in the clinical case 3 treated with
blue LED light on the right upper limb in which graft skin failed
(Figure 3F-G) and those of the lower limb (Figure 3H) in which the
engraftment of skin after surgery was evident (Table 3). Based on the
clinical evaluation and the score obtained using the modified Yeong
scale, we can conclude that the area treated with blue LED light has
had a more favorable evolution in terms of scar outcome (thickness,
discoloration and consistency of the tissue) than the area treated in a
standard way.
Discussion
Surgical procedure of autologous graft is performed as the standard of care (SOC) for burns; the coverage of a deep burn with
the graft may be immediate, delayed for a few days after the excision
or late, after a first phase of direct healing. However, the autologous
graft has a probability of failure with total or partial detachment of the
grafted skin. When it happens, the healing process of the lesion occurs
by secondary intention but it is not always easy to manage, as this
process can be delayed or stopped by many factors such as diabetes,
infections, metabolic deficiencies and the advanced age of the subject.
Although SOC appears to be effective in the most of clinical cases, it
results invasive, not selective for necrotic tissue and not always easily
practicable for clinical and organizational problems; moreover, the
critical conditions of the patients or the presence of comorbidities
can be real contraindications to surgical approach. For this reasons,
minimally or not invasive approaches have been considered as additional therapies able to reduce the possible side effects related to
surgery. In fact, a proper wound management and dressing of burn
instead of or after surgery is an important part of the healing process,
in order to prevent the onset of infections or other complications, and
also to accelerate the wound healing with as little scarring as possible.
Among the not invasive approaches used for the burns management,
photobiomodulation is a new therapy for treating hard to heal
wounds. To the best of our knowledge there are not trials or studies
that have analyzed photobiomodulation’s effects on burns so this is
the first case series. The benefits identified in our clinical cases can be
attributable not only to a reactivation of the tissue repair process but
also to a reduced healing time and an improvement in scarring, with
the consequent indirect benefits, namely reduction of public health
expenditure, improvement of quality of the life of patients with burn
scars that often significantly impact this parameter. According to
our small experience, the blue LED light used for PBMT contributed
significantly to a faster healing process, a reduction of inflammatory
response and pain as well as better recovered skin morphology.
Conclusions
Based on our observation, we can conclude that PBMT can be
proposed as a promising therapy to be used in the management
of cutaneous fibrosis, likely in combination with pre-existing
treatments. Patient consent statement: the patients’ informed consent
was acquired for all patients involved in the study.
References
Citation
Orlandi C, Purpura V, Melandri D. Blue Led Light in Burns: A New Treatment’s Modality. J Clin Investigat Dermatol. 2021;9(2): 5